Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
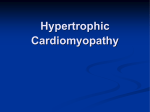
Risk Stratification and Outcome of Patients With Hypertrophic Cardiomyopathy ≥60 Years of Age Barry J. Maron, MD; Ethan J. Rowin, MD; Susan A. Casey, RN; Tammy S. Haas, RN; Raymond H.M. Chan, MD; James E. Udelson, MD; Ross F. Garberich, MS; John R. Lesser, MD; Evan Appelbaum, MD; Warren J. Manning, MD; Martin S. Maron, MD Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Background—Hypertrophic cardiomyopathy (HCM) is prominently associated with risk for sudden death and disease progression, largely in young patients. Whether patients of more advanced age harbor similar risks is unresolved, often creating clinical dilemmas, particularly in decisions for primary prevention of sudden death with implantable defibrillators. Methods and Results—We studied 428 consecutive HCM patients presenting at ≥60 years of age and followed for 5.8±4.8 years; 53% were women. Of the 428 patients, 279 (65%) survived to 73±7 years of age (range, 61–96 years), most (n=245, 88%) with no/mild symptoms, including 135 with ≥1 conventional sudden death risk factors and 50 (37%) with late gadolinium enhancement. Over follow-up, 149 (35%) died at 80±8 years of age, mostly from non--HCM-related causes (n=133, 31%), including a substantial proportion from noncardiac disease (n=54). Sixteen patients (3.7%) had HCMrelated mortality events (0.64%/y), including embolic stroke (n=6), progressive heart failure or transplantation (n=3), postoperative complications (n=2), and arrhythmic sudden death events (n=5, 1.2% [0.20%/y]). All-cause mortality was increased in HCM patients ≥60 years of age compared with an age-matched US general population, predominantly as a result of non--HCM-related diseases (P<0.001; standard mortality ratio, 1.5). Conclusions—HCM patients surviving into the seventh decade of life are at low risk for disease-related morbidity/mortality, including sudden death, even with conventional risk factors. These data do not support aggressive prophylactic defibrillator implantation at advanced ages in HCM. Other cardiac or noncardiac comorbidities have a greater impact on survival than HCM in older patients. (Circulation. 2013;127:585-593.) Key Words: cardiomyopathy ◼ death, sudden ◼ echocardiography ◼ genetics ◼ heart failure ◼ hypertrophy ◼ magnetic resonance imaging H Clinical Perspective on p 593 ypertrophic cardiomyopathy (HCM) is an often unpredictable genetic heart disease associated with a well-acknowledged risk for sudden death (SD), as well as the development of heart failure disability.1–8 Once regarded as a disease most relevant to the young, HCM has been identified with increasing frequency in older patients,9 largely as a result of heightened physician awareness and the availability of advanced imaging modalities.10,11 However, the natural history of older HCM patients is incompletely resolved with respect to risk of adverse events, including heart failure, stroke, and SD. Although SD risk stratification initiatives have identified many young HCM patients likely to benefit from implantable cardioverter-defibrillator (ICD) therapy,12–14 guidelines governing decision making for prophylactic ICDs remain uncertain for older patients surviving decades with HCM, often without symptoms.15 The present study describes the clinical course and risk stratification of a large cohort of patients with HCM beyond the sixth decade of life. Methods Patient Selection Databases of 2 large HCM centers, the Minneapolis Heart Institute Foundation and Tufts Medical Center, identified 428 HCM patients consecutively presenting to these institutions for the first time at ≥60 years of age. Referral to the centers and enrollment in the cohort occurred for the following reasons: to establish or confirm HCM diagnosis (n=78), with or without a family history of the disease, or for targeted subspecialty evaluation, risk stratification, and management considerations (n=350). Most recent clinical assessment was obtained by hospital visit or telephone contact up to November 2011. Mean duration of follow-up was 5.8±4.8 years (range, 3 months to 27 years) from study entry at the first visit to a participating center to the most recent contact or death. The diagnosis of HCM was based on the echocardiographic or cardiovascular magnetic resonance (CMR) demonstration of a hypertrophied and nondilated left ventricle (LV; maximum wall thickness ≥15 mm) in the absence of another Received April 12, 2012; accepted December 17, 2012. From the Hypertrophic Cardiomyopathy Center, Minneapolis Heart Institute Foundation, Minneapolis, MN (B.J.M., S.A.C., T.S.H., R.F.G., J.R.L.); Hypertrophic Cardiomyopathy Center, Tufts Medical Center, Boston, MA (E.J.R., J.E.U., M.S.M.); PERFUSE Core Laboratory and Data Coordinating Center, Harvard Medical School, Boston, MA (R.H.M.C., E.A.); and Department of Medicine, Cardiovascular Division, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA (W.J.M.). Guest Editor for this article was Salvador Borges-Neto, MD. Correspondence to Barry J. Maron, MD, Hypertrophic Cardiomyopathy Center, Minneapolis Heart Institute Foundation, 920 E 28th St, Ste 620, Minneapolis, MN 55407. E-mail [email protected] © 2012 American Heart Association, Inc. Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.112.136085 585 586 Circulation February 5, 2013 cardiac or systemic disease capable of producing similar magnitude of hypertrophy.2,11,15 Each patient had ≥1 of the following disease features characteristic of HCM: (1) LV wall thickness ≥18 mm (n=338); systolic anterior motion of mitral valve (n=266, including 167 with LV outflow gradients ≥30 mm Hg at rest); family history of HCM (n=116, including 57 with HCM-related SD); late gadolinium enhancement (LGE) by contrast CMR not confined to a coronary arterial vascular territory (n=53); surgical septal myectomy/alcohol septal ablation (n=93); LV apical aneurysm with regional scarring (n=11); and sarcomere protein mutations (n=21), including myosin binding protein (n=15), β-myosin heavy chain (n=4), and troponin I (n=2) genes. Coronary arteriograms or computed tomographic angiography was performed on the basis of clinical indications in 286 patients (67%). Atherosclerotic coronary artery disease, defined as ≥50% narrowing in ≥1 epicardial vessels, was present in 84 patients (29%), including 24% of survivors (47 of 198) and 42% who died (37 of 88; P=0.002). Echocardiography Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Transthoracic echocardiographic studies were performed with commercially available instruments. Maximum LV wall thickness was the greatest dimension measured at any site within the LV chamber at end diastole. Left atrial and LV end-diastolic cavity dimensions were assessed by M-mode echocardiography. Peak instantaneous LV outflow gradient was estimated with continuous-wave Doppler under basal conditions. CMR Studies CMR studies were performed with a 1.5-T clinical CMR scanner (Phillips Gyroscan ACS-NT, Best, Netherlands; Sonata or Avanto, Siemens Medical, Erlangen, Germany) in 145 patients.11 Breath-hold cine steady-state free-precession sequences were performed in horizontal long-axis, vertical long-axis, and contiguous short-axis slices with full coverage of LV and slice thicknesses of 10 mm with no gap. Short-axis cine stack was obtained parallel to atrioventricular groove, covering the entire LV chamber. LGE images were acquired 10 to 15 minutes after intravenous administration of 0.2 mmol/kg gadolinium-DTPA (Magnevist, Schering, Berlin, Germany) using breath-held segmented inversion-recovery sequence acquired in the same orientations as the cine images. Mean signal intensity of normal myocardium was calculated, and the threshold exceeding the mean by ≥6 SDs was used to define LGE. Statistical Analysis Descriptive Statistics Data are displayed as mean ± SD for continuous variables and as proportions for categorical variables. When continuous variables had skewed distributions, data were transformed with ln (value +1) to achieve normality. Paired or unpaired Student t tests or 1-way ANOVA assessed statistical significance for continuous variables, with χ2 tests used for categorical variables. Values of P<0.05 were considered significant; all are reported as 2 sided. Statistical calculations were performed with Stata 11.2 (Stata Corp, College Station, TX). Survival Analysis The fraction of HCM patients surviving at each follow-up interval was estimated by the Kaplan-Meier method. The expected fraction surviving at each time interval was computed by assigning to each patient the probability of survival after initial evaluation, appropriate to age and sex, based on US census data.16 Actual and expected surviving fractions were compared by use of the 1-sample log-rank test, which provides a standardized mortality ratio and the 95% confidence interval. Annual mortality rates were calculated for 389 patients with >1 clinical evaluation; the other 39 patients with short follow-up (<3 months) were excluded from this particular analysis. All computations used the survival package (version 2.36-14) of the R software systems, version 2.15.1R (Development Core Team 2012). Results Demographics The 428 study patients were 60 to 91 years old at study entry (mean, 70±7 years); 225 patients (53%) were women (Figure 1). Age at HCM diagnosis was 65±10 years. At the most recent evaluation (or death), patients were 61 to 96 years old (mean, 75±8 years) as follows: 60 to 69 years, n=127; 70 to 79 years, n=172; 80 to 89 years, n=104; and ≥90 years, n=25. A total of 116 patients (27%) had a known family history of HCM. Initial echocardiographic study showed maximum LV wall thickness (usually ventricular septum) of 15 to 33 mm (mean, 20±4 mm); 248 patients (58%) showed ≥20 mm, including 12 with ≥30 mm. Eighty of 89 patients (90%) with LV Figure 1. Clinical outcome in 428 hypertrophic cardiomyopathy (HCM) patients ≥60 years of age at study entry. AF indicates atrial fibrillation; CAD, coronary artery disease; CV, cardiovascular; ICD, implantable cardioverter-defibrillator; OHCA, out-ofhospital cardiac arrest; SD, sudden death; VT/VF, ventricular tachycardia/ventricular fibrillation. *Of these 16 patients, atherosclerotic obstructive CAD was excluded in 15 by computed tomography or coronary angiography (n=10) or by the absence of angina or acute coronary events, traditional cardiovascular risk factors, and Q waves on ECG (n=5). One patient died after septal myectomy and coronary artery bypass surgery. †Operations to relieve left ventricular outflow obstruction (146- and 150-mm Hg gradients at rest) with septal myectomy includes 1 patient with associated CAD and bypass surgery. ‡Transplantation for drug-refractory end-stage heart failure with systolic dysfunction. Maron et al Sudden Death Risk in Elderly HCM Patients 587 70 1.0 65% HCM vs. U.S.; p<0.001 50 0.8 40 30 20 0.24%/y 0.12%/y 0.20%/y 1.4% 0.7% 1.2% NonNon-HCM Embolic Cardiac Cardiac Stroke Death Death Heart Failure* 13% 10 0 Survivors 12% SD † Proportion of Patients Survivin ng % of HCM Cohort 60 0.6 0.4 0.2 HCM Survival (95% CI) U.S. Expected Survival HCM Deaths/Events Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Figure 2. Clinical outcome of hypertrophic cardiomyopathy (HCM) patients first evaluated at ≥60 years of age. SD indicates sudden death. Graph excludes 2 HCM-related operative deaths and 27 others resulting from indeterminate causes. *Includes 1 surviving patient with