Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug interaction wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacogenomics wikipedia , lookup
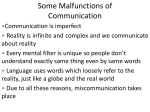
Population Science/Epidemiology Chlorthalidone Reduces Cardiovascular Events Compared With Hydrochlorothiazide A Retrospective Cohort Analysis Michael P. Dorsch, Brenda W. Gillespie, Steven R. Erickson, Barry E. Bleske, Alan B. Weder See Editorial Commentary, pp 665– 666 Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 Abstract—There is significant controversy around whether chlorthalidone (CTD) is superior to hydrochlorothiazide (HCTZ) in hypertension management. The objective of this analysis was to evaluate the effects of CTD compared with HCTZ on cardiovascular event (CVE) rates. We performed a retrospective observational cohort study from the Multiple Risk Factor Intervention Trial data set from the National Heart, Lung, and Blood Institute. The Multiple Risk Factor Intervention Trial was a cardiovascular primary prevention trial where participants were men 35 to 57 years of age enrolled and followed beginning in 1973. CVEs were measured yearly, and time to event was assessed by Cox regression. Systolic blood pressure, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglyceride, potassium, glucose, and uric acid were measured yearly. The difference between groups was evaluated by repeated-measures mixed modeling, and each model was adjusted for predictors of each variable. CVEs were significantly lower in those on CTD (adjusted hazard ratio: 0.51 [95% CI: 0.43 to 0.61]; P⬍0.0001) and on HCTZ (adjusted hazard ratio: 0.65 [95% CI: 0.55 to 0.75]; P⬍0.0001) compared with those who took neither drug. When comparing the 2 drugs, CTD had significantly fewer CVEs compared with HCTZ (P⫽0.0016). CTD displayed significantly lower SBP (P⬍0.0001), lower total cholesterol (P⬍0.0001), lower low-density lipoprotein cholesterol (P⫽0.0009), lower potassium (P⫽0.0003), and higher uric acid (P⬍0.0001) over time compared with HCTZ. In conclusion, both HCTZ and CTD reduce CVEs compared with neither drug. When comparing both drugs, CTD reduces CVEs more than HCTZ, suggesting that CTD may be the preferred thiazide-type diuretic for hypertension in patients at high risk of CVEs. (Hypertension. 2011;57:689-694.) ● Online Data Supplement Key Words: chlorthalidone 䡲 hydrochlorothiazide 䡲 hypertension 䡲 thiazide diuretic 䡲 antihypertensive agents T pamide. The choice between HCTZ and CTD for the treatment of hypertension is controversial and has recently been a topic of editorials, meta-analyses, and reviews.3–7 CTD may have superior 24-hour blood pressure control compared with HCTZ.8 There are also several studies that demonstrate the efficacy of both CTD and HCTZ,9 –15 but one recent clinical trial has led some to question the effectiveness of HCTZ.16 The Multiple Risk Factor Intervention Trial (MRFIT) was a large primary prevention trial that began in 1973.17 It was the first study to hint that CTD may be superior to HCTZ. In 1980, the MRFIT Policy Advisory Board changed the hypertension treatment protocol, recommending CTD over HCTZ for initial hypertension therapy.13 This was done because the coronary heart disease (CHD) mortality of special intervention clinics using HCTZ was 44% higher than other clinics (P⫽0.23). The MRFIT data set provides the opportunity to hiazide-type diuretics are recommended as a primary choice for the treatment of hypertension.1 In the case of uncomplicated hypertension, without the presence of comorbid conditions that would benefit from another class of antihypertensive drug, the thiazide-type diuretics are considered one of the initial agents to use. If not used as initial therapy, thiazide-type diuretics are recommended as the next agent added to existing therapy, should more aggressive treatment be desired. Clinicians have several options when prescribing a thiazide-type diuretic. The most commonly prescribed thiazide-type diuretic is hydrochlorothiazide (HCTZ).2 This agent is listed 9 different times as HCTZ or as 1 of 2 agents in a combination drug in the 2008 top 200 drugs prescribed in the United States. Other thiazide-type diuretics include chlorthalidone (CTD), chlorothiazide, metolazone, and inda- Received August 18, 2010; first decision September 7, 2010; revision accepted January 31, 2011. From the University of Michigan Health System (M.P.D.), Ann Arbor, MI; School of Public Health (B.W.G.), College of Pharmacy (S.R.E., B.E.B.), and Medical School (A.B.W.), University of Michigan, Ann Arbor, MI. This article was prepared using a limited access data set obtained from the National Heart, Lung, and Blood Institute and does not necessarily reflect the opinions or views of the MRFIT or the National