Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Point mutation wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Frameshift mutation wikipedia , lookup
Population genetics wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Microevolution wikipedia , lookup
Genetic testing wikipedia , lookup
Public health genomics wikipedia , lookup
Down syndrome wikipedia , lookup
Medical genetics wikipedia , lookup
Genome (book) wikipedia , lookup
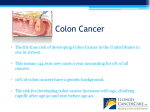
Lynch syndrome Developed by Dr. June Carroll, Ms. Shawna Morrison, Dr. Sean Blaine and Dr. Judith Allanson Last updated April 2014 Disclaimer • This presentation is for educational purposes only and should not be used as a substitute for clinical judgement. GEC-KO aims to aid the practicing clinician by providing informed opinions regarding genetic services that have been developed in a rigorous and evidence-based manner. Physicians must use their own clinical judgement in addition to published articles and the information presented herein. GEC-KO assumes no responsibility or liability resulting from the use of information contained herein. Objectives • Following this session the learner will be able to: – Refer to their local genetics centre and/or order genetic testing appropriately for Lynch syndrome (LS) – Discuss and address patient concerns regarding family history of LS – Find high quality genomics educational resources appropriate for primary care Case • Jane - healthy 26 year old • Office visit for a routine pap smear and renewal of birth control pills • Family History (any cancer in the family?) – Mother with breast cancer at 66 – Father’s side of the family: – uncle - CA kidney age 72 – uncle - CA colon age 56 – aunt - double primary: endometrial CA age 45, colon CA age 68 – 1 cousin - endometrial CA age 40 – 2 cousins - both have colon CA LEGEND Family history Kidney Colon Endometrial Breast Accident Mary Dx 45 CA Endometrial A&W Bob Dx 56 CA colon Stroke Nat Causes Steve Dx 72 Kevin, 67 CA Kidney A&W Paula Dx 66 CA- Br MI 72 A&W A&W A&W Dx 68 CA Colon Linda Dx 38 CA - colon Jeana Dx 40 Ca- Christa Dx 52 Endometrial CA – Colon Jane, 26 A&W A&W What is Lynch syndrome? • Lynch syndrome (LS), also known as Hereditary Non-Polyposis Colorectal Cancer, (HNPCC), is an inherited cancer predisposition syndrome • Individuals with LS have a greatly increased risk for certain cancers • LS accounts for about 0.7-3.6% of cases of CRC • Research on LS-related endometrial cancer is still emerging; current data suggest that in North America between 1.8% and 4.5% of cases are attributed to LS LYNCH SYNDROME-RELATED CANCERS Colorectal Endometrial Ovarian Pancreatic Ureter Brain Renal Gastric Small bowel Hepato-biliary Sebaceous (adenoma or carcinoma) What do I need to know about the genetics of Lynch syndrome? • Autosomal dominant • Reduced penetrance and variable expressivity Mismatch genes play an inherit important role in a cell’s to repair – not allrepair individuals who a mutation in ability a Lynch DNA damage as a cell grows and divides, by identifying and removing syndrome gene will develop cancer (reduced penetrance) single nucleotide mismatches, insertions and deletion loops. Defects in – signs symptoms/type and onset of cancerinwill the MMR and pathway lead to an accumulation of mutations a cellvary which maybetween result in aaffected malignancy family members (variable expressivity) • Caused by an inherited mutation in at least one of four mismatch repair (MMR) genes* (MLH1, MSH2, MSH6 or PMS2) or in EPCAM Who should be offered genetic testing? • Currently the decision to offer genetic testing is made in the setting of a genetics consult at a hereditary cancer program or a general genetics clinic • If possible, the affected individual in the family at highest risk to carry a mutation is offered testing first in order to maximize the likelihood of detecting a mutation – This would usually be a young individual with CRC or another Lynch syndrome-associated cancer Red Flags for hereditary cancer • There are multiple family members with cancer – Same side of family – Diagnoses occur at a younger than expected age – Several generations are affected • Clustering of certain types of cancers • Multiple primary cancers in same individual Family history Red Flags for a CRC syndrome • A patient is considered to be at high risk for Lynch syndrome (LS) if he/she has: – A known LS-causing mutation in the family OR – At least three relatives with an LS-associated cancer; the following criteria should also be present: • One must be a first degree relative of the other two; • At least two successive generations must be affected (autosomal dominant inheritance); • At least one relative with LS-related cancer should be diagnosed before age 50; – Tumour pathology should be verified when possible and other CRC syndromes should be ruled out What does the genetic test result mean? • If your patient has been found to carry a mutation in a Lynch syndrome gene (a positive result) – he/she has an increased lifetime risk to develop certain cancers – family members are at risk of carrying the same mutation and of having similar cancer risks • If a mutation is not identified and testing was for a known familial mutation (true negative) – Your patient is not considered to be at increased risk of developing hereditary cancer • If a mutation is not identified in an affected patient who has no known familial mutation (uninformative result) or when a variant of uncertain significance (VUS) is identified – The diagnosis of Lynch syndrome is not confirmed or ruled out, even in families with a strong history of CRC A VUS is a gene change that has not yet been classified as pathogenic or benign Cancer type Colorectal Endometrial Stomach Ovarian Hepato-biliary tract Urinary tract (ureter and renal pelvis) Small bowel Brain/ central nervous system Sebaceous neoplasm Pancreas Lynch syndrome lifetime cancer risk (carrier of a MLH1 or MSH2 gene mutation) General Population lifetime cancer risk to age 70 Risk Mean age at diagnosis Risk 52-82% 25-60% 6-13% 4-12% 44-61 years 48-62 years 56 years 42.5 years 5.5% 2.7% <1% 1% 1-4% 1-4% Not yet reported 55 years <1% <1% 3-6% 1-3% 49 years 50 years <1% <1% 1-9% 1-6% Not yet reported Not yet reported <1% <1% How do I order the genetic test? • Genetic testing is generally performed on a blood sample • Specifics will depend on your region. Details can be found at www.geneticseducation.ca How will genetic testing help you and your patient? • Positive result: – Clinical intervention may improve outcome – Family members at risk can be identified – Positive health behaviour can be reinforced – Reduction of uncertainty • True negative: – Avoidance of unnecessary clinical interventions – Emotional - relief – Children can be reassured Are there harms or limitations of genetic testing? • Positive result: – Adverse psychological reaction – Family issues/distress – Uncertainty - incomplete penetrance – Interventions may carry risk – Discrimination • Job, insurance – Privacy, confidentiality • True negative: – Adverse psychological reaction (i.e. survivor guilt) – Dysfunctional family dynamics – Complacent attitude to health • Uncertain result: – Complacent attitude to health – Uncertainty – Continued anxiety Screening and surveillance • In general, for high risk individuals (carriers of a Lynch syndrome gene mutation and their first degree relatives who have not yet had genetic testing): • Colorectal Cancer – Colonoscopy every 1-2 years beginning between ages 20 and 25 or 2-5 years prior to the earliest colon cancer in the family if that diagnosis was made before age 25 years, whichever is earlier • Endometrial and Ovarian cancer – Education about the symptoms of endometrial cancer – Annual transvaginal ultrasound and endometrial biopsy (limited evidence) – Prophylactic hysterectomy and bilateral salpingo-oophorectomy (for women who have completed childbearing) • Other Extracolonic cancers – Family history dependent Screening and surveillance • For patients who have a known mutation in a Lynch syndrome gene – Genetics healthcare provider or oncologist may provide recommendations specific to the patient and his/her family history • For patients who have a true negative result – Provincial guidelines for population risk CRC screening should be followed i.e. Fecal Occult Blood Test every two years from age 50 – For those individuals who have a family history of CRC unrelated to the mutation in their family (i.e. on the other side of the family), screening recommendations would be based on family history. • For patients with an uninformative result or a VUS – Recommendations will be based on a combination of factors, such as family history and, in cases where a VUS was identified, information about the VUS VUS – Variant of uncertain significance Screening and surveillance • Screening recommendations for individuals at increased risk to develop CRC and who do not meet high risk, Lynch syndrome criteria Criteria Recommendation One 1st degree relative with a CRC diagnosis less than age 50 (older than age 35) Colonoscopy beginning at age 40 OR 10 years younger than the youngest CRC diagnosis. Repeat every 3-5 years depending on family history and findings. OR Two 1st degree relatives with CRC diagnoses at any age A 1st degree relative with a CRC diagnosis at age 50 or older Colonoscopy beginning at age 50 OR 10 years younger than the earliest CRC diagnosis. Repeat every 5 years, depending on family history and findings. One 2nd degree relative with a CRC diagnosis less than age 50 Colonoscopy beginning at age 50. Repeat depending on findings. A 1st degree relative with advanced adenomas Colonoscopy beginning at age 50 OR at age of detection, whichever is first. Repeat depending on findings. A personal history of colorectal adenomatous polyps Colonoscopy repeated every 3-5years depending on findings. A personal history of inflammatory bowel disease Initiate screening 8-12 years after onset of symptoms (consult specialist), with colonoscopy every 1-2 years. Management is dependent upon findings. Screening and surveillance • For patients who are at general population risk (no symptoms of CRC and no family history of CRC, or negative test result for a known Lynch syndrome gene mutation in the family), recommendations should follow provincial guidelines – i.e. Fecal Occult Blood Test q2 years from age 50 Pearls • Lynch syndrome (LS) is the most common hereditary colorectal cancer predisposition syndrome • It is an autosomal dominant condition that results in an increased lifetime risk of CRC in addition to other cancers • Individuals at high risk of LS should be referred for a genetic consultation for consideration of genetic testing – Consult your local genetics or hereditary cancer centre if you are unsure of your patient’s eligibility • Surveillance and management of CRC and other cancers should be guided by genetic test results and/or family/ personal history – Studies show that conversations between patients and their healthcare providers are the strongest drivers of screening participation LEGEND Family history Kidney Colon Endometrial Breast Accident Mary Dx 45 CA Endometrial A&W Bob Dx 56 CA colon Stroke Nat Causes Steve Dx 72 Kevin, 67 CA Kidney A&W Paula Dx 66 CA- Br MI 72 A&W A&W A&W Dx 68 CA Colon Linda Dx 38 CA - colon Jeana Dx 40 Ca- Christa Dx 52 Endometrial CA – Colon Jane, 26 A&W A&W References • • • • Kohlmann W, Gruber SB. Lynch Syndrome. 2004 Feb 5 [Updated 2012 Sep 20]. In: Pagon RA, Adam MP, Bird TD, et al., editors. GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2013. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1211/ [Accessed April 4, 2014] Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Colorectal Cancer Screening V.2.2013© National Comprehensive Cancer Network, Inc 2013. All rights reserved. Accessed [Month and Day, Year]. To view the most recent and complete version of the guideline, go online to www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc. Leddin D et al. Canadian Association of Gastroenterology and Canadian Digestive Health Foundation: Guidelines on colon screening. Can J Gastroenterol 2004; 18(2): 93-99 Lynch HT et al. Review of the Lynch syndrome: history, molecular genetics, screening, differential diagnosis, and medicolegal ramifications. Clin Genet 2009; 76(1):1-18.