heart transplantation. †Includes 3 surviving patients with aborted ventricular tachycardia/ventricular fibrillation. ‡Associated atrial fibrillation in 5 of 6 patients. wall thickness of 15 to 17 mm showed ≥1 other clinical features characteristic of HCM: family history of HCM (n=21, including 12 with HCM-related SD); LV outflow gradient ≥30 mm Hg at rest, or systolic anterior motion of mitral valve without obstruction (n=43); LGE by contrast CMR ≥2% of the LV mass (n=9); prior surgical septal myectomy (n=9) or alcohol ablation (n=4); LV apical aneurysm (n=4); and sarcomere protein mutations (n=4). The other 9 patients had atrial fibrillation, a particularly common consequence of HCM.2 Mortality Rates Of 428 patients in the overall cohort, 279 (65%) had survived over the follow-up period to 73±7 years of age (61–96 years); 149 (35%) had died at a mean of 80±8 years of age (61–96 years; Figures 1 and 2). Survival at 5 and 10 years (accounting for all-cause mortality) was 77% (95% confidence interval, 73–82) and 54% (95% confidence interval, 48–62), respectively. Compared with the expected mortality in the US general population, HCM patients ≥60 years of age showed a reduced life expectancy resulting predominantly from non-HCM-related comorbidities (P<0.001; Figure 3). The standard mortality ratio for HCM was 1.5 (95% confidence interval, 1.3--1.8; P<0.001). Univariate predictors of HCM-related mortality were: 1) symptoms at study entry (88% in New York Heart Association (NYHA) classes II and III versus 51% of survivors in class I; P=0.02) and 2) left atrial size (47±8 versus 43±7 mm in survivors; P=0.02). Non--HCM-Related Mortality Of 428 patients, 133 died of non-HCM causes, including 54 who died of noncardiac causes, most commonly cancer (n=28; (Figure 1 and Table 1). In 52 patients, a variety of non-HCM cardiovascular causes, including operative complications, were judged to be primarily responsible for death (Table 1). Of these, 14 had ≥1-vessel obstructive CAD, experiencing acute myocardial infarction (1 patient with myocardial rupture; n=7) or therapeutic intervention, for example, coronary 0.0 0 3 6 9 12 15 51 127 29 137 Years from First Evaluation # at risk: 428 # died: 0 243 51 154 81 89 107 Figure 3. Kaplan-Meier survival curves describing total mortality (death resulting from any cause, including hypertrophic cardiomyopathy [HCM]), at ≥60 years of age among 428 HCM patients, compared with that expected in the US general population after adjustment for age and sex. Dotted lines represent 95% confidence intervals for survival probability. artery bypass surgery or percutaneous transluminal angioplasty/stent (n=8). In the remaining 27 elderly patients, most well beyond normal life expectancy, the precise cause of death (at 82±9 years of age) could not be ascertained with certainty (including 9 patients who died in nursing home environments at 90±6.6 Table 1. Non–Hypertrophic Cardiomyopathy–Related Causes of Death Non-Cardiac (n=54) Cancer Multiorgan Non-HCM Cardiovascular (n= 52) 28 4 Multiorgan, including pulmonary or cardiac (CAD; valvular) comorbidities 32 14 Gastrointestinal bleeding 4 CAD: heart failure/SD* Obstructive pulmonary disease 3 Operative complications Hemorrhagic stroke 3 Brain/abdominal aneurysm 3 Pneumonia/sepsis 3 Blunt trauma/drowning 2 Hepatitis 2 Bowel obstruction 1 Dementia 1 6† CAD indicates coronary artery disease; HCM, hypertrophic cardiomyopathy; and SD, sudden death. *Includes myocardial infarction (n=7), coronary artery bypass surgery (n=3), percutaneous transluminal coronary angioplasty/stent (n=3), and CAD without prior intervention or event (n=1). †Operation-related complications during mitral valve surgery (at 68 and 79 years of age), coronary artery bypass (at 79 years of age), or hip replacement (at 80 years of age), or hemorrhage (n=2; at 73 and 75 years of age). 588 Circulation February 5, 2013 Table 2. Patients With Hypertrophic Cardiomyopathy--Related Deaths/Events Age at Initial Evaluation, y Sex NYHA Age at Death, y Initial Last LVOTG (Rest), mm Hg LV Thickness, mm Risk Factors LGE, % LA, mm EF, % Event/Outcome Sudden death/events 1 60 F 61 1 1 0 20 Syncope, NSVT 14.1 27 55 Alive: ATP for VT 2 61 M 61 3 1 70* 20 NSVT N/A 46 70 Alive: ICD shock for VT† 3 64 M 69 3 N/A 70* 21 0 N/A 41 70 SD 4 mo after myectomy‡ 4 66 F 69 3 1 80* 21 0 N/A 37 65 SD 1 y after myectomy‡ 5 72 M 77 1 1 0 22 Syncope 0 62 60 Alive/out of hospital VF; TH Heart failure and other death/events Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 6 60 M 62 3 1 0 22 Syncope N/A 56 32 Alive: heart transplantation (end stage) 7 64 F 67 2 4 100§ 20 NSVT N/A 47 55 Died: progressive HF 8 65 M 67 2 2 0 22 0 0 49 60 Died: embolic stroke (AF) 9 66 F 66 3 3 146 26 0 N/A 48 wnl Died: postoperative HCM (SM; MVR) 10 67 F 71 3 3 150 20 0 N/A 41 60 Died: postoperative HCM (SM; CABG) 11 68 F 70 3 3 40 20 Syncope; NSVT N/A 48 70 Died: progressive HF 12 71 F 72 2 2 35 25 Family history of SD; syncope N/A 52 80 Died: embolic stroke (AF) 13 77 F 80 2 3 36 20 Syncope N/A 50 70 Died: embolic stroke (AF) 14 78 F 79 2 2 0 28 0 N/A 50 25 Died: embolic stroke (AF);end-stage 15 82 F 84 2 2 54 15 0 N/A 47 65 Died: embolic stroke 16 86 F 86 2 2 0 28 0 N/A 48 60 Died: embolic stroke (AF) AF indicates atrial fibrillation; ATP, antitachycardia pacing; CABG, coronary artery bypass grafting; EF, ejection fraction; HF, heart failure; ICD, implantable cardioverterdefibrillator; LA, left atrium; LGE, late gadolinium enhancement; LV, left ventricle; LVOTG, left ventricular outflow tract gradient; MVR, mitral valve replacement; N/A, not available; NSVT, nonsustained ventricular tachycardia on 24-hour ambulatory (Holter) ECG; NYHA, New York Heart Association; SD, sudden death; SM, surgical