Heart, Lung, and Blood Institute. Correspondence to Michael P. Dorsch, University of Michigan Health Systems, B2D301 SPC 5008, 1500 East Medical Center Dr, Ann Arbor, MI 48109-5008. E-mail [email protected] © 2011 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.110.161505 689 690 Hypertension April 2011 directly compare HCTZ and CTD, because the documentation of these drugs was done at each follow-up visit. The objective of the current analysis was to evaluate the cardiovascular end points between patients who took HCTZ and CTD. The secondary objective was to compare the change in systolic blood pressure (SBP), total cholesterol (TC), lowdensity lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglyceride, potassium, glucose, and uric acid of patients in the 2 groups. Methods Design Overview Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 We performed a retrospective observational cohort analysis comparing the clinical effects of CTD with HCTZ. Data for this analysis were collected as part of the MRFIT, which was a randomized cardiovascular primary prevention trial in 12 866 men, 35 to 57 years of age, who were enrolled and followed beginning in 1973. The study tested whether a multifaceted intervention program could reduce mortality from CHD. The specifics of the study have been published previously.17 Briefly, patients were randomized to a special intervention group consisting of treatment for hypertension, smoking cessation counseling, and dietary guidance or to usual care from their healthcare provider with follow-up of 7 years. The hypertension intervention involved a stepped-care approach, which began with HCTZ or CTD at either 50 or 100 mg daily, with weight and sodium reduction. The steps that followed were to add antiadrenergic drug therapy, an arteriolar vasodilator, and then guanethidine in step 4. The goal blood pressure was a diastolic blood pressure of 89 mm Hg or 10-mm Hg less than the average diastolic blood pressure at that visit, whichever is lower. The use of CTD and HCTZ was assessed by interview at each follow-up visit for 7 years, along with many other clinical variables. Our analysis was approved by the University of Michigan Institutional Review Board. Patient Population Eligible patients for the MRFIT were in the upper 15% of risk for death from CHD based on risk factors of elevated cholesterol, elevated diastolic blood pressure, and cigarette smoking from the Framingham Heart Study. Patients also could not have had preexisting, definite clinical CHD before entering the study. Exposure Definition The use of CTD or HCTZ was considered first line therapy for the hypertension intervention in the MRFIT. Use of either CTD or HCTZ was documented yearly. It was assumed that if the patient indicated taking the diuretic at the follow-up assessment, they had taken the medication in the year before that visit. This exposure was then used as a time-dependent variable to include all of the follow-up time points in which patients were exposed to either drug. Based on the time-dependent nature of this analysis, an individual patient could cross over from one drug group to the other over time. If a patient reported stopping either drug during the follow-up, then those time points were defined as “stopped drug.” This definition of exposure was undertaken to capture the cross over that is seen in the data set. Figure 1 provides further explanation. For the secondary outcomes, the exposure was defined as those patients who stated adherence to either CTD or HCTZ for 6 of the 7 yearly visits. Outcome Measures The full Outcome Measures section defining each end point is described in the online Data Supplement (please see http://hyper. ahajournals.org). The primary outcome of this analysis was cardiovascular events that were adjudicated and prespecified in the MRFIT data set. Nonfatal events consisted of clinical myocardial infarction (MI), MI determined by annual ECG, stroke, coronary artery bypass surgery, ECG-defined left ventricular hypertrophy, heart failure, angina determined by Rose questionnaire, and peripheral artery Year 1 Year 2 Year 3 Year 4 Figure 1. Exposure definition for the primary analysis. The dashed line is CTD, the dotted line is HCTZ, and the solid line is when one of the drugs was stopped. Patients were not entered into the data set until the first exposure to CTD or HCTZ. As seen, this example patient did not enter into the data set until year 2. Year 2 exposure was considered CTD. During year 3, the patient stopped taking CTD and was considered stopped drug for year 3. Year 4 was then considered HCTZ. occlusive disease. Nonfatal CVEs were documented at the yearly follow-up in the MRFIT data set; the specific dates of each event were not recorded. Cause-specific mortality is based