Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
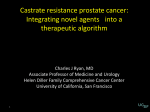
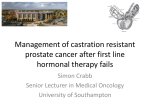
Treatment strategies for metastatic prostate cancer Oliver Hakenberg Department of Urology, Rostock University prostate cancer is hormone-dependent testosterone testes orchidectomy antiandrogens hypothalamus pineal gland LHRH analogues Prostata prolactine LHRH antiandrogens adrenal glands cortisole LHRH = luteinising hormone releasing hormone LH = luteinising hormone ACTH = adrenocorticotropal hormone adrenal androgens Pathologic fractures after orchidektomy % cumulative incidence of osteoporotic fractures n=235 50 40 orchidectomy 30 20 no orchidectomy 10 0 0 1 Daniell et al, J Urol 1997 2 3 4 5 6 7 8 9 years Immediate androgen ablation • permanent – advanced metastatic disease M+ – locally advanced, if androgen ablation is the only treatment option • adjuvant/temporary – radical prostatectomy with positive nodes (pN+) – adjuvant with radiotherapy in intermediate and high risk disease Early or delayed androgen ablation? Overall survival RPE pN+ early vs observation/delayed randomized n= 98 Cancer-specific survival Messing et al, Lancet Oncology 2006 androgen ablation • ↓ gonadal testosterone • 10-30% serum androgens from other sources • Adrenal cortex: DHEA + androstendione → transformed to testosterone in periphery (including prostate) • progression after xx months → hormone resistant hormone resistance? • de novo intratumoral androgen synthesis in progressive CRPC • → maintenance of intracellular andogen levels • → androgen receptor (AR) stimulation despite low serume testosterone • „castration-resistant prostate cancer“ = CRPC Locke et al, Cancer Res 2008 3 new developments • autologous vaccine sipuleucel-T (IMPACT) – mCRPC docetaxel-naive (85%) – improved OS vs placebo • cabazitaxel (TROPIC) – mCRPC doxetaxel-refractory – improved OS vs mitoxantrone • arbiraterone – hormonal principle in CPRC Kantoff et al, N Engl J Med 2010 De Bono et al, Lancet 2010 Arbiraterone inhibition of testosterone biosynthesis • arbiraterone acetate inhibits – C17,20 lyase – 17 hydroxylase – Inhibition selective & irreversible • • • • adrenals, testes, prostate cancer cells arbiraterone acetate: prodrug good oral bioavailability Development of resistance Sonpavde et al, Eur Urol 2011 Attard et al, Cancer Res 2009 Study data: arbiraterone in CRPC • phase I – chemotherapy-naive CRPC patients • phase-II NCT 00474383 – progression after docetaxel • phase-III NCT 00638690 – progression after docetaxel • phase III NCT 00887198 – asymptomatic, low metastatic load in chemotherapy-naive patients phase I • n=21 • chemo-naive, CRPC – 12/21 with PSA↓>50% and > 3 months – of which in 6/12 PSA↓ > 90% – PR (RESIST) in 5/8 patients and ↓analgesic medication – no grade grade 3/4 toxicity Attard et al, J Clin Oncol 2008 phase II a • • • • • chemotherapy-naive CRPC patients PSA↓> 50% in 70-80% of patients RESIST response 37.5% median time to PSA-rise 225 days dexamethasone at progression with arbiraterone: further PSA↓>50% in 33% Attard et al, J Clin Oncol 2009 phase II b • n= 47 docetaxele-pretreated CRPC • PSA↓> 50% in 51% of patients • 35 with RESIST – PR 17% – SD 66% • 23% ECOG improvement Reid et al, J Clin Oncol 2009 Reid et al, J Clin Oncol 2009 Reid et al, J Clin Oncol 2009 Phase II c • docetaxele-pretreated CRPC • better efficacy without ketoconazole pretreatment – 53% vs 33% PSA-response without/with – 31% vs 4% PSA↓>90% without/with ketoconazole – median time to progression 198 vs 99 days with/without ketoconazole Danila et al, J Clin Oncol 2009 phase III (COU-AA-301) • n=1195 docetaxel-refractory CRPC • arbiraterone vs placebo 2:1 randomisation • stratification – – – – ECOG 0-1 vs 2 prior chemotherapy schedules 1 vs 2 pain score type of progression: PSA vs XR phase III (COU-AA-301) 1.interim analysis 2010 • • • • • OS 14.8 vs 10.4 months TTP 10.2 vs 6.6 months rPFS 5.6 vs 