myectomy; TH, therapeutic hypothermia; VF, ventricular fibrillation; VT, ventricular tachycardia; and wnl, within normal limits. *LV outflow gradient before myectomy. †Occurred 1 month before myectomy. ‡Patient without conventional SD risk markers; postmyectomy outflow gradient was zero. §Patient elected treatment with dual-chamber pacing, which was ineffective. years of age and up to 96 years of age), although the available information was most consistent with multiorgan involvement and was insufficient to incriminate HCM as the cause of (or a significant contributor to) demise. (n=65), including 41 for whom this was the only marker, and nonsustained ventricular tachycardia (n=59; Table 3). Of 5 patients with SD events, 2 had 1 risk factor and 1 had 2 markers (Tables 2 and 3). HCM-Related Mortality/Adverse Events Mortality events attributable to HCM occurred in 16 patients (3.7%; 0.64%/y) at 72±8 years of age: embolic stroke (n=6; atrial fibrillation in 5 patients, with 2 patients on warfarin), progressive heart failure (n=2), heart transplantation for end-stage disease17 (n=1); postoperative complications (n=2), and arrhythmic SD events (n=5; Figures 1–3 and Table 2). The 5 SD events (1.2%; 0.20%/y) included 3 survivors: 2 with appropriate primary prevention ICD therapy for ventricular tachycardia/ventricular fibrillation at 60 and 61 years of age, and 1 with aborted out-of-hospital cardiac arrest with therapeutic hypothermia at 72 years of age. Coronary artery disease was excluded in each of these 5 patients. Late Gadolinium Enhancement Contrast-enhanced CMR was analyzed in 145 patients 71±6 years old. LGE was present in 53 patients (37%). Among the 135 survivors, LGE occupied 5.2±6.3% of the LV mass (range, 0.2%–29.0%) and was marked (≥10%; range, 10.5%–29%) in 9 patients (7%; Table 3). LGE extent did not differ with respect to most recent NYHA class: 6.2±7.4%, 5.8±5.9%, and 2.9±2.7% for classes I, II, and III, respectively (P=0.7; Figure 4). SD Risk Markers Conventional Risk Factors Among the 279 survivors, 135 (48%) had ≥1 major clinical marker conventionally used to stratify SD risk in HCM pati ents;1,2,7,14,18 144 patients (52%) had no risk marker (Table 3). The most common risk factors were unexplained syncope Heart Failure At the most recent evaluation, most patients (245, 88%) were either asymptomatic (168; class I) or mildly symptomatic (77; class II). Initial and recent NYHA class for the study group did not differ significantly (P=0.18; Figure 5). Of 64 patients who improved during follow-up by ≥1 NYHA class, this change was judged to be attributable primarily to relief of LV outflow obstruction by surgical myectomy (n=37); alcohol septal ablation (n=8); mitral valve replacement (n=2); pharmacological treatment (β-blockers, verapamil, disopyramide; ≥1 211 135 8 3 Patients, n 428 279 16# 5 2 6 96 149 1 1 2 33 49 2 110 57 39 1 0 13 6 0 0 1 4 65 Syncope Family History of HCM SD >3 20* 90 59 3 2 12 6 0 0 1 1 15 ABPR NSVT LV Thickness ≥30 mm Patients With Individual Risk Factor, n 2(40) 9(56) 108(39) 165(39) LVOTG ≥30 mm Hg (Rest), n (%) 53/145(37) 50/135‖ (37) 1/3(33) 1/2(50) 190(44) 107(38) 11(69) 3(60) 21‡ 17 0 0 72† 53§ 3 7 LGE, n (%) AF, n (%) Alcohol Ablation, n 1/2 1/3 9/135(7) 11/145(8) LGE ≥10%, n (%) 14 14 5.2±6.3 5.7±6.6 LGE, % ABPR indicates abnormal blood pressure response (to exercise); AF, atrial fibrillation; LGE, late gadolinium enhancement; LV, left ventricular; LVOTG, left ventricular outflow tract gradient; NSVT, nonsustained ventricular tachycardia (on 24-hour ambulatory [Holter] ECG; ≥3 beats at >120 bpm); and SD, sudden death. *Of 87 patients studied with exercise (stress) echocardiography. †Includes 13 patients with surgical myectomy performed before the first visit to the participating institution at ≥60 years of age. ‡Includes 2 patients with (failed) alcohol septal ablation performed before the first visit to the participating institution at ≥60 years of age who later underwent surgical myectomy. §Includes 3 patients with myectomy performed before the first visit to the participating institution at ≥60 years of age. ‖Includes 1 patient with cardiovascular magnetic resonance after alcohol septal ablation (LGE=5.2%). ¶Includes 4 nonfatal events: 3 patients with life-threatening events aborted by an implantable cardioverter-defibrillator (ICD) or external defibrillation for out-of-hospital cardiac arrest and 1 other patient with heart transplantation for refractory failure. #Of these 16 patients, obstructive atherosclerotic coronary artery disease was excluded in 15 by either selective coronary or computed tomography angiography (n=10) or absence of angina, acute coronary events, traditional cardiovascular risk factors, and Q-waves on ECG (n=5). The remaining patient died after septal myectomy and coronary artery bypass surgery. **Includes 3 patients with ICD-aborted SD events or defibrillation for cardiac arrest. HCM SD/events** All HCM deaths/events¶ Survivors All patients Patient Subset Risk Factors, n Myectomy, n Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Table 3. Markers of Increased Sudden Death Risk in Hypertrophic Cardiomyopathy Patients ≥60 Years of Age Maron et al Sudden Death Risk in Elderly HCM Patients 589 A B ** * RV RV RV LV LV C * D LV RA LV LA Figure 4. Cine and contrast-enhanced cardiovascular magnetic resonance images in hypertrophic cardiomyopathy (HCM) patients ≥60 years of age. A, Left ventricular (LV) short-axis slice from a 66-year-old woman with massive LV hypertrophy involving the anterior septum (36 mm; asterisks) extending into the anterolateral wall. B, Contrast-enhanced LV short-axis slice from a 73-year-old woman with a localized area of transmural late gadolinium enhancement (LGE) in the basal anterior septum (arrows). C, Four-chamber slice from a 67-year-old woman with hypertrophy confined to the LV apex (asterisks). D, Four-chamber slice from a 71-year-old-woman with transmural LGE of septum (small arrows) and posterobasal free wall (large arrows). LA indicates left atrium; RA, right atrium; and RV, right ventricle. n=14); percutaneous transluminal coronary angioplasty for obstructive CAD (n=1); and radiofrequency ablation for atrial fibrillation (n=2). Thirty-four patients were in NYHA classes III and IV at the last evaluation, primarily because of atrial fibrillation (n=12), obstructive pulmonary disease (n=4), CAD complications (n=2), or noncardiopulmonary disease (n=1). In 15 other patients, severe symptoms persisted despite myectomy or alcohol ablation or because those interventions were withheld as a result of patient preference. LV Outflow Obstruction LV outflow obstruction at rest (gradient, 30–180 mm Hg; average, 73±31 mm Hg)5 was present at study entry in 165 patients (39%). Sixteen of these patients had outflow gradients (assessed by echocardiography) of 75±41 mm Hg, 5.6±1 years earlier at 63±6 years of age, compared with a gradient of 70±32 mm Hg on study entry at 69±6 years of age (P=0.65). Age at HCM Diagnosis To ascertain whether age at diagnosis was relevant to disease presentation or outcome, patients identified with HCM at <60 and ≥60 years of age were compared (Table 4). Earlier diagnosis at <60 years of age was associated with slightly greater LV wall thickness and end-diastolic dimension, but more frequent atrial fibrillation and male predominance (Table 4). 590 Circulation February 5, 2013 Most Recent Evaluation Initial Evaluation NYHA FC-1 NYHA FC-2 142* 69 123 41 168 77 Table 4. Relation of Age at Diagnosis to Clinical Features and Outcome in Hypertrophic Cardiomyopathy Parameter Age <60 y Age ≥60 y at Diagnosis at Diagnosis P Value Patients, n (%) 112 (26) 316 (74) Male, n (%) 66 (59) 137 (43) Age diagnosis, y 52±7.7 69±6.8 0.005 LVOT gradient ≥30 mm Hg at rest, n (%) 47 (42) 118 (37) 0.39 Left atrium, mm 45±8.4 43±8.3 0.02 LVED, mm 44±6.8 42±7.1 0.01 Maximum LV thickness, mm 21+3.6 20±3.6 0.01 Atrial fibrillation, n (%) 64 (57) 126 (40) 0.002 1 46 (41) 140 (44) 0.20 2 30 (27) 101 (32) 3/4 36 (32) 75 (24) 1 59 (53) 148 (47) 2 36 (32) 95 (30) 3/4 17 (15) 73 (23) NYHA, initial evaluation, n (%) NYHA FC-3/4 68 24 34 Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 NYHA, last evaluation, n (%) Figure 5. Changes in symptom level (New York Heart Association functional class [NYHA FC]) from initial to most recent evaluation in 279 surviving patients. *Includes 1 patient with surgical myectomy 1 year before the first evaluation. †Includes 2 patients with alcohol ablation and 2 patients with myectomy performed before the first evaluation. Age at diagnosis did not affect HCM-related mortality or NYHA class. Associated Systemic Hypertension Fifty-six patients (13%) had associated hypertension based on blood pressure ≥140/90 mm Hg recorded on the first visit, a history of hypertension for >3 years, or a history of antihypertensive drug administration (including at initial visit). HCM patients with and without hypertension did not differ with respect to demographic and clinical variables; hypertension did not enhance mortality risk (Table 5). Discussion Sudden unexpected death is a well-recognized and devastating consequence of HCM.1–4,12,15 Risk stratification markers have demonstrated strong predictive power in identifying many susceptible children, adolescents, and adults who have benefited from the introduction of prophylactic ICD therapy to this disease.1,12–14 However, HCM patients of more advanced age beyond midlife are recognized with increasing frequency because of the heightened index of suspicion for this disease and the increasing penetration of high-resolution diagnostic imaging such as CMR11 and cardiac computed tomographic angiography.10 The influx of older HCM patients often recognized for the first time, and frequently with conventional SD risk factors,1 has created unique clinical decision-making and management uncertainties, particularly with respect to recommendations for primary prevention ICDs.12 To confront these difficult clinical scenarios, we assembled the present large HCM cohort of advanced age and assessed them with respect to demographics, clinical and imaging profiles, risk stratification models, and natural history. The present data in >400 patients, selected by virtue of achieving age ≥60 years at the first visit to the participating 0.21 Mortality, n (%) HCM-related 6/31 (19) 10/118 (8) Non-HCM 25/31 (81) 108/118 (92) 0.08 HCM indicates hypertrophic cardiomyopathy; LV, left ventricular; LVED, left ventricular end-diastolic dimension; LVOT, left ventricular outflow tract; and NYHA, New York Heart Association functional class. institutions, provide novel insights into the natural history of HCM. For example, the common perception among patients that the course of HCM is one of unwavering progression throughout a lifetime is not supported by our data. Indeed, although this cohort cannot take into consideration higher-risk patients who may have died earlier in life, it nevertheless supports the principle that achieving older age in a genetic disease such as HCM may itself convey relative protection from ongoing SD risk and afford more favorable prognosis—that is, for many patients, their underlying HCM (present for >6 decades) has largely declared its natural history. This principle is underscored by the relatively low HCM-related SD event rate of 0.20%/y (in the absence of CAD). Three of these 5 patients with SD events survived ventricular tachycardia/ventricular fibrillation by virtue of prophylactically implanted ICDs or external