on death certificates coded by trained nosologists using the International Classification of Diseases, 9th Revision. The study personnel adjudicated these cardiovascular deaths to be caused by coronary surgery, congestive heart failure, sudden death, MI, hypertension with renal failure, hypertension with left ventricular failure, stroke, and other cardiovascular disease. Secondary outcomes were the change in SBP, TC, LDL cholesterol, HDL cholesterol, triglyceride, potassium, glucose, and uric acid at each time point of follow-up between CTD and HCTZ. Statistical Analysis The primary outcome was the time from first follow-up documenting CTD or HCTZ exposure during the study to the first cardiovascular event. A time-to-event analysis was performed using Cox regression, stratifying by the MRFIT follow-up clinic. The covariates of primary interest were the prescription of CTD, HCTZ, or neither drug, entered in the model as time-dependent covariates. This method allowed us to define exposure at each time point for a specific patient and examine the events when patients were in that exposure time. Models were adjusted for baseline age, race, smoking status, MRFIT randomized group, diuretic dose, SBP, LDL, HDL, and baseline hypertension treatment, which are either known predictors of CVEs or had significant treatment imbalance at baseline. Patients without an event were censored at last follow-up. Secondary analyses were performed to investigate differences in the mean levels of SBP, TC, LDL, HDL, triglyceride, potassium, glucose, and uric acid between those on CTD versus HCTZ over time. Mixed-model analyses controlling for baseline predictors for each variable were used with a random slope and intercept for each patient. Tests for a difference between those on CTD versus HCTZ were performed overall, as well as at each time point. All of the statistical analyses were performed using SAS software version 9.2 (SAS Institute, Inc). Results Of the 12 866 patients in the MRFIT, 6441 were initially prescribed either CTD (N⫽2392) or HCTZ (N⫽4049) with a median follow-up of 6 years. Seventy-five percent of the initial HCTZ patients and 76% of the initial CTD patients crossed over into either the other drug group or the drugstopped group. Of the initial HCTZ patients, 29% crossed over into the CTD group, whereas 37% of the initial CTD patients crossed over into the HCTZ group sometime during follow-up. Overall, 46% of the time patients were in the HCTZ group, 32% in the CTD group, and 23% in the stopped-drug group, accounting for 33 614 years of exposure among the 6441 patients. Baseline characteristics of patients based on the initial diuretic are presented in Table 1. There were no statistically significant baseline differences in demographics, cardiovascular risk factors, and metabolic parame- Dorsch et al Table 1. Baseline Demographics for Those Initially Receiving CTD and HCTZ Variables HCTZ (N⫽4049) CTD (N⫽2392) Age, y 46.9⫾5.9 46.7⫾5.7 0.1234 2740 (67.7) HTN MI Angina DM 1563 (65.3) 0.0647 8 (0.2) 5 (0.21) 0.9832 19 (0.47) 10 (0.42) 0.2113 77 (3.2) 0.9126 125 (3.1) LVH on ECG P 8 (0.2) 4 (0.17) 0.7854 Smoker 2242 (55.4) 1346 (56.3) 0.4827 Total cholesterol, mg/dL 249.5⫾36.4 249.3⫾35.8 0.8072 HDL, mg/dL 42.6⫾11.6 42.9⫾12.4 0.3779 LDL, mg/dL 156.5⫾35.2 156.8⫾35.6 0.7427 SBP, mm Hg 142.1⫾13.7 142.7⫾13.1 0.1119 Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 Serum creatinine, mg/dL 1.11⫾0.152 Glucose, mg/dL 99.6⫾15.7 Potassium, mEq/L 1.10⫾0.152 100.3⫾14.5 0.2497 0.0986 4.4⫾0.5 4.4⫾0.5 0.9959 27.8⫾3.5 27.8⫾3.4 0.7393 ⬎50 mg 1149 (28.4) 1145 (47.9) ⬍0.0001 ⱕ50 mg 2900 (71.6) 1247 (52.1) White 3535 (87.3) 2116 (88.5) 0.1718 Black 385 (9.5) 213 (8.9) 0.4198 BMI, kg/m2 Dose Race Other 129 (3.2) 63 (2.6) 1814 (44.8) 2007 (83.9) ⬍0.0001 Any HTN medication 1406 (34.7) 697 (29.1) ⬍0.0001 Diuretic 1291 (31.2) 627 (26.2) ⬍0.0001 3 (0.07) 3 (0.13) 0.2249 564 (13.9) 242 (10.1) ⬍0.0001 MRFIT intervention, n (%) 0.2080 Medications Ganglionic blockers Methyldopa HTN indicates hypertension; DM, diabetes mellitus; LVH, left ventricular hypertrophy; SBP, systolic blood pressure; BMI, body mass index. Values are represented as mean⫾SD or n (%). P values were calculated by Student t test for age, total cholesterol, HDL, LDL, SBP, serum creatinine, glucose, potassium, and BMI, whereas all others were calculated by 2 or Fisher exact test. ters. However, significantly more CTD patients were randomized to the MRFIT intervention than the control and were taking higher doses of a thiazide-type diuretic. The HCTZ group had a significantly greater proportion of patients receiving hypertensive drug therapy at baseline. A total of 1244 cardiovascular events were documented over the 7 years of follow-up. Cardiovascular Events CVEs were significantly lower