Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
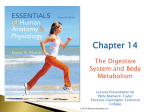
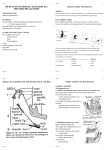
ANATOMY OF THE DIGESTIVE SYSTEM PART I Oral region Pharynx Esophagus Stomach Small intestine Large intestine 19.11.2013 Kaan Yücel M.D., Ph.D. http://yeditepeanatomyfhs121.wordpress.com Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I The oral region includes the oral cavity (mouth), teeth, gingivae (gums), tongue, palate, and the region of the palatine tonsils. The digestion starts here in the oral cavity. It is the place where the food is ingested and prepared for digestion in the stomach and small intestine. The oral cavity (mouth) is inferior to the nasal cavities and extends from the lips to the pharynx. The oral cavity is separated into two regions by the upper and lower dental arches consisting of the teeth and alveolar bone that supports them: The outer oral vestibule and the inner oral cavity proper (mouth proper). The lips are mobile, musculofibrous folds surrounding the mouth. The cheeks (L. buccae) form the movable walls of the oral cavity. The teeth are set in the tooth sockets. There are 20 deciduous teeth and 32 permanent teeth. The gingivae (gums) are composed of fibrous tissue covered with mucous membrane. The tongue is a mass of striated muscle covered with mucous membrane which forms part of the floor of the oral cavity and part of the anterior wall of the oropharynx. The superior surface of the oral or anterior twothirds of the tongue is oriented in the horizontal plane. The pharyngeal surface or posterior one-third of the tongue curves inferiorly and becomes oriented more in the vertical plane. The superior surface of the oral part of the tongue is covered by hundreds of papillae. There are four types of papillae in the tongue: filiform papillae;fungiform papillae;the largest of the papillae;vallate papillae, and foliate papillae. The muscles of the tongue are divided into two types: intrinsic and extrinsic. The roof of the oral cavity consists of the palate, which has two parts-an anterior hard palate and a posterior soft palate. Five muscles on each side contribute to the formation and movement of the soft palate. The fauces (L. the throat) is the space between the cavity of the mouth and the pharynx. The fauces is bounded superiorly by the soft palate, inferiorly by the root of the tongue. The parotid gland is the largest salivary gland. Parasympathetic secretomotor supply arises from the glossopharyngeal nerve. Parasympathetic stimulation of the parotid gland produces thin watery saliva. Submandibular gland lies beneath the lower border of the body of the mandible. Parasympathetic secretomotor supply is from the facial nerve. Sublingual gland lies beneath the floor of the mouth. Nerve supply is the same as the submandibular gland. The pharynx is a musculofascial half-cylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck. It is the superior expanded part of the alimentary system posterior to the nasal and oral cavities. Based on these anterior relationships the pharynx is subdivided into three regions, the nasopharynx, oropharynx, and laryngopharynx. The abundant lymphoid tissue in the pharynx forms an incomplete tonsillar ring (Waldeyer’s Ring of Lymphoid Tissue) around the superior part of the pharynx. Tonsils occur mainly in four areas:pharyngeal tonsil, palatine tonsils, lingual tonsil, tubal tonsil. The esophagus is a muscular tube about 10 in. (25 cm) long, extending from the pharynx to the stomach. It begins in the neck where it is continuous with the laryngopharynx at the pharyngo-esophageal junction. The stomach is located at the epigastric, umbilical, and left hypochondrium regions. The stomach is the most dilated part of the gastrointestinal tract and has a J-like shape. It is positioned between the abdominal esophagus and the small intestine. The stomach is divided into four regions: cardia, fundus, body, and pylorus. The small intestine is the longest part of the gastrointestinal tract and extends from the pyloric orifice of the stomach to the ileocecal fold. This hollow tube, which is approximately 6-7 m long with a narrowing diameter from beginning to end, consists of the duodenum, the jejunum, and the ileum. The small intestine is the primary site for absorption of nutrients from ingested materials. The large intestine extends from the distal end of the ileum to the anus, a distance of approximately 1.5 m. in adults. It absorbs fluids and salts from the gut contents, thus forming feces, and consists of the cecum, appendix, colon, rectum, and anal canal. 