Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
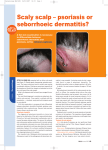
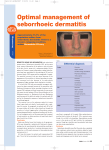
HIV AND THE SKIN Seborrhoeic dermatitis Only 1-3% of the general population have seborrhoeic dermatitis compared with 20-85% of patients with HIV. Seborrhoeic dermatitis is commoner in seropositive than in seronegative homosexual men. its severity is increased at CD4 T-cell counts below 100 .Itchy, scaly patches are found at the classical sites for seborrhoeic dermatitis. Management follows conventional lines: emollients, topical steroids and antifungals and oral imidazoles. Drug reactions Of patients with Pneumocystis jiroveci pneumonia treated with co-trimoxazole, 60% experience fever, nausea, vomiting and a rash. Xerosis and cheilitis are common with PIs. Lipodystrophy, retinoid-like effects particularly indinavir-paronychia, periungual pyogenic granuloma-like lesions, xerosis and cheilitis, and curly hair Zidovudine:trichomegaly, alopecia,nail Pigmentation, Longitudinal melanonychia Bacilary angiomatosis caused by the Gram-negative cat-scratch disease organism Bartonella (previously Rochalimaea) henselae affecting the skin. presents with purple, papular and nodular vascular lesions resembling KS. Diagnosis is achieved by skin biopsy. Bacillary angiomatosis responds to oral erythromycin in most patients; isoniazid, rifampicin, ethambutol or clofazimine, either in addition to or instead of erythromycin, have also been used. Candidosis. Oral candidosis has classically been associated with immunosuppressive states and was one of the first features to be recognized in the early days of the HIV epidemic before the syndrome was clearly defined and the causative agent identified. Oesophageal candidosis is an AIDS-defining diagnosis. Scabies has been endemic in the HIV population and there are occasional epidemic outbreaks on HIV wards, in hospices and in the community. Transmission is by sexual intercourse, nursing, comforting and massage. Norwegian/crusted scabies is highly contagious and its diagnosis should arouse suspicion of underlying HIV infection. Kaposi's sarcoma KS is caused by infection with human herpes virus (HHV)-8 (KSHV). It is probably transmitted sexually, more by the faecooral route or the ejaculate than by blood, in HIV-positive homosexual men. HIV / AIDS-related KS may be a disseminated disease with gastrointestinal and pulmonary involvement. Cutaneous KS is multicentric and often involves the face, oral mucosa, palate and genitalia. Oropharynx Distressing mouth ulceration occurs frequently. The differential diagnosis includes malignancy (KS and lymphoma), HSV,CMV, fungal infections, Behcet's disease, drug-induced ulceration(e,g. didanosisne-ddI, DDI), and idiopathic aphthous ulceration. Oral candidosis is very common in HIV-positive individuals and almost universal in AIDS. Hairy leukoplakia is a new clinical entity that has emerged during the HIV epidemic and is probably associated with EpsteinBarr virus infection. It is usually asymptomatic, although patients have often noticed the appearance of a roughened patch along the lateral margin of the tongue. is now known to occur in other immunocompromised people and has even been reported in healthy individuals.