in those on CTD (adjusted hazard ratio [aHR]: 0.51 [95% CI: 0.43 to 0.61]; P⬍0.0001) and on HCTZ (aHR: 0.65 [95% CI: 0.55 to 0.75]; P⬍0.0001) compared with those on neither drug, adjusting for baseline age, race, smoking status, MRFIT randomized intervention group, diuretic dose, SBP, LDL, HDL, and hypertension treatment. When comparing the 2 drugs, those on CTD had significantly fewer CVEs compared with those on HCTZ CTD Reduces CVEs Compared With HCTZ 691 (aHR: 0.79 [95% CI: 0.68 to 0.92]; P⫽0.0016). Figure 2 displays the adjusted event-free probabilities for each group over time for a subject with the covariate values specified in the Figure 2 legend. The adjusted HR for each individual component of the composite primary outcome is represented in Table 2. The individual events that contributed most importantly to the difference between HCTZ and CTD were clinical MI, ECG MI, coronary artery bypass, Rose angina, and peripheral artery occlusive disease. The unadjusted estimates of the individual components of the composite primary outcome are available in the online Data Supplement Table S1 (please see http://hyper.ahajournals.org). Interactions among the drug variables, the MRFIT intervention groups, and time were tested. The MRFIT intervention significantly altered the effects of the drugs (drug by study intervention interaction P⫽0.0003). The MRFIT intervention group enhanced the effect of CTD compared with no drug in the intervention group (aHR: 0.47 [95% CI: 0.38 to 0.60]; P⬍0.0001), and the corresponding effect of HCTZ was similar to the main effects compared with no drug (aHR: 0.67 [95% CI: 0.53 to 0.84]; P⫽0.0006). Within the MRFIT intervention, those on CTD had fewer events than those on HCTZ, but the difference was not statistically significant (aHR: 0.79 [95% CI: 0.59 to 1.08]; P⫽0.15). There was also a significant interaction among drug, MRFIT intervention, and time. Over time, the initial hazard reduction seen with both drug groups diminished significantly (HCTZ by time interaction aHR: 1.19 [95% CI: 1.08 to 1.32], P⫽0.0004; CTD by time interaction aHR: 1.15 [95% CI: 1.03 to 1.27], P⫽0.01). Those in the MRFIT intervention group receiving CTD had significant reductions in CVE compared with those on neither drug at year 1 (aHR: 0.29 [95% CI: 0.19 to 0.44]; P⬍0.0001) and 3 (aHR: 0.38 [95% CI: 0.29 to 0.50]; P⬍0.0001). Those in the MRFIT intervention group receiving HCTZ had significant reductions in CVE compared with those on neither drug at year 1 (aHR: 0.38 [95% CI: 0.26 to 0.56]; P⬍0.0001) and 3 (aHR: 0.54 [95% CI: 0.42 to 0.70]; P⬍0.0001). Differential Effects of CTD Compared With HCTZ Figure 3 shows each variable over time adjusted for baseline predictors with asterisks delineating the time points that are significantly different between groups. In the longitudinal models comparing CTD with HCTZ over time, CTD patients displayed significantly lower SBP (overall P⬍0.0001), TC (overall P⬍0.0001), LDL (overall P⫽0.0009), and serum potassium (overall P⫽0.0003) and higher uric acid over time (overall P⬍0.0001) compared with HCTZ. Glucose over time (overall P⫽0.1595) and triglyceride over time (overall P⫽0.2648) did not differ between the groups. The specific values are available in the online Data Supplement Table S2. Discussion Based on a post hoc analysis of a primary prevention study, currently the only study that allows for direct comparison between HCTZ and CTD on cardiovascular outcomes, we were able to demonstrate that CTD significantly reduced CVEs as compared with HCTZ. This finding is analogous to 692 Hypertension April 2011 1.0 0.9 Event Free Probability 0.8 0.7 0.85 0.6 0.80 0.5 0.75 0.4 0.70 0.3 6.0 6.5 7.0 0.2 CTD HCTZ Drug Stopped 0.1 CTD versus Stopped Drug HR 0.51; 95% CI 0.43-0.61; p<0.0001 HCTZ versus Stopped Drug HR 0.64; 95% CI 0.55-0.75; p<0.0001 CTD versus HCTZ HR 0.79; 95% CI 0.68-0.92; p=0.0016 0 Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.5 Time (years) Figure 2. Adjusted event-free probability of CVEs. The hazard ratio was estimated using the Cox model. Adjusted estimates were controlled for by age, race, smoking status, MRFIT randomized group, diuretic dose, SBP, LDL, HDL, and baseline hypertension treatment. the morality data after a 10.5-year follow-up from MRFIT.13 In March 1980, the CHD mortality of special intervention clinics using HCTZ was 44% higher than other clinics (P⫽0.23). This led to a change in study protocol to the use of CTD as the thiazide-type diuretic of choice. From April 1980, the rate of CHD mortality in those clinics decreased by 28% (P⫽0.04, for comparison of percentage difference in mortality in the 2 time points). The results from our study further enhance the notion that CTD may be the preferred thiazide-type diuretic for treatment of