2 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I 1. ORAL REGION includes the oral cavity (mouth), teeth, gingivae (gums), tongue, palate, and the region of the palatine tonsils. The digestion starts here in the oral cavity. It is the place where the food is ingested and prepared for digestion in the stomach and small intestine. Food is chewed by the teeth, and saliva from the salivary glands facilitates the formation of a manageable food bolus (L. lump). Swallowing is voluntarily initiated in the oral cavity (Oral phase). The voluntary phase of the process pushes the bolus from the oral cavity into the pharynx, where the involuntary (automatic) phase of swallowing occurs. The three phases of swallowing: Oral phase, pharyngeal phase, and esophageal phase. http://www.singhealth.com.sg/PatientCare/ConditionsAndTreatments/Pages/Throat-Virtual-Tour.aspx ORAL CAVITY The oral cavity (mouth) is inferior to the nasal cavities and extends from the lips to the pharynx. The roof of the oral cavity consists of the hard and soft palates. The floor is formed mainly of soft tissues, which include a muscular diaphragm and the tongue. The lateral walls (cheeks) are muscular and merge anteriorly with the lips surrounding the oral fissure (the anterior opening of the oral cavity). The oral cavity is continuous with the cavity of the pharynx at the oropharyngeal isthmus. The oral cavity is separated into two regions by the upper and lower dental arches consisting of the teeth and alveolar bone that supports them: The outer oral vestibule, a slit-like space, is between the dental arches and the deep surfaces of the cheeks and lips-the oral fissure opens into it and can be opened and closed by muscles of facial expression, and by movements of the lower jaw.The duct of the parotid salivary gland (Stensen’s duct) opens on a small papilla into the vestibule opposite the upper second molar tooth. The inner oral cavity proper (mouth proper) is the space between the upper and lower dental arches (maxillary and mandibular alveolar arches and the teeth they bear). It is enclosed by the dental arches. The oral cavity has multiple functions: • It is the inlet for the digestive system involved with the initial processing of food, which is aided by secretions from salivary glands. It is in the oral cavity that food and drinks are tasted and where mastication and lingual manipulation of food occur. • It manipulates sounds produced by the larynx and one outcome of this is speech. • It can be used for breathing because it opens into the pharynx, which is a common pathway for food and air. For this reason, the oral cavity can be used by physicians to access the lower airway. 3 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I Lips & Cheeks The lips are mobile, musculofibrous folds surrounding the mouth and are covered externally by skin and internally by mucous membrane. The lips function as the valves of the oral fissure, containing the sphincter (orbicularis oris) that controls entry and exit from the mouth and upper alimentary and respiratory tracts. The cheeks (L. buccae) form the movable walls of the oral cavity. Teeth The teeth are set in the tooth sockets. There are 20 deciduous teeth and 32 permanent teeth: four incisors, two canines, four premolars, and six molars in each jaw. They begin to erupt at 6 years of age. The last tooth to erupt is the third molar, which may happen between the ages of 17 and 30. The chief functions of the teeth are to: • Incise, reduce, and mix food material with saliva during mastication (chewing). • Help sustain themselves in the tooth sockets by assisting the development and protection of the tissues that support them. • Participate in articulation (distinct connected speech). Gingivae (Gums) The gingivae (gums) are composed of fibrous tissue covered with mucous membrane. The gingiva proper (attached gingiva) is firmly attached to the alveolar processes of the mandible and maxilla and the necks of the teeth. Figure 1. Oral cavity http://training.seer.cancer.gov/anatomy/digestive/regions/mouth.html Tongue The tongue is a mass of striated muscle covered with mucous membrane. The tongue forms part of the floor of the oral cavity and part of the anterior wall of the oropharynx. Its anterior part is in the oral cavity and is somewhat triangular in shape with a blunt apex of tongue. The apex is directed anteriorly and sits 4 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I immediately behind the incisor teeth. The root of tongue is attached to the mandible and the hyoid bone. The muscles attach the tongue to the styloid process and the soft palate above and to the mandible and the hyoid bone below. The superior surface of the oral or anterior two-thirds of the tongue is oriented