defibrillation that appropriately terminated ventricular tachyarrhythmias (for a true HCM SD mortality rate of only 0.08%/y).12,13,15 In contrast, the most common cause of HCM-related death was embolic stroke associated with atrial fibrillation, underscoring the importance of considering anticoagulation therapy early in such HCM patients. In a subgroup of 27 patients (6% of the overall cohort), it was not possible to reliably ascertain the true contribution (if any) of HCM to demise from the available evidence. Of note, however, these patients were of particularly advanced age (mean, 82±9 years), including 9 who died while under nursing home care and surveillance at 90 years of age on average (and well past estimated life expectancy). Furthermore, the available evidence was most consistent with multiorgan Maron et al Sudden Death Risk in Elderly HCM Patients 591 Table 5. Comparison of Clinical and Demographic Features in Hypertrophic Cardiomyopathy Patients With and Without Systemic Hypertension Hypertension-Negative Hypertension-Positive 372 (87) 56 (13) Age at HCM diagnosis, y 64±10 (15–91) 66±8 (49–84) 0.15 Age at first evaluation, y 70±7 (60–91) 71±7 (60–84) 0.21 176 (47) 27 (48) 0.90 20.6±4 (15–33) 20.4±3.6 (15–33) 0.72 Patients, n (%) Male, n (%) Maximum LV thickness, mm P Value Atrial fibrillation, n (%) 167 (45) 23 (41) 0.59 LVOT gradient ≥30 mm Hg at rest, n (%) 150 (40) 18 (32) 0.24 1 161 (43) 25 (45) 2 113 (30) 18 (32) ¾ 98 (26) 13 (23) 1 180 (48) 27 (48) 2 115 (31) 16 (29) ¾ 77 (21) 13 (23) HCM-related 13/119 (11) 3/30 (10) Non HCM-related 106/119 (89) 27/30 (90) NYHA, initial evaluation, n (%) 0.88 NYHA, last evaluation, n (%) Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 0.89 Mortality, n (%) 0.88 HCM indicates hypertrophic cardiomyopathy; LV, left ventricle; LVOT, left ventricular outflow tract; and NYHA, New York Heart Association functional class. involvement and was insufficient to incriminate HCM as the cause of (or a significant contributor to) demise. Even with these patients considered HCM-related deaths, the calculated mortality rate was only 1.7%/y. In this study population with relatively low HCM-related mortality, we nevertheless identified a substantial proportion of patients with those risk factors conventionally associated with susceptibility to life-threatening arrhythmias.1–3,15 About 50% of our overall cohort had ≥1 risk markers, including about one half of those patients surviving to the end of the follow-up period (achieving 73 years of age on average). These findings underscore the important principle that clinical markers that convey predictive power for SD in younger HCM patients do not necessarily assume the same significance in patients who have achieved more advanced ages. We should emphasize that the weight afforded syncope in risk stratification of older HCM patients remains a difficult area.7 In the present cohort, unexplained syncope (ie, judged likely nonneurocardiogenic in origin) was particularly common, affecting ≈50% of those patients with risk factors (including one third in whom syncope was the sole potential marker). Massive LV hypertrophy (wall thickness ≥30 mm), a SD risk marker in younger patients,4,19 was uncommon (<3%) in our present cohort but nevertheless demonstrated compatibility with advanced age.4 Similarly, ≈40% of our patients achieved advanced age despite LV outflow gradients (average, 73 mm Hg), underscoring that many patients tolerate these gradients for extensive periods of time. LGE on contrast CMR (presumably a marker for myocardial fibrosis) has been advanced as a potential predictor of SD events and progressive heart failure.18,20–22 However, a large proportion (ie, almost 40%) of our surviving patients had areas of LGE, including some with substantial hyperenhancement. Although the time at which LGE developed in these patients is unknown, recognition that many HCM patients survive to normal or near-normal longevity with myocardial fibrosis raises some skepticism concerning LGE as a risk marker in this age group. In the present cohort, the HCM-related death/event rate owing to progressive heart failure, embolic stroke, or SD (0.64%/y) was less than reported in other HCM cohorts encompassing a broader age range,23 as well as the estimated annual mortality risk in the general population >60 years of age (ie, ≈2%).16 Furthermore, the study cohort demonstrated a large measure of stability over the follow-up period with only 2 deaths (and 1 heart transplantation) and with almost 80% of the surviving patients reporting no or only mild heart failure symptoms at their most recent evaluation. Finally, our observation that 47 survivors benefited from septal reduction procedures with relief of severe symptoms and achieved the advanced age of >70 years on average is consistent with the principles that myectomy is associated with extended survival indistinguishable from that expected in the general population24 and that both surgery and ablation are effective in reducing heart failure symptoms.1,2,15,24–26 Notably, Kaplan-Meier analysis showed that total mortality in these HCM patients exceeded that expected in the general population but was due largely to other associated cardiovascular diseases (particularly CAD), and noncardiac conditions (eg, cancer) that are prevalent at the advanced 592 Circulation February 5, 2013 Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 ages achieved by these patients. Indeed, such comorbidity posed a greater threat to survival than long-standing HCM itself. This observation that prognosis in older HCM patients may be based largely on comorbidities has the effect of shifting the clinical focus at advanced ages to non-HCM diseases. Whether HCM is a passive bystander or