hypertension. Obviously, one question that needs to be addressed is why CTD showed better efficacy in reducing cardiovascular events as compared with HCTZ when both agents work in a pharmacologically similar fashion. Based on our findings, an answer may be that CTD at the doses studied is a more potent antihypertensive agent resulting in greater blood pressure lowering and better outcomes. Recent data in Table 2. the literature support our findings that CTD appears to lower SBP more than HCTZ.8 Another reason why patients in the CTD group had improved outcomes may relate to metabolic profile of the drugs. When evaluating the metabolic profile, the CTD group had lower LDL and glucose values as compared with the HCTZ group. The lower the LDL levels the greater the chance of reducing cardiovascular events. Similarly, impaired glucose tolerance may also contribute to cardiovascular disease. The trends in glucose values were higher in the HCTZ group compared with the CTD group. The reason for the improved metabolic profile seen in the CTD group is not known. However, more CTD patients were in the study intervention group where lifestyle interventions were performed. We controlled for this intervention within our models, but there may have been residual effects that were not accounted for by that covariate. In contrast to these positive aHRs for Each Component of the Composite End Point CTD vs Drug Stopped Variables HR (95% CI) P HCTZ vs Drug Stopped HR (95% CI) P CTD vs HCTZ, P Cardiovascular death 0.33 (0.13 to 0.82) 0.0174 0.38 (0.17 to 0.84) 0.0163 0.6959 Clinical MI 0.13 (0.08 to 0.21) ⬍0.0001 0.34 (0.24 to 0.47) ⬍0.0001 0.0001 0.0103 ECG MI 0.26 (0.16 to 0.42) ⬍0.0001 0.49 (0.33 to 0.71) 0.0002 Stroke 0.55 (0.21 to 1.43) 0.2192 0.73 (0.32 to 1.67) 0.4493 0.4837 CABG 0.19 (0.12 to 0.30) ⬍0.0001 0.45 (0.33 to 0.62) ⬍0.0001 0.0001 ECG LVH 0.65 (0.38 to 1.10) 0.1088 0.62 (0.39 to 0.97) 0.0367 0.8114 Rose angina 0.52 (0.40 to 0.67) ⬍0.0001 0.71 (0.57 to 0.88) 0.0019 0.0029 CHF 0.28 (0.03 to 2.87) 0.2854 0.25 (0.06 to 1.045) 0.0575 0.9229 PAOD 0.75 (0.44 to 1.27) 0.2765 1.24 (0.78 to 1.95) 0.3662 0.0218 The hazard ratios were estimated using the Cox model. All of the variables were controlled for by age, race, smoking status, MRFIT randomized group, diuretic dose, SBP, LDL, HDL, and baseline HTN treatment. There can be overlap in events. CABG indicates coronary artery bypass; CHF, congestive heart failure; PAOD, peripheral artery occlusive disease; LVH, left ventricular hypertrophy. Dorsch et al A 144 142 * D 162 HCTZ CTD Overall p<0.0001 CTD Reduces CVEs Compared With HCTZ 140 HCTZ CTD Overall p=0.0009 160 693 158 138 SBP (mmHg) * 134 132 130 * 128 * * LDL (mg/dL) 156 136 * 126 150 148 122 144 120 142 118 140 0 112 1 2 3 4 Years 5 6 0 7 E HCTZ CTD 4.6 1 2 3 Years 4 5 6 Overall p=0.0003 4.5 HCTZ CTD 4.4 4.3 Potassium (mEq/L) * 108 106 104 102 * 4.2 4.1 * * * * * 3 4 Years 5 6 4.0 * 3.9 3.8 3.7 100 3.6 3.5 98 3.4 0 255 1 2 3 4 Years 5 6 0 7 F Overall p<0.0001 HCTZ CTD * 245 240 7.7 1 * * 235 7 HCTZ CTD Overall p=0.0001 * 7.5 * 2 7.6 250 Uric Acid (mg/dL) C Total Cholesterol (mg/dL) Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 Overall p=0.1595 110 Glucose (mg/dL) 152 146 124 B * 154 * 230 7.4 * 7.3 7.2 225 7.1 220 7.0 215 0 1 2 3 4 Years 5 6 7 0 1 2 3 4 Years 5 6 7 Figure 3. Effects of CTD vs HCTZ over time. Adjusted values were estimated using mixed models and represented as mean⫾SEM. Asterisks (*) represent P⬍0.05. The overall P value in each figure is the drug-by-time interaction. SBP was adjusted by age, diuretic dose, diagnosis of hypertension, and MRFIT randomization group. Glucose was adjusted by age, diuretic dose, body mass index, and diagnosis of diabetes. TC and LDL were adjusted by diuretic dose and the MRFIT randomization group. Potassium was adjusted by age, diuretic dose, and MRFIT randomization group. Uric acid was adjusted by diuretic dose and the diagnosis of diabetes mellitus. findings, the CTD group had lower potassium levels and higher uric acid levels. The reason for these findings may again relate to the potency of CTD and the doses used in the study. Despite the lower potassium levels and higher uric acid levels, increases in events were not seen in the CTD group. These findings are consistent with a previous MRFIT subgroup analysis in patients with baseline rest ECG abnormalities, suggesting that hypokalemia did not contributed to 694 Hypertension April 2011 Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 coronary artery disease mortality rate in the special intervention group at 48 months of follow-up.12 Other reasons for improved outcomes with CTD may relate to differences in pharmacokinetic and pharmacodynamic properties between CTD and HCTZ. With regard to pharmacokinetics, the half-life