in the horizontal plane. The pharyngeal surface or posterior one-third of the tongue curves inferiorly and becomes oriented more in the vertical plane. Papillae The superior surface of the oral part of the tongue is covered by hundreds of papillae. There are four types of papillae in the tongue: filiform papillae are small cone-shaped projections of the mucosa that end in one or more points; fungiform papillae are rounder in shape and larger than the filiform papillae, and tend to be concentrated along the margins of the tongue; the largest of the papillae are the vallate papillae, which are blunt-ended cylindrical papillae invaginations in the tongue's surface-there are only about 8 to 12 vallate papillae in a single V-shaped line immediately anterior to the terminal sulcus of tongue; foliate papillae are linear folds of mucosa on the sides of the tongue near the terminal sulcus of tongue. The papillae in general increase the area of contact between the surface of the tongue and the contents of the oral cavity. All except the filiform papillae have taste buds on their surfaces. The undersurface of the oral part of the tongue lacks papillae, but does have a number of linear mucosal folds. A single median fold (the frenulum of tongue) is continuous with the mucosa covering the floor of the oral cavity. On each side of the frenulum is a lingual vein, and lateral to each vein is a rough fimbriated fold. The oral and pharyngeal surfaces are separated by a V-shaped terminal sulcus of tongue. This terminal sulcus forms the inferior margin of the oropharyngeal isthmus between the oral and pharyngeal cavities. At the apex of the V-shaped sulcus is a small depression (the foramen cecum of tongue), which marks the site in the embryo where the epithelium invaginated to form the thyroid gland. In some people a thyroglossal duct persists and connects the foramen cecum on the tongue with the thyroid gland in the neck. The mucosa covering the pharyngeal surface of the tongue (posterior one-third of the tongue) is irregular in contour because of the many small nodules of lymphoid tissue in the submucosa. These nodules are collectively the lingual tonsil. There are no papillae on the pharyngeal surface. Muscles The tongue is completely divided into a left and right half by a median sagittal septum composed of connective tissue. This means that all muscles of the tongue are paired. The muscles of the tongue are divided 5 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I into two types: intrinsic and extrinsic. Intrinsic muscles are confined to the tongue and are not attached to bone and alter the shape of the tongue. The extrinsic muscles are attached to bones and the soft palate. Intrinsic muscles The intrinsic muscles of the tongue originate and insert within the substance of the tongue. They are divided into superior longitudinal, inferior longitudinal, transverse, and vertical muscles, and they alter the shape of the tongue. Working in pairs or one side at a time the intrinsic muscles of the tongue contribute to precision movements of the tongue required for speech, eating, and swallowing. Extrinsic muscles Extrinsic muscles of the tongue originate from structures outside the tongue and insert into the tongue. These muscles protrude, retract, depress, and elevate the tongue. There are four major extrinsic muscles on each side. 1. Genioglossus: make a substantial contribution to the structure of the tongue. They occur on either side of the midline septum that separates left and right halves of the tongue. These muscles stick the tongue out. 2. Hyoglossus: thin quadrangular muscles lateral to the genioglossus muscles which depress the tongue. 3. Styloglossus: originate from the anterior surface of the styloid processes of the temporal bones. They enter the lateral surface of the tongue where they blend with the superior margin of the hyoglossus and with the intrinsic muscles. The styloglossus muscles retract the tongue and pull the back of the tongue superiorly. 4. Palatoglossus: muscles of the soft palate and the tongue. Each originates from the undersurface of the palatine aponeurosis and passes anteroinferiorly to the lateral side of the tongue. The movements of the palatoglossus muscle facilitate closing of the oropharyngeal isthmus and as a result separate the oral cavity from the oropharynx. Unlike other muscles of the tongue, but similar to most other muscles of the soft palate, the palatoglossus muscles are innervated by the vagus nerves [X]. The rest of the intrinsic muscles of the tongue are innervated by the hypoglossal nerve [XII]. Asking a patient to "stick your tongue out" can be used as a test for the hypoglossal nerves [XII]. If the nerves are functioning normally, the tongue should protrude evenly in the midline. If the nerve on one side is not fully functional, the tip of the tongue will point to that side. Vessels The major artery of the tongue is the lingual artery. On each side, the lingual artery originates from the external carotid artery in the neck. The tongue is drained by dorsal lingual and deep lingual veins. The deep lingual veins are visible through the mucosa on the undersurface of the tongue. 