Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
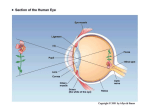
Functional and Dysfunctional Anatomy of Visual Cortex Emily A UlmerA, Stephanie M. FranczakB, Edgar DeYoe PhDC, Andrew P Klein MDC, Leighton P Mark MDC University Lake School, Hartland, WIA Divine Savior Holy Angels, Milwaukee, WIB Medical College of Wisconsin, Milwaukee, WIC Purpose: The purpose of this exhibit is to demonstrate functional brain anatomy and deficit localization of vision cortex. Overview: Visual field topography is preserved on the retina, through visual pathways, and in the visual cortex. Functional brain mapping reveals the retinotopic organization of the visual cortex and can be used to understand and predict the location of scotoma. Divergent hierarchical and parallel processing of visual stimuli attributes generates the perception of color, form, motion and position. A ventral processing stream provides information to the temporooccipital visual area, or the “What Area,” for visual object and color recognition processing. A dorsal processing stream provides information to the parietal visual area, or the “Where Area,” for higher visuospatial and attention processing. Each processing stream has multiple functional sub-streams and numerous interconnections. This tutorial reviews the functional organization of the visual system and associated deficits. For a more thorough review on the topic, see: 1. 2. DeYoe, EA, Raut RV. Neuroimaging Clinics 24.4, Clinical Applications of Functional MRI, Elsevier, November 2014. Visual Mapping Using Blood Oxygen Level Dependent FMRI pg 573-584. Jonathan D. Trobe, The Neurology of Vision Oxford University Press March 2001.V. Overview The visual system engages in significant computational processing to transform simple retinal images and sensory cues, to infer attributes about the physical world Retinal images Sensory Cues (V1) Image Intensity Wavelength Time Position Eyes (R,L) Primary Luminance Spectral Inferred Attributes (extrastriate cortex) 3D form Shape Size Rigidity Feature-based Contrast Surface properties Disparity Color (brightness, hue, saturation) 2-D velocity Visual texture 2-D orientation Specular reflectance Transparency (shadows & highlights) V1 = 1o visual cortex Extrastriate = association visual cortex 3-D spacial relationships Relative positions (X,Y,Z) 3-D orientation in space 3-D movement Trajectory Rotation What is it? Temporal visual cortex Where is it? Parietal visual cortex Take a minute to review the major visual pathways and functions Geniculostriate system Retinotectal system (see Agarwal et al., EdE Conscious visual perception 41, Neural Control of Ocular Movements) Pathway: Retina lateral geniculate nucleus (LGN) Directing eye movements and visual striate cortex extrastriate cortex attention Pathway: Retina superior colliculus pulvinar extrastriate cortex Geniculostriate and Retinotectal Visual Systems Temporal half of right retina Nasal half of left retina Retina Meyer's loop Lateral geniculate body (nucleus) Medial geniculate body Pulvinar Extrastriate cortex Optic radiations (in retrolenticular limb of internal capsule) Right lateral geniculate nucleus Brachium of sup. colliculus Superior colliculus Striate cortex Visual cortex of right hemisphere Visual reflex pathways (see Agarwal et al., EdE-41, Neural Control of Ocular Movements) Accommodation (focusing the eye): Controls muscles of the ciliary body via a pathway through the cortex, pretectum, and ciliary ganglion. Contraction of the ciliary muscle causes thickening of the lens. Pupillary control of light intensity: Constriction: Retinal signals control pupillary constrictor muscles via pathways through the pretectum, Edinger-Westphal nucleus, and ciliary ganglion Dilation: Retinal signals control dilator muscles via pathways through the spinal cord and superior cervical ganglion Fibers emanating from the LGN forming the optic radiation Optic radiation: Chiasm Optic tract Meyers loop tract LGN Radiations Visual cortex Projects from the LGN to the primary visual cortex (V1) Passes through the posterior (retrolenticular) aspect of the posterior limb IC Superior fibers course backward toward the occipital lobe Inferior fibers course antero-inferiorly around the temporal horn before turning backwards (Meyer`s loop) Optic radiation maintains retinotopic organization Now that you have reviewed the geniculostriate pathway, try your luck at predicting visual field deficits. Click once for the lesion and a second time for the deficit. RIGHT EYE LEFT EYE VISUAL FIELDS LEFT RIGHT Total blindness - Right eye Left superior quadrantanopia Optic