has a potentially deleterious interaction with other diseases in this age group is unresolved.8,27 Alternatively, this relationship may have been influenced by selection bias, with HCM patients having significant comorbidities more likely to come to clinical recognition. The patient cohort reported here constitutes the experience of 2 large HCM centers for which some patient referral selection bias was unavoidable. Therefore, typical of all hospital-based cohort studies in HCM,28 we cannot be certain that our data are entirely representative of the general HCM population. Nevertheless, we would anticipate that in a purely unselected HCM cohort uncontaminated by referral bias (and no longer accessible in this disease),28 susceptibility for SD would be similar to and certainly no higher than that reported here. In addition, although survival to older ages and normal longevity have been recognized in HCM,9,28–30 prior data in this age group are encumbered by limited study designs, relatively small cohorts, and selected patient populations that did not specifically address risk stratification.9,23,29,30 Conclusions In a large HCM cohort, advanced age itself appears to mitigate disease-related complications, including death resulting from progressive heart failure or SD even in the presence of conventional risk markers and LGE. This represents a shift in perception of HCM, once regarded as a progressive disorder at any age (and throughout life), with aging in effect representing a negative risk factor for many patients. The data presented here propose an inverse relationship between advanced age and disease-related risk in HCM, inevitably affecting management decision making. Recommendations for primary prevention ICDs in older HCM patients should be made on a case-by-case basis with prudent restraint. In such HCM patients, non--HCM-related cardiac and noncardiac competing modes of death convey disproportionate impact on mortality and pose a greater threat to longterm survival than HCM alone. These observations underscore the importance of attention to the overall clinical environment with aggressive identification of coexistent disease. Disclosures Dr B.J. Maron serves as a consultant for GeneDx and has received grant/research support from Medtronic. Dr M.S. Maron serves as a consultant/is on the advisory board for PGx and GeneDx. The other authors report no potential conflicts. References 1. Maron BJ. Contemporary insights and strategies for risk stratification and prevention of sudden death in hypertrophic cardiomyopathy. Circulation. 2010;121:445–456. 2. Maron BJ, Maron MS. Hypertrophic cardiomyopathy [published online ahead of print August 3, 2012]. Lancet. doi:10.1016/S0140-6736(12) 60397-3. 3. Elliott PM, Poloniecki J, Dickie S, Sharma S, Monserrat L, Varnava A, Mahon NG, McKenna WJ. Sudden death in hypertrophic cardiomyopathy: identification of high risk patients. J Am Coll Cardiol. 2000;36:2212–2218. 4. Spirito P, Bellone P, Harris KM, Bernabo P, Bruzzi P, Maron BJ. Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. N Engl J Med. 2000;342:1778–1785. 5.Maron MS, Olivotto I, Betocchi S, Casey SA, Lesser JR, Losi MA, Cecchi F, Maron BJ. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003;348:295–303. 6. Spirito P, Autore C, Rapezzi C, Bernabò P, Badagliacca R, Maron MS, Bongioanni S, Coccolo F, Estes NA, Barillà CS, Biagini E, Quarta G, Conte MR, Bruzzi P, Maron BJ. Syncope and risk of sudden death in hypertrophic cardiomyopathy. Circulation. 2009;119:1703–1710. 7. Melacini P, Basso C, Angelini A, Calore C, Bobbo F, Tokajuk B, Bellini N, Smaniotto G, Zucchetto M, Iliceto S, Thiene G, Maron BJ. Clinicopathological profiles of progressive heart failure in hypertrophic cardiomyopathy. Eur Heart J. 2010;31:2111–2123. 8. Ball W, Ivanov J, Rakowski H, Wigle ED, Linghorne M, Ralph-Edwards A, Williams WG, Schwartz L, Guttman A, Woo A. Long-term survival in patients with resting obstructive hypertrophic cardiomyopathy comparison of conservative versus invasive treatment. J Am Coll Cardiol. 2011;58:2313–2321. 9. Maron BJ, Casey SA, Hauser RG, Aeppli DM. Clinical course of hypertrophic cardiomyopathy with survival to advanced age. J Am Coll Cardiol. 2003;42:882–888. 10. Knickelbine T, Lesser JR, Haas TS, Brandenburg ER, Gleason-Han BK, Flygenring B, Longe TF, Schwartz RS, Maron BJ. Identification of unexpected nonatherosclerotic cardiovascular disease with coronary CT angiography. JACC Cardiovasc Imaging. 2009;2:1085–1092. 11. Maron MS, Maron BJ, Harrigan C, Buros J, Gibson CM, Olivotto I, Biller L, Lesser JR, Udelson JE, Manning WJ, Appelbaum E. Hypertrophic cardiomyopathy phenotype revisited after 50 years with cardiovascular magnetic resonance. J Am Coll Cardiol. 2009;54:220–228. 12. Maron BJ, Spirito P, Shen WK, Haas TS, Formisano F, Link MS, Epstein AE, Almquist AK, Daubert JP, Lawrenz T, Boriani G, Estes NA 3rd, Favale S, Piccininno M, Winters SL, Santini M, Betocchi S, Arribas F, Sherrid MV, Buja G, Semsarian C, Bruzzi P. Implantable cardioverterdefibrillators and prevention of sudden cardiac death in hypertrophic cardiomyopathy. JAMA. 2007;298:405–412. 13.Maron BJ, Spirito P. Implantable defibrillators and prevention of sudden death in hypertrophic cardiomyopathy. J Cardiovasc Electrophysiol. 2008;19:1118–1126. 14. Woo A, Monakier D, Harris L, Hill A, Shah P, Wigle ED, Rakowski H, Rozenblyum E, Cameron DA. Determinants of implantable defibrillator discharges in high-risk patients with hypertrophic cardiomyopathy. Heart. 2007;93:1044–1045. 15. Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW; American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; American Society of Echocardiography; American Society of Nuclear Cardiology; Heart Failure Society of America; Heart Rhythm Society; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:e783–e831. 