6 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I Innervation Innervation of the tongue is complex and involves a number of nerves (trigeminal nerve CN V; sensation from anterior 2/3, glossopharyngeal nerve (CN IX) from posterior 1/3, taste from oral part is carried by the facial nerve (CN VII); taste from the pharyngeal part of the tongue by the glossopharyngeal nerve (CN IX)). Protrusion, retraction, depression, shape changes are the main movemements of the tongue. Palate The roof of the oral cavity consists of the palate, which has two parts-an anterior hard palate and a posterior soft palate. The hard palate separates the oral cavity from the nasal cavities. It consists of a bony plate covered above and below by mucosa: • above, it is covered by respiratory mucosa and forms the floor of the nasal cavities; • below, it is covered by a tightly bound layer of oral mucosa and forms much of the roof of the oral cavity. The palatine processes of the maxillae form the anterior three-quarters of the hard palate. The horizontal plates of the palatine bones form the posterior one-quarter. In the oral cavity, the upper alveolar arch borders the hard palate anteriorly and laterally. Posteriorly, the hard palate is continuous with the soft palate. Soft palate The soft palate continues posteriorly from the hard palate and acts as a valve that can be: depressed to help close the oropharyngeal isthmus; elevated to separate the nasopharynx from the oropharynx. The soft palate is formed and moved by four muscles and is covered by mucosa that is continuous with the mucosa lining the pharynx and oral and nasal cavities. The small tear-shaped muscular projection that hangs from the posterior free margin of the soft palate is the uvula. Muscles of the soft palate Five muscles on each side contribute to the formation and movement of the soft palate. Two of these, the tensor veli palatini and levator veli palatini, descend into the palate from the base of the skull. Two others, the palatoglossus and palatopharyngeus, ascend into the palate from the tongue and pharynx, respectively. The last muscle, the musculus uvulae, is associated with the uvula. All muscles of the palate are innervated by the vagus nerve [X] except for the tensor veli palatini, which is innervated by the mandibular nerve [V3]. 7 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I Tensor veli palatini Tenses the soft palate; opens the pharyngotympanic tube. The tensor veli palatini muscle is composed of two parts-a vertical muscular part and a more horizontal fibrous part, which forms the palatine aponeurosis. Levator veli palatini Only muscle to elevate the soft palate above the neutral position. Palatopharyngeus Depresses soft palate; moves palatopharyngeal arch toward midline; elevates pharynx. Palatoglossus Depresses palate; moves palatoglossal arch toward midline; elevates back of the tongue. Musculus uvulae Elevates and retracts uvula; thickens central region of soft palate. Fauces (Thorat) The fauces (L. the throat) is the space between the cavity of the mouth and the pharynx. The fauces is bounded superiorly by the soft palate, inferiorly by the root of the tongue. The oropharyngeal isthmus (isthmus of the fauces) is the short constricted space that establishes the connection between the oral cavity proper and the oropharynx. By closing the oropharyngeal isthmus, food or liquid can be held in the oral cavity while breathing. The palatine tonsils, often referred to as “the tonsils,” are masses of lymphoid tissue, one on each side of the oropharynx. Salivary Glands Figure 2. Salivary glands Parotid gland is the largest salivary gland. It lies in a deep http://bohone09.wikispaces.com/Group+9 hollow behind the ramus of the mandible. The parotid duct (Stenson’s duct) opens into the oral cavity adjacent to the crown of the second upper molar tooth. Parasympathetic ecretomotor supply arises from the glossopharyngeal nerve. Parasympathetic stimulation of the parotid gland produces thin watery saliva. Submandibular gland lies beneath the lower border of the body of the mandible. Parasympathetic secretomotor supply is from the facial nerve. The submandibular duct opens on the summit of a small sublingual caruncle (papilla) beside the base of frenulum of the tongue. Sublingual gland lies beneath the floor of the mouth. The sublingual ducts (8 to 20 in number) open into the mouth. Nerve supply is the same as the submandibular gland. The sublingual gland drains into the oral cavity via numerous small ducts (minor sublingual ducts), which open onto the crest of the sublingual fold (superior margin of the sublingual gland raising as an elongated muscosa). 