Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
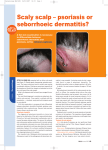
Forum Dermatology Treating scalp psoriasis in general practice Johnny Loughnane details the manifestations of psoriasis on and near the scalp, as well as how to best manage a condition that often impinges on quality of life Figure 1. Severe psoriasis can lead to alopecia. However, hair regrowth is usual with effective treatment Psoriasis is a common inflammatory dermatosis, affecting 2% of the population. Scalp involvement is common. Indeed, scalp involvement may be the only manifestation of the disease. It may be difficult to distinguish between psoriasis and dandruff or seborrhoeic dermatitis. Psoriasis usually presents with more well-demarcated, erythematous plaques covered with thick, silvery scales. Seborrhoeic dermatitis is less well demarcated and scales are finer and have a more greyish colour. Both conditions can itch. Scratching a psoriasis plaque lifts the surface scales, making their silvery colour more obvious. Picking off the silvery scales results in bleeding points, a finding known as the Auspitz sign. Psoriasis is one of those skin conditions that preferentially involves damaged skin, the so-called Koebner phenomenon. Many patients with dandruff/seborrhoeic dermatitis scratch their scalp. In psoriasis patients, the disease may Koebnerise to the scratched scalp. Indeed, many patients present with features of psoriasis and seborrhoeic dermatitis: socalled sebopsoriasis. Scalp psoriasis significantly impinges on quality of life: • It is a highly visible disease, especially when it spreads beyond the hair margins • There are problems with scales falling on clothing • There may be persistent itch • It is traditionally difficult and messy to treat. Treatment has to include a thick coverage of scalp hair. This is difficult to achieve with creams, ointments and especially pomades. Patient compliance and tolerability can play a crucial role in efficacy. Therefore, when it comes to treatment, choice of vehicle can be as important as the choice of therapy itself. Topical corticosteroids have been widely used in general practice. Steroids are effective thanks to their antiinflammatory action. There are two problems with steroid applications when used as sole therapy. Firstly, they are Figure 2 and 3. Psoriasis of the hair margin and ears before and after treatment with Eumovate ointment in the morning an Silkis in the evening usually only partially effective. Secondly, continued use over a period of time gives less and less of a response, ie. tachyphylaxis. Traditional tar and dithranol treatments are just not used in general practice due to their messiness and side-effect profile. Two approaches have been adopted in an attempt to improve acceptability and effectiveness of topical treatment: Reduce messiness of treatment Cocois contains tar and salicylic acid. It has a bit of a smell but is generally well tolerated. It is more effective if left on the scalp for longer than recommended by the manufacturers. It can be applied at night and washed out in the morning. A shower cap helps protect bedding. Combination treatments • Combine steroid and salicylic acid (Diprosalic scalp application): The salicylic acid is an excellent keratolytic and helps break down scale • Combine steroid and tar: Cocois can be applied, as above, at night. A steroid is applied after washing out Cocois in the morning FORUM February 2010 49 Scalp psoriasis-NH2* 1 28/01/2010 16:33:16 Forum Dermatology Treatment of scalp psoriasis Mild • Calcipotriol + betamethasone (Xamiol) • Tar shampoo • Topical steroid: betamethasone as scalp application or mousse • Topical steroid + salicylic acid (Diprosalic scalp application) Moderate • Calcipotriol/betamethasone (Xamiol) • Tar (Cocois) +/– betamethasone (Bettamousse/Betacap) Figure 4 and 5. Scalp psoriasis before and two weeks after daily Xamiol. Results with Xamiol are often much quicker than with traditional therapies. The gel is applied to the scalp at night and washed out in the morning. Some patients find that leaving the hair shampoo for a few minutes, before washing out, makes removal of the gel more effective • Combine steroid and a vitamin D analogue: calcipotriol (Dovonex) applied at night with a steroid in the morning has been used for many years. Applying even cosmetically acceptable applications to the scalp is difficult. Understandably, regimens needing twice daily treatments have a poor compliance record. A recent addition to our therapeutic options combines a Severe • Coal tar pomade • Refer steroid, betamethasone with a vitamin D analogue, calcipotriol (Xamiol). Psoriasis of the face and hair margin The hair margin is an important dividing line between the tougher skin of the scalp and the more delicate skin of the face. This has implications when treating psoriasis that extends beyond the hair margin: • Potent steroids will cause thinning of facial skin • Tar and vitamin D analogues may irritate facial skin. Calcitriol (Silkis) is less effective than calcipotriol (Dovonex) but appears less irritant on delicate skin, such as on the face. We therefore tend to combine a moderate potency steroid, clobetasone ointment (Eumovate), with calcitriol (Silkis). They should be applied at different times of the day. If this does not give an acceptable result one may try tacrolimus (Protopic). Tacrolimus is generally ineffective on chronic plaque psoriasis. However, on the thinner skin of the face it is effective in up to 90% of patients. Johnny Loughnane is in practice in Limerick Irish College of General Practitioners Place an advert free of charge on the ICGP website The ICGP Classifieds section allows members to place job adverts online, free of charge. GPs can advertise posts in their practice (short-term and long-term) or advertise their availability for work. GPs looking to pass on their practice or GPs looking to take over a practice can also post adverts. See www.icgp.ie/classifieds 50 FORUM February 2010 Scalp psoriasis-NH2* 2 28/01/2010 16:33:32