3.6 months PSA RR 29.1% vs 5.5% toxicity – – – – hyperhydration 2.3% vs 1.0% hypokalaemia 3.8% vs 0.8% hypertension 1.3% vs 0.3% cardiopulmonary 4.1% vs 2.3% De Bono et al, ESMO 2010 arbiraterone • n=1195 docetaxel resistant • 2:1 randomisation – arbiraterone 1000 mg + 5 mg prednisone vs – placebo + 5 mg prednisone • overall survival – arbiraterone – placebo 14.8 months 10.9 months de Bono et al, N Engl J Med 2011 treatment options for metastatic prostate cancer • hormonal – androgen ablation • orchidectomy • LHRH-antagonists or –agonists • androgen blockers – androgen conversion blocker • arbiraterone • chemotherapy – docetaxel – cabazitaxel • • • • bisphosphonates pain treatment nuclear medical tretament: samarium, strontium best supportive care Prognosis of metastatic prostate cancer • • • • initial response to androgen ablation > 80% progression in 50-60% of patients within 2 years after that median survival 23-37 months 5 year survival rate with M+oss 20% androgen antagonists • steroidal – cyproterone acetate • non-steroidal – bicalutamide – flutamide – nilutamide Early Prostate Cancer Program reduction of the risk of PSA progression by 59 % Kaplan-Meier curve of time to PSA progression 1.0 proportion without event 0.9 0.8 0.7 0.6 0.5 0.4 0.3 bicalutamide 150 mg + standard care Placebo + standard care 0.2 0.1 0.0 0 6 12 18 24 30 36 time (months) HR 0.41; 95% CI 0.38, 0.45; p<<0.0001 42 48 54 60 natural course of prostate cancer after radical prostatectomy and PSA recurrence (n= 311) distant metastases PSA recurrence 0 Pound et al., JAMA 1999 5 death of prostate cancer 10 15 years Hormone-independent prostate cancer hormone independent hormone naive hormone withdrawal hormone dependent hormone sensitive hormone independent definition of castration-resistant prostate hormonerefractory prostate cancer (HRPC) • serume testosteron at castration level • secondary hormonal treatment without effect • ketoconazole • estrogens • rising PSA at 3 consecutive measurements at intervals of 1 week at leastt • with continued LHRH – blockade and after witrhdrawal of androgen blocker • lowest PSA limit: 0.4 ng/ml Chemotherapy for prostate cancer? Reviews response rates P.Walsh 1995: 1985: (17 Studien) % „This is going to be an extremely short 6,5 discussion. Not only does it fail to cure the cancer, it doesn’tM. even prolong Eisenberger, J Clinsurvival Oncol 1985 to any significant degree, and its side effects only add to the unpleasantness of having prostate cancer.“ 1992: (26 Studien) 8,7 % Yagoda & Petrylak, Cancer 1993 chemotherapy for prostate cancer – mitoxantrone for HRPC? • phase III: mitoxantrone (12mg/m²) + prednisone (10mg/d) prednisone (10mg/d) vs. – 161 patients. (80 M+P; 81 P) • phase III: mitoxantrone (14mg/m²) + hydrocortisone (40mg/d) vs. hydrocortisone (40mg/d) – 242 patients results – improvement in pain – improvement in quality of life – duration of response 5-7 months – no influence on survival Tannock et al. 1996 Kantoff et al. 1999 docetaxel • TAX 327 • SWOG 9916 • both studies showed overall survival advantage for docetaxel Petrylak, N Engl J Med 2004 Tannock, N Engl J Med 2004 docetaxel chemotherapy overall survival SWOG 9916 no. at Risk 100% D + E 338 M + P 336 80% median survival (months) no (n) died 217 235 18 16 HR: 0.80 (95% CI 0.67, 0.97), p = 0.01 med. F/U: 1 J 60% 40% 20% 0 12 Petrylak et al, N Engl J Med 2004 24 36 48 months SWOG 99-16 Petrylak J NCI 2006 Survival in subgroups docetaxel 3 weekly vs mitoxantrone hazard ratio in favour of docetaxel mitoxantrone Intent to Treat age < 65 age ≥ 65 age ≥ 75 pain no pain yes KPS ≥ 80 KPS ≤ 70 0.2 Tannock et al, N Engl J Med 2004 0.4 0.6 0.8 1 1.2 1.4 Cochrane Review chemotherapy of HRPC • n=6929 patients; 47 studies • investigated substances: – – – – – – – EMP docetaxel 5-FU cyclophosphamide doxorubicine mitoxantrone vinorelbine Shelley M, Harrison C et al. Cochrane Database Syst Rev 2006 Cochrane Review • PSA response (>50%): – – – – – – – EMP docetaxel 5-FU cyclophosphamide doxorubicine mitoxantrone vinorelbine Shelley M, Harrison C et al. Cochrane Database Syst Rev 2006 48% 52% 20% n.d. 50% (CAVE: only 1 study!) 