8 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I Closure of oropharyngeal isthmus Medial and downward movements of palatoglossal & palatopharyngeal arches Upward movement of tongue Downward and forward movement of soft palate 2. PHARYNX The pharynx is a musculofascial half-cylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck. It is the superior expanded part of the alimentary system posterior to the nasal and oral cavities, extending inferiorly past the larynx. The pharyngeal cavity is a common pathway for air and food. The pharynx extends from the cranial base to and is continuous with the top of the esophagus. The walls of the pharynx are attached anteriorly to the margins of the nasal cavities, oral cavity, and larynx. Based on these anterior relationships the pharynx is subdivided into three regions, the nasopharynx, oropharynx, and laryngopharynx: • posterior apertures (choanae) of the nasal cavities open into the nasopharynx; • posterior opening of the oral cavity (oropharyngeal isthmus) opens into the oropharynx; • superior aperture of the larynx (laryngeal inlet) opens into the laryngopharynx. The oral part of the pharynx (oropharynx) is posterior to the oral cavity, inferior to the level of the soft palate, and superior to the upper margin of the epiglottis. It opens anteriorly into the mouth. The oropharynx has a digestive function. The nasal part of the pharynx (nasopharynx) has a respiratory function; it is the posterior extension of the nasal cavities. The Eustachian tube (auditory tube or pharyngotympanic tube) is a tube that links the nasopharynx to the middle ear. The laryngopharynx lies posterior to the larynx and anterior to the vertebral column. The laryngeal inlet opens into the anterior wall of the laryngopharynx. Inferior to the laryngeal inlet, the anterior wall consists of the posterior aspect of the larynx. Pharyngeal Muscles The muscles of the pharynx are organized into two groups based on the orientation of muscle fibers. The constrictor muscles have fibers oriented in a circular direction relative to the pharyngeal wall, whereas the longitudinal muscles have fibers oriented vertically. 9 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I The three constrictor muscles on each side are major contributors to the structure of the pharyngeal wall and their names indicate their position-superior, middle, and inferior constrictor muscles. Posteriorly, the muscles from each side are joined together by the pharyngeal raphe. Anteriorly, these muscles attach to bones and ligaments related to the lateral margins of the nasal and oral cavities and the larynx. Collectively, the muscles constrict or narrow the pharyngeal cavity. When the constrictor muscles contract sequentially from top to bottom, as in swallowing, they move a bolus of food through the pharynx and into the esophagus. All of the constrictors are innervated by the pharyngeal branch of the vagus nerve [X]. The three longitudinal muscles of the pharyngeal wall are named according to their originsstylopharyngeus from the styloid process of the temporal bone, salpingopharyngeus from the cartilaginous part of the pharyngotympanic tube (salpinx is Greek for "tube"), and palatopharyngeus from the soft palate. From their sites of origin, these muscles descend and attach into the pharyngeal wall. The longitudinal muscles elevate the pharyngeal wall, or during swallowing, pull the pharyngeal wall up and over a bolus of food being moved through the pharynx and into the esophagus. These muscles elevate the larynx and shorten the pharynx during swallowing and speaking. Figure 3. Pharynx http://medical-dictionary.thefreedictionary.com/_/viewer.aspx?path=dorland&name=pharynx.jpg 3. WALDEYER'S RING OF LYMPHOID TISSUE The abundant lymphoid tissue in the pharynx forms an incomplete tonsillar ring (Waldeyer’s Ring of Lymphoid Tissue) around the superior part of the pharynx. Collections of lymphoid tissue in the mucosa of the pharynx surrounding the openings of the nasal and oral cavities are part of the body's defense system. The largest of these collections form distinct masses (tonsils). Tonsils occur mainly in four areas: • pharyngeal tonsil, known as adenoids when enlarged, is in the midline on the roof of the nasopharynx; • palatine tonsils are on each side of the oropharynx just posterior to the oropharyngeal isthmus; (The palatine tonsils are visible through the open mouth of a patient when the tongue is depressed.) 