of CTD (45 to 60 hours) is much longer than the half-life of HCTZ (16 to 24 hours), and CTD has a larger volume of distribution. In addition, CTD is thought to be 1.5 to 2.0 times more potent than HCTZ, with 24-hour ambulatory blood pressure monitoring demonstrating lower blood pressure with CTD during the nighttime hours.8 Furthermore, a recent meta-analysis also suggested that CTD has greater effects on systolic blood pressure reductions as compared with HCTZ.5 Greater systolic blood pressure reductions in concert with more consistent effects over 24 hours with the use of CTD may have contributed to our study findings. There are inherent limitations in an observational study design, in that we cannot exclude unmeasured confounding, selection bias, and information bias that may have occurred during the study. Unmeasured confounding could exist, because the treating physician determined antihypertensive drug selection, and we could not determine why HCTZ or CTD was chosen as initial therapy or why patients switched from one drug to another. We have attempted to reduce selection bias by comparing the HCTZ and CTD groups in a time-dependent fashion to a time period when people stopped taking either drug; we believe that this gives more strength to the conclusions of this analysis. Another limitation to this analysis is that we could access only the data collected in MRFIT. The nonfatal events were only documented during each yearly follow-up so the exact time of each event is not known. We hope that defining drug exposure for the year before the documented event limits bias for each group studied. Also, data on why patients stopped taking CTD or HCTZ are unavailable and may pose information bias. Despite these limitations, our finding that both the HCTZ and CTD groups have better outcomes as compared with the stopped drug group gives a measure confidence in our approach to the data. Perspectives Our study demonstrates that both HCTZ and CTD reduce CVEs compared with neither drug. When comparing both drugs, CTD reduces CVEs more than HCTZ, suggesting that CTD may be the preferred thiazide-type diuretic for hypertension in patients at high risk of cardiovascular events. Prospective randomized, controlled trials are needed to confirm the effects on clinical end points, because this class of medications is so commonly prescribed for hypertension. Sources of Funding The MRFIT Study was conducted and supported by the National Institutes of Health/National Heart, Lung, and Blood Institute in collaboration with the MRFIT Study Investigators. This manuscript was prepared using a limited access dataset obtained from the NHLBI and does not necessarily reflect the opinions or views of the MRFIT or the NHLBI. Disclosures None. References 1. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ, for the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206 –1252. 2. Lamb E. Top 200 prescription drugs of 2008. Pharmacy Times Web site. May 2009. Available at: http://www.pharmacytimes.com/issue/ pharmacy/2009/2009-05/RxFocusTop200Drugs-0509. Accessed April 10, 2010. 3. Pitt B. The role of chlorthalidone in patients with high-risk hypertension. J Clin Hypertens (Greenwich). 2009;11:460 – 461. 4. Ernst ME, Carter BL, Basile JN. All thiazide-like diuretics are not chlorthalidone: putting the ACCOMPLISH Study into perspective. J Clin Hypertens (Greenwich). 2009;11:5–10. 5. Ernst ME, Carter BL, Zheng S, Grimm RH Jr. Meta-analysis of doseresponse characteristics of hydrochlorothiazide and chlorthalidone: effects on systolic blood pressure and potassium. Am J Hypertens. 2010; 23:440 – 446. 6. Sica DA. Chlorthalidone: a renaissance in use? Expert Opin Pharmacother. 2009;10:2037–2039. 7. Kaplan NM. The choice of thiazide diuretics: why chlorthalidone may replace hydrochlorothiazide. Hypertension. 2009;54:951–953. 8. Ernst ME, Carter BL, Goerdt CJ, Steffensmeier JJ, Phillips BB, Zimmerman MB, Bergus GR. Comparative antihypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension. 2006;47:352–358. 9. Amery A, Birkenhger W, Brixko P, Bulpitt C, Clement D, Deruyttere M, De Schaepdryver A, Dollery C, Fagard R, Forette F. Mortality and morbidity results from the European Working Party on High Blood Pressure in the Elderly Trial. The Lancet. 1985;1:1349 –1354. 10. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial: major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic. JAMA. 2002;288:2981–2997. 11. Hypertension Detection and Follow-up Program Cooperative Group. Five-year findings of the hypertension detection and follow-up program: reduction in mortality of persons with high blood pressure, including mild hypertension. JAMA. 1979;242:2562–2571. 