33% n.d. results • only DOC => months) • pain ↓ • quality of life ↑ overall survival ↑ (<2.5 DOC > Mit + Pred DOC > Mit + Pred authors‘ conclusion: „At the present time this* probably represents the best chemotherapeutic regime available for men with HRPC“ *- docetaxel q3w Shelley M, Harrison C et al. Cochrane Database Syst Rev 2006 secondary hormone manipulation or chemotherapy? secondary hormone manipulation chemotherapy CALGB9583 SWOG 9916 TAX-327 AAW + Ketokonazol EMP docetaxel vs MP DP q3w vs DP q1w vs MP n 260 770 1006 overall survival in better arm 16.7 months 17.5 months 18.9 months overall survival in worse arm 15.3 months 15.6 months 16.5 months Bellmunt, Eur Urol Suppl 2009 open questions • • • • • • when to start with chemotherapy? should asymptomatic M+ patients be treated? how long to continue treatment? secondary treatment? intermittent chemotherapy? re-exposition? Early vs late chemotherapy? • for – benefit established for other entities (breast cancer, colorectal cancer) – lower tumour mass – treatment prolongs survival • against – toxicity vs unreliable response – early induction of chemotherapy-refractory state – outcome is not influenced since no difference in survival between symptomatic vs asymptomatic patients (TAX327) forms of HRPC indications for starting with chemotherapy • only rising PSA • asymptomatic, low metastatic load no indication PSA doubling time? individual decision inclusion in study? • asymptomatic, large metastatic load yes • symptomatic metastases yes Estimating the prognosis in CPRC PSA doubling time • günstig – TAX 327: PSA-DT > 55 Tage – Oudard et al: PSA-DT > 45 Tage Armstrong et al, Clin Cancer Res 2007 Oudard et al, Ann Oncol 2007 nomographic estimation Armstrong, A. J. et al. Clin Cancer Res 2007;13:6396-6403 rising PSA under chemotherapy… • often initiial PSA flare-up • no negative influence on survival, unless there are signs of clinical progression => minimum of 8 weeks treatment before deciding to discontinue ! Olbert Anticancer Drugs 2006 PSA-Flare with chemotherapy in patients with subsequent PSA response or stable disease PSA values normalized to a starting point of 100 ng/ml Thuret etrestrictions al, Ann Oncol 2008 Copyright may apply. Chemotherapy until… • best number of cycles unknown • TAX 327: mean of 8 cycles • but: chronic toxicity increases with no of cycles • intermittend chemotherapy? When to discontinue chemotherapy…? • definite worsening of physical state • PSA doubling time < 3 Monate • slow PSA increase: - discontinue if clinically progressive Miller et al. Akt Urol 2006 First line chemotherapy docetaxel Mono (75mg/m² KO d1, q21d) Second line chemotherapy options: – docetaxel (M D) – docetaxel weekly – mitoxantrone (D M) – satraplatin (SPARC) – cabazitaxel PR: 44-85% PR: 72% PR: 6-15% Cabazitaxel second line overall survival open label, randomized, n= 755 CPRC patients with progression on docetaxel cabazitaxel 25 mg/m2 q3w + prednisone 10 mg p.o. daily vs mitoxantrone 12 mg/m2 q3w i.v.+ prednisone 10 mg p.o. daily mean survival overall CABA 15.1 months MITO 12.7 months de Bono et al, Lancet 2010 Cabazitaxel second line progression-free survival de Bono et al, Lancet 2010 ketoconazole • • • • 200 or 400 mg tid p.o. ketoconazole + hydrocortisone replacement doses 30-0-10 mg p.o. n= 114 response depends on disease burden Keizman et al, Prostate 2010 Beltran et al, Eur Urol 2011 Hypothetical calculation Future prognosis of metastatic prostate cancer? • • • • • • initial response to androgen ablation > 80% progression in 50-60% of patients within 2 years after that median survival 23-37 months + 4 months with docetaxel + 4 months with cabazitaxel + 4 months with arbiraterone „This will buy you three months“ Rostock