10 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I • lingual tonsil refers collectively to numerous lymphoid nodules on the posterior one-third of the tongue. • tubal tonsil is the collection of lymphoid tissue in the submucosa of the pharynx near the pharyngeal opening or orifice of the pharyngotympanic tube. Figure 4. Waldeyer’s Ring of Lymphoid Tissue http://www.sciencedirect.com/science/article/pii/S0169409X01001624 4. OESOPHAGUS The esophagus is a muscular tube about 10 in. (25 cm) long, extending from the pharynx to the stomach. It begins in the neck where it is continuous with the laryngopharynx at the pharyngo-esophageal junction. The esophagus consists of striated (voluntary) muscle in its upper third, smooth (involuntary) muscle in its lower third, and a mixture of striated and smooth muscle in between. The esophagus is a flexible, muscular tube that can be compressed or narrowed by surrounding structures at four locations: 1. junction of the esophagus with the pharynx in the neck; 2. in the superior mediastinum where the esophagus is crossed by the arch of aorta; 3. in the posterior mediastinum where the esophagus is compressed by the left main bronchus; 4. in the posterior mediastinum at the esophageal hiatus in the diaphragm. These constrictions have important clinical consequences. For example, a swallowed object is most likely to lodge at a constricted area. An ingested corrosive substance would move more slowly through a narrowed region, causing more damage at this site than elsewhere along the esophagus. Also, constrictions present problems during the passage of instruments. 5. STOMACH @ epigastric, umbilical, and left hypochondrium regions The stomach is the most dilated part of the gastrointestinal tract and has a J-like shape. It is positioned between the abdominal esophagus and the small intestine. The stomach is divided into four regions: 11 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I cardia, which surrounds the opening of the esophagus into the stomach; fundus of stomach, which is the area above the level of the cardial orifice; body of stomach, which is the largest region of the stomach; pyloric part, which is divided into the pyloric antrum and pyloric canal and is the distal end of the stomach. The most distal portion of the pyloric part of the stomach is the pylorus. It is marked on the surface of the organ by the pyloric constriction and contains a thickened ring of gastric circular muscle, the pyloric sphincter, that surrounds the distal opening of the stomach, the pyloric orifice. The pyloric orifice is just to the right of midline in a plane that passes through the lower border of vertebra LI (the transpyloric plane). greater curvature, a point of attachment for the gastrosplenic ligament and the greater omentum; lesser curvature, a point of attachment for the lesser omentum; cardial notch, superior angle created when the esophagus enters the stomach. The stomach is specialized for the accumulation of ingested food, which it chemically and mechanically prepares for digestion and passage into the duodenum. The stomach acts as a food blender and reservoir; its chief function is enzymatic digestion. The gastric juice gradually converts a mass of food into a semiliquid mixture, chyme (G. juice), which passes fairly quickly into the duodenum. An empty stomach is only of slightly larger caliber than the large intestine; however, it is capable of considerable expansion and can hold 2-3 L of food. The size, shape, and position of the stomach can vary markedly in persons of different body types (bodily habitus) and may change even in the same individual as a result of diaphragmatic movements during respiration, the stomach's contents (empty vs. after a heavy meal), and the position of the person. Figure 5. Esophagus and stomach http://3dsciencepics.com/wp-content/uploads/photos_52CADD54-F9CC-44BE-A86A-ECECA81793A2.jpg 12 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I 6. SMALL INTESTINE The small intestine is the longest part of the gastrointestinal tract and extends from the pyloric orifice of the stomach to the ileocecal fold. This hollow tube, which is approximately 6-7 m long with a narrowing diameter from beginning to end, consists of the duodenum, the jejunum, and the ileum. The small intestine is the primary site for absorption of nutrients from ingested materials. It extends from