12. Multiple Risk Factor Intervention Trial Research Group. Baseline rest electrocardiographic abnormalities, antihypertensive treatment, and mortality in the multiple risk factor intervention trial. Am J Cardiol. 1985; 55:1–15. 13. Multiple Risk Factor Intervention Trial Research Group. Mortality after 10 1/2 years for hypertensive participants in the Multiple Risk Factor Intervention Trial. Circulation. 1990;82:1616 –1628. 14. SHEP cooperative research group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA. 1991;265:3255–3264. 15. MRC working party. Medical research council trial of treatment of hypertension in older adults: principal results. BMJ. 1992;304:405– 412. 16. Jamerson K, Weber M, Bakris G, Dahlf B, Pitt B, Shi V, Hester A, Gupte J, Gatlin M, Velazquez E. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med. 2008;359: 2417–2428. 17. Multiple Risk Factor Intervention Trial Research Group. Coronary heart disease death, nonfatal acute myocardial infarction and other clinical outcomes in the multiple risk factor intervention trial. Am J Cardiol. 1986;58:1–13. Chlorthalidone Reduces Cardiovascular Events Compared With Hydrochlorothiazide: A Retrospective Cohort Analysis Michael P. Dorsch, Brenda W. Gillespie, Steven R. Erickson, Barry E. Bleske and Alan B. Weder Downloaded from http://hyper.ahajournals.org/ by guest on April 30, 2017 Hypertension. 2011;57:689-694; originally published online March 7, 2011; doi: 10.1161/HYPERTENSIONAHA.110.161505 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2011 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/57/4/689 Data Supplement (unedited) at: http://hyper.ahajournals.org/content/suppl/2011/03/04/HYPERTENSIONAHA.110.161505.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/ ONLINE DATA SUPPLEMENT Chlorthalidone reduces cardiovascular events compared to hydrochlorothiazide: A retrospective cohort analysis. Short title: CTD reduces CV events compared to HCTZ Michael P. Dorsch, Pharm.D., M.S., *‡ Brenda W. Gillespie, Ph.D., † Steven R. Erickson, Pharm.D., *‡ Barry E. Bleske, Pharm.D., *‡ Alan B. Weder, M.D. *§ From *University of Michigan Health System, †University of Michigan School of Public Health, ‡University of Michigan College of Pharmacy, and §University of Michigan Medical School, Ann Arbor, MI, USA. Reprint requests and correspondence: Michael P. Dorsch, Pharm.D., M.S. University of Michigan Health Systems B2D301 SPC 5008 1500 East Medical Center Drive Ann Arbor, MI 48109-5008 Email: [email protected] Phone: 734-763-5576 Fax 734-936-7027 1 Methods Outcome Measures The primary outcome of this analysis was cardiovascular events that were adjudicated and pre-specified in the MRFIT dataset. Non-fatal events consisted of clinical myocardial infarction (MI), MI determined by annual electrocardiogram (ECG), stroke, coronary artery bypass (CABG) surgery, ECG defined left ventricular hypertrophy (LVH), heart failure (HF), angina determined by Rose questionnaire, and peripheral artery occlusive disease (PAOD). Clinical MI was defined as an admission for MI based on review of hospital records. The records, which included admission sheet, discharge summary, ECGs and laboratory reports were forwarded to the coordinating center where nurses abstracted them. If a cardiovascular diagnosis was recorded in the chart, the records were reviewed by a cardiologist who evaluated the data in 3 categories of evidence for MI: history, serum enzyme levels, and ECGs. Each category was classified as strong, moderate, weak, or no evidence of MI. Definite MI required strong evidence in at least one category and strong or moderate evidence in a second category. The cardiologist diagnosis was compared to a computer algorithm of abstracted data. Discordant cases were assessed by two cardiologists, who reached a consensus on the diagnosis. The diagnosis of ECG MI required both of the following conditions: change in Minnesota Code for Q-QS patterns within any lead groups and significant change from the last screening ECG as judged by two cardiologists. ECG defined LVH was done by measurements made on standard 12-lead ECG. R-wave amplitude greater than 26 mm in either leads V5 or V6 or R-wave amplitude in V5 or V6 plus S or QS amplitude in V1 greater than 35 mm was diagnostic of ECG LVH. Stroke was diagnosed if hemiplegia or hemiparesis was present on physical exam. HF was defined by the presence of at least 2 major and 2 minor criteria. Major criteria were paroxysmal nocturnal 2 dyspnea, distended neck veins, rales in the presence of unexplained dyspnea, and S3 gallop. Minor criteria consisted of bilateral ankle edema, dyspnea on ordinary exertion, hepatomegaly, decrease in vital capacity by one-third from maximum record, and tachycardia. The Rose questionnaire, a standardized measure of angina, was performed to assess angina. A patient experiencing angina would respond