nerve Bitemporal hemianopia Optic chiasm Optic tract Chiasm Optic tract Meyers loop tract Geniculocalcarine tract or optic radiations Left homonymous hemianopia Lat. geniculate body LGN Left homonymous superior Meyer’s quadrantanopia Loop has fibers from both eyes Radiations Primary visual cortex (area 17) Visual cortex Left homonymous hemianopia (macula spared) Topography of the Visual System Visual field Topography of the Visual System & Cortical Magnification Retina Uncrossed fibers Crossed fibers A B LGN Topography of the visual system Overlapping visual fields Projection on right retina Left retina Projection on left lateral geniculate body Optic nerve Optic tract Optic chiasm Lat. geniculate body Projection on right LGN Calc. fissure Projection on left occipital lobe Geniculocalcarine (optic) radiation Occipital Lobe Preserved topography Visual field topography is preserved on the retina The topography of the receptor array (retina) is preserved in the LGN The retinotopic organization of the LGN is maintained in the visual cortex Foveal magnification Foveal vision is magnified in the LGN and primary visual cortex Magnification changes from 4 mm/degree to 0.5 mm/degree as the visual representation moves from 1o to 25o away from the center of gaze One central degree of visual field is represented by 64 times the area of cortex than that devoted to the peripheral visual field Foveal vision is represented in the cortex of the occipital pole Divergence of Hierarchical Visual Processing There is hierarchical (more complex) processing of visual stimuli attributes from retina to higher-order visual areas There is a relative divergence of processing of attributes (i.e. color, form, motion and position) Ventral processing stream Temporal visual area Object /word/face/place recognition “What area” Dorsal processing stream Parietal visual area Visuospatial processing and visual attention “Where area” Each processing stream has multiple functional sub-streams with numerous interconnections The primary visual cortex (V1) is centered around the calcarine sulcus. Hierarchical processing occurs in association cortex along dorsal (parietal) and ventral (temporal) processing streams, becoming ever more complex Spatial relations Visual attention Motion Identification Visual memory The type of visual deficit present depends on the location of the cortical lesion Deficits: V1, V2 – complete blindness of visual information Occipital pole – central visual field deficit Closer to parieto-occipital sulcus (POS) – peripheral visual field deficit Higher visual areas – loss of different types of visual information processing such as shape, color, motion, and/or position Specific deficits affected by involvement of dorsal or ventral processing streams Ventral Stream Visual Deficits Deficits of the ventral stream (ventral temporal area - VTA) Visual object agnosia Bilateral but left >right TVA Prosopagnosia (faces) Bilateral or right >>left TVA Pure word alexia Left TVA Contralesional achromatopsia (lack of color recognition) V4/VO Color anomia (naming colors) Left TVA Visual amnesia Bilateral or right >>left Dorsal Stream Visual Deficits Deficits of the dorsal stream (Parietal visual area - PVA) Hemispatial neglect Right >>>Left PVA/angular gyrus, or frontal lobe, or pulvinar Bilateral inattention Bilateral PVA Acquired ocular motor apraxia Bilateral PVA Optic ataxia Usually bilateral >> unilateral PVA Impaired spatial relations Right >>>left parieto-occipital Akinetopsia Bilat. hMT (Occ-temp-pariet jxn) Retinotopic Mapping of Visual Cortex The retinotopic organization of the visual cortex can be mapped with fMRI: Eccentricity Mapping eccentricity in 3 subjects 3D Flat Map The retinotopic organization of the visual cortex can be mapped with fMRI: Polar Angle Polar angle mapping in 3 subjects 3D Flat Map Functional field maps can be constructed from eccentricity and polar angle coordinates, relating activation to visual field locations Composite eccentricity and polar angle maps can localize functional visual cortical areas Cases: Apply Your Knowledge 48 yo with right visual field cut Where is the infarct? (choose one) A. Right thalamus (MGN) B. Left thalamus (MGN) C. Right medial occipital lobe D. Left medial occipital lobe 48 yo with right visual field cut D. Left medial occipital lobe Sulcal effacement 48 yo with right visual field cut deficit may occur at several AD.visual Leftfield medial occipital lobe locations along the visual pathway. Tracing the pathways on CT in this case revealed subtle left occipital sulcal effacement, suggesting an infarct accounting for the contralateral