the pylorus to the ileocecal junction where the ileum joins the cecum (the first part of the large intestine). The pyloric part of the stomach empties into the duodenum, duodenal admission being regulated by the pylorus. Duodenum The duodenum (L. breadth of 12 fingers), the first and shortest (25 cm) part of the small intestine, is also the widest and most fixed part. The duodenum pursues a C-shaped course around the head of the pancreas. The duodenum is divided into four parts: The superior part (first part) extends from the pyloric orifice of the stomach to the neck of the gallbladder. Clinically, the beginning of this part of the duodenum is referred to as the ampulla or duodenal cap, and most duodenal ulcers occur in this part of the duodenum. The descending part (second part) of the duodenum is just to the right of midline and extends from the neck of the gallbladder. This part of the duodenum contains the major duodenal papilla, which is the common entrance for the bile and pancreatic ducts, and the minor duodenal papilla, which is the entrance for the accessory pancreatic duct. The inferior part (third part) of the duodenum is the longest section. The ascending part (fourth part) of the duodenum terminates at the duodenojejunal flexure. This duodenojejunal flexure is surrounded by a fold of peritoneum containing muscle fibers called the suspensory muscle (ligament) of duodenum (ligament of Treitz). Jejunum & Ileum The second part of the small intestine, the jejunum, begins at the duodenojejunal flexure. The third part of the small intestine, the ileum, ends at the ileocecal junction, the union of the terminal ileum and the cecum. Together, the jejunum and ileum are 6-7 m long, the jejunum constituting approximately two fifths and the ileum approximately three fifths of the of the small intestine. Most of the jejunum lies in the left upper quadrant (LUQ), whereas most of the ileum lies in the right lower quadrant (RLQ). The terminal ileum usually lies in the pelvis from which it ascends, ending in the medial aspect of the cecum. Although no clear line of demarcation between the jejunum and ileum exists, they have distinctive characteristics that are surgically important. 13 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I The structure of the small intestine is similar to other regions of the digestive tube, but the small intestine incorporates three features which account for its huge absorptive surface area: Mucosal folds: the inner surface of the small intestine is not flat, but thrown into circular folds, which not only increase surface area, but aid in mixing the ingesta by acting as baffles. Villi: the mucosa forms multitudes of projections which protrude into the lumen and are covered with epithelial cells. Microvilli: the lumenal plasma membrane of absorptive epithelial cells is studded with densely-packed microvilli. Figure 6. Small intestine http://students.cis.uab.edu/ashjones/index3a.html Figure 7. Small intestine-cross section; villi and microvilli http://www.daviddarling.info/encyclopedia/S/small_intestine.html 7. LARGE INTESTINE The large intestine extends from the distal end of the ileum to the anus, a distance of approximately 1.5 m in adults. It absorbs fluids and salts from the gut contents, thus forming feces, and consists of the cecum, appendix, colon, rectum, and anal canal. Beginning in the right groin as the cecum, with its associated appendix, the large intestine continues upward as the ascending colon through the right flank and into the right hypochondrium. Just below the liver, it 14 Dr.Kaan Yücel yeditepeanatomyfhs121.wordpress.com Digestive system – Part I bends to the left, forming the right colic flexure (hepatic flexure), and crosses the abdomen as the transverse colon to the left hypochondrium. At this position, just below the spleen, the large intestine bends downward, forming the left colic flexure (splenic flexure), and continues as the descending colon through the left flank and into the left groin. It enters the upper part of the pelvic cavity as the sigmoid colon, continues on the posterior wall of the pelvic cavity as the rectum, and terminates as the anal canal. The large intestine can be distinguished from the small intestine by: • Omental appendices: small, fatty, omentum-like projections. • Teniae coli: three distinct longitudinal bands. • Haustra: sacculations of the wall of the colon between the teniae • A much greater caliber (internal diameter). Figure 8. Large intestine http://en.wikipedia.org/wiki/File:Gray1223.png Figure 9. Omental appendices, teniae coli, and haustra (coli) http://classes.midlandstech.com/carterp/Courses/bio211/chap23/chap23.htm 15