that they have chest pain when walking up a hill, in a hurrying, or at a normal pace, if they stop or slow down when they get chest pain, if it goes away within 10 minutes of stopping or slowing down, and if the pain is located left sternum or left arm. PAOD was determined on physical exam if the patient had an absent or diminished femoral pulse with the presence of either a bruit, ischemic ulcers, surgery for peripheral arterial disease, or amputation of the lower limb. Non-fatal CV events were documented at the yearly follow-up in the MRFIT dataset; the specific dates of each event were not recorded. Cause-specific mortality is based on death certificates coded by trained nosologists using the Ninth Revision of the International Classification of Diseases (ICD-9). ICD-9 rubrics 410-414 and 429.2 are used to identify CHD deaths. ICD-9 code 429.2 identifies "cardiovascular disease, unspecified." The study personnel adjudicated these CV deaths to be caused by coronary surgery, congestive heart failure, sudden death, myocardial infarction, hypertension with renal failure, hypertension with LV failure, stroke, and other cardiovascular disease. Secondary outcomes were the change in SBP, TC, LDL cholesterol, HDL cholesterol, triglyceride, potassium, glucose, and uric acid at each time point of follow up between CTD and HCTZ. The standard mercury sphygmanometer was used to measure blood pressure. Sitting blood pressure was taken in a quiet room at each follow up visit. 3 Table S1: Unadjusted hazard ratios for each component of the composite endpoint CTD vs Variable CTD vs Drug Stopped HCTZ vs Drug Stopped HCTZ HR (95% CI) p-value HR (95% CI) p-value p-value CV Death 0.31 (0.13-0.74) 0.0083 0.38 (0.18-0.83) 0.0143 0.5640 Clinical MI 0.13 (0.08-0.21) <0.0001 0.35 (0.25-0.47) <0.0001 <0.0001 ECG MI 0.30 (0.18-0.48) <0.0001 0.51 (0.35-0.74) 0.0004 0.0221 Stroke 0.83 (0.32-2.15) 0.6961 1.21 (0.51-2.88) 0.6695 0.3115 CABG 0.21 (0.14-0.33) <0.0001 0.54 (0.40-0.73) <0.0001 <0.0001 ECG LVH 0.98 (0.60-1.59) 0.93 1.06 (0.68-1.63) 0.8029 0.7127 Rose Angina 0.66 (0.51-0.84) 0.0008 0.98 (0.79-1.22) 0.8504 <0.0001 CHF 0.13 (0.02-1.11) 0.062 0.28 (0.07-1.11) 0.0699 0.4829 PAOD 0.87 (0.52-1.46) 0.5873 1.56 (0.99-2.47) 0.0558 0.0038 4 Table S2: Values Represented in Figure 3. Effects of CTD versus HCTZ over time Adjusted values were estimated using mixed models. SBP was adjusted by age, diuretic dose, diagnosis of HTN, and MRFIT randomization group. Glucose was adjusted by age, diuretic dose, BMI, and diagnosis of diabetes. TC and LDL were adjusted by diuretic dose and the MRFIT randomization group. Potassium was adjusted by age, diuretic dose and MRFIT randomization group. Uric acid was adjusted by diuretic dose and the diagnosis of diabetes. SEM = Standard Error of the Mean S2A: SBP (mmHg) Year 0 1 2 3 4 5 6 7 HCTZ mean 135.98 132.81 130.53 128.43 127.97 127.83 127.51 128.28 CTD SEM 0.6429 0.5024 0.5164 0.5172 0.5213 0.5314 0.5456 0.6364 mean 140.82 130.49 126.72 125.75 125.9 125.48 126.84 127.26 p-value SEM 0.6724 0.5325 0.5487 0.5499 0.5521 0.5623 0.578 0.7066 <.0001 0.0022 <.0001 0.0004 0.0061 0.0022 0.3949 0.2824 S2B: Glucose (mg/dL) Year 0 1 2 3 4 5 6 7 HCTZ mean SEM 102.51 0.8348 99.1265 0.6629 100.11 0.7179 101.9 0.7656 104.01 0.8245 106.62 0.8965 108.72 0.9758 109.67 1.1412 CTD mean 103.29 99.0201 99.6077 100.84 102.36 103.59 106.25 107.13 p-value SEM 0.8717 0.7045 0.7632 0.8128 0.8738 0.9497 1.03 1.24 0.4302 0.916 0.6335 0.3438 0.1711 0.0202 0.0812 0.1326 5 S2C: TC (mg/dL) Year 0 1 2 3 4 5 6 7 HCTZ mean 249.6 241.48 240.06 237.88 236.46 234.75 234.66 233.59 CTD SEM 1.7067 1.4749 1.5111 1.5239 1.5396 1.5637 1.5925 1.7529 mean 251.67 235.17 234.6 234.1 231.93 228.39 231.98 231 p-value SEM 1.8039 1.5758 1.6155 1.6294 1.6431 1.6677 1.6994 1.9245 0.3724 0.0066 0.0189 0.1066 0.0555 0.0079 0.2697 0.3377 S2D: LDL (mg/dL) Year 0 2 4 6 HCTZ mean 157.17 151.46 147.27 146.84 CTD SEM 2.5295 1.6976 1.7091 1.7341 mean 156.74 145.52 144.01 143.88 p-value SEM 2.5901 1.794 1.7938 1.819 0.8475 0.0069 0.1382 0.1837 S2E: Potassium (mEq/L) Year 0 1 2 3 4 5 6 7 HCTZ mean 3.9499 4.1664 4.1218 4.0824 4.0739 4.0509 4.0292 3.9829 CTD SEM 0.02541 0.01997 0.02037 0.02038 0.02037 0.02076 0.02121 0.02553 mean 3.9232 3.9019 3.8511 3.8505 3.7919 3.7553 3.7502 3.7401 p-value SEM 0.03056 0.026 0.02602 0.02583 0.02612 0.02658 0.02684 0.03565 0.4126 <.0001 <.0001 <.0001 <.0001 <.0001 <.0001 <.0001 S2F: Uric Acid (mg/dL) Year HCTZ mean CTD SEM mean p-value SEM 6 0 1 2 3 4 5 6 7 7.306 7.3174 7.2391 7.1241 7.1835 7.1534 7.1942 7.1777 0.05755 0.04897 0.04839 0.04854 0.04922 0.05057 0.0525 0.06341 7.2998 7.5923 7.4402 7.2728 7.2222 7.2796 7.1941 7.2273 0.06016 0.05225 0.05249 0.05271 0.05326 0.05427 0.05584 0.07 0.9327 0.0001 0.0046 0.0371 0.5922 0.0882 0.9993 0.5998 7