visual deficit. Visual Field Deficits Lesions of the Visual Pathways 3 1 Monocular Blindness 2 Monocular Blindness and (Chiasm) 1 Meyers’ Loop 4 Optic Nerve 2 Superior Quadrantopia Optic Tract 3 Bitemporal Hemianopia 5 LGN 4 Homonymous Hemianopia Optic Radiation 5 Homonymous Superior Quadrantanopia Homonymous Hemianopia 6 Visual Cortex 6 (macula spared) 68 yo with right visual field deficit Where is the acute infarct? (choose one) A. Right corona radiata B. Right putamen C. Left posterior limb IC D. Left thalamus 68 yo with right visual field deficit C. Left posterior limb internal capsule 68 yo with right visual field deficit C. Left posterior limb internal capsule (PLIC) The infarct is located in the retrolenticular portion of the internal capsule (bordering the posterior putamen), corresponding to anterioposterior orientation of fiber bundles (green) at DTI. This area contains portions of non-motor fiber tracts such the optic radiation, the acoustic radiation, and is adjacent to somatosensory fibers. Thus, an infarct here may cause deficits in vision and audition, and somatosensory perception. Retrolenticular portion of the PLIC Retrolenticular portion of the PLIC 59 yo RH patient with a ventral temporo-occipital infarct What is the most likely deficit? (choose one) A. Right hemi-spatial neglect B. Visuomotor dysfunction C. Optic ataxia D. Visual agnosia 59 yo RH patient with a ventral temporo-occipital infarct D. Visual agnosia Higher visual processing occurs along hierarchical dorsal and ventral processing streams. The temporal visual area (ventral processing stream) compares what one sees to visual memories, to provide recognition of objects, faces, places, and words (dominant hemisphere). Infarcts of the ventral visual areas may cause a class of deficits known as agnosias. Agnosia is the inability to recognize objects, places, faces, as well as words in the dominant hemisphere. Visual spatial, visual motor, visual attention Object, word, place, face recognition 53 yo with an occipital infarct What is the most likely deficit? (choose one) A. Left hemianopia B. Left upper quadrantanopia C. Left lower quadrantanopia D. Agnosia 53 yo with an occipital infarct C. Left lower quadrantanopia The infarct is located in the supracalcarine visual cortex (cuneus), C which processes visual information from the lower visual field. Thus, a unilateral supra-calcarine occipital cortex infarct will result in a Calcarine contralateral lower quadrantanopia. Cuneus infarct sulcus fMRI 59 yo right handed patient with a right parietal infarct What is the most likely deficit? (choose one) A. Left hemianopia B. Left hemispatial neglect C. Aphasia D. Agnosia 59 yo right handed patient with a right parietal infarct B. Left hemispatial neglect Hierarchical visual processing occurs along dorsal and ventral processing streams. Parietal visual areas (dorsal processing stream) process visual spatial and visual motor information, as well as support attention to visual stimuli. Cortex of the inferior parietal lobule is responsible for visual attention. The left parietal visual area (PVA) supports attention to the right visual hemi-field while the right PVA supports attention to both visual hemi-fields. Consequently, left PVA infarcts rarely cause hemi-spatial neglect, because the right PVA supports both hemi-fields. Right PVA infarcts on the other hand may cause left hemi-spatial neglect. It should be noted, however, that recent studies have questioned this classic model and suggest the organization may be more complex. Stay tuned… Visual spatial, visual motor, visual attention Object, word, place, face recognition 8 yo female with refractory right hemispheric seizures and visuospatial dysfunction. Where is the abnormal cortex likely to be? Click once for answer 8 yo female with visuospatial dysfunction, Answer: Right parietal visual area PET Based on cortical retinotopy, what visual field deficits are at risk? What visual field deficits are at risk? Click once for answer Answer: Peripheral vision is at risk along the posterior tumor border Eccentricity What visual field deficits are at risk? What about white matter? Answer: Central and peripheral vision is at risk along the lateral border Eccentricity DTI Optic radiation Conclusions Understanding visual system functional and dysfunctional anatomy improves the accuracy of Neuroradiologic interpretations at standard MRI Understanding visual system functional anatomy improves utilization of fMRI and DTI for presurgical planning Understanding the effects of lesions on vision function provides a framework by which to guide surgical decision-making