16. Therneau TM, Offord J. Expected Survival Base on Hazard Rates (Update), 1999. Rochester, MN: Mayo Clinic; 1999. Mayo Clinical Biostatistics Technical Report 63. 17. Harris KM, Spirito P, Maron MS, Zenovich AG, Formisano F, Lesser JR, Mackey-Bojack S, Manning WJ, Udelson JE, Maron BJ. Prevalence, clinical profile, and significance of left ventricular remodeling in the end-stage phase of hypertrophic cardiomyopathy. Circulation. 2006;114:216–225. 18.Rubinshtein R, Glockner JF, Ommen SR, Araoz PA, Ackerman MJ, Sorajja P, Bos JM, Tajik AJ, Valeti US, Nishimura RA, Gersh BJ. Characteristics and clinical significance of late gadolinium enhancement by contrast-enhanced magnetic resonance imaging in patients with hypertrophic cardiomyopathy. Circ Heart Fail. 2010;3:51–58. 19. Olivotto I, Gistri R, Petrone P, Pedemonte E, Vargiu D, Cecchi F. Maximum left ventricular thickness and risk of sudden death in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2003;41:315–321. 20. O’Hanlon R, Grasso A, Roughton M, Moon JC, Clark S, Wage R, Webb J, Kulkarni M, Dawson D, Sulaibeekh L, Chandrasekaran B, Bucciarelli-Ducci Maron et al Sudden Death Risk in Elderly HCM Patients 593 C, Pasquale F, Cowie MR, McKenna WJ, Sheppard MN, Elliott PM, Pennell DJ, Prasad SK. Prognostic significance of myocardial fibrosis in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2010;56:867–874. 21. Maron MS, Appelbaum E, Harrigan CJ, Buros J, Gibson CM, Hanna C, Lesser JR, Udelson JE, Manning WJ, Maron BJ. Clinical profile and significance of delayed enhancement in hypertrophic cardiomyopathy. Circ Heart Fail. 2008;1:184–191. 22. Maron BJ, Maron MS, Lesser JR, Hauser RG, Haas TS, Harrigan CJ, Appelbaum E, Main ML, Roberts WC. Sudden cardiac arrest in hypertrophic cardiomyopathy in the absence of conventional criteria for high risk status. Am J Cardiol. 2008;101:544–547. 23. Maron BJ, Olivotto I, Spirito P, Casey SA, Bellone P, Gohman TE, Graham KJ, Burton DA, Cecchi F. Epidemiology of hypertrophic cardiomyopathyrelated death: revisited in a large non-referral-based patient population. Circulation. 2000;102:858–864. 24.Ommen SR, Maron BJ, Olivotto I, Maron MS, Cecchi F, Betocchi S, Gersh BJ, Ackerman MJ, McCully RB, Dearani JA, Schaff HV, Danielson GK, Tajik AJ, Nishimura RA. Long-term effects of surgical septal myectomy on survival in patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2005;46:470–476. 25. Maron BJ, Dearani JA, Ommen SR, Maron MS, Schaff HV, Gersh BJ, Nishimura RA. The case for surgery in obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2004;44:2044–2053. 26.Nagueh SF, Groves BM, Schwartz L, Smith KM, Wang A, Bach RG, Nielsen C, Leya F, Buergler JM, Rowe SK, Woo A, Maldonado YM, Spencer WH 3rd. Alcohol septal ablation for the treatment of hypertrophic obstructive cardiomyopathy: a multicenter North American registry. J Am Coll Cardiol. 2011;58:2322–2328. 27. Sorajja P, Ommen SR, Nishimura RA, Gersh BJ, Berger PB, Tajik AJ. Adverse prognosis of patients with hypertrophic cardiomyopathy who have epicardial coronary artery disease. Circulation. 2003;108:2342–2348. 28. Maron BJ, Casey SA, Poliac LC, Gohman TE, Almquist AK, Aeppli DM. Clinical course of hypertrophic cardiomyopathy in a regional United States cohort. JAMA. 1999;281:650–655. 29. Lewis JF, Maron BJ. Elderly patients with hypertrophic cardiomyopathy: a subset with distinctive left ventricular morphology and progressive clinical course late in life. J Am Coll Cardiol. 1989;13:36–45. 30. Maron BJ, Casey SA, Haas TS, Kitner CL, Garberich RF, Lesser JR. Hypertrophic cardiomyopathy with longevity to 90 years or older. Am J Cardiol. 2012;109:1341–1347. Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Clinical Perspective Hypertrophic cardiomyopathy (HCM) is the most common cause of sudden death in the young and is responsible for heart failure and stroke-related disability and death in adults of all ages. Although HCM is known to be compatible with normal longevity, a common perception also remains that this disease is ultimately associated with unrelenting progression throughout a patient’s lifetime. Therefore, whether patients of more advanced ages harbor disease-related risks similar to young patients is unresolved. By assembling and analyzing 428 HCM patients presenting at ≥60 years of age to 2 major centers, we were able to clarify the natural history of this complex disease at more advanced ages. Over follow-up, 279 patients (65%) survived to 73±7 years of age, and 149 (35%) died at 80±8 years. Only 16 patients (3.7%) had HCM-related mortality events (0.64%/y), including embolic stroke (n=6), progressive heart failure or transplantation (n=3), postoperative complications (n=2), and arrhythmic sudden death events (n=5, including 2 who died; 0.2%/y). Notably, all-cause mortality was increased compared with a matched US general population, predominantly resulting from non--HCM-related causes. Consequently, these data suggest an inverse relationship between the inherent risks from HCM and achieving advanced age, with survival itself generally declaring lower-risk status. Patients surviving into the seventh decade with this genetic disease are at low risk for HCM-related mortality and morbidity, including sudden death (even when conventional risk factors are present). These data do not support aggressive prophylactic defibrillator implantation at advanced ages for HCM patients. Indeed, in such older patients, other cardiac or noncardiac comorbidities, as competing modes of death, pose a greater threat to long-term survival. Risk Stratification and Outcome of Patients With Hypertrophic Cardiomyopathy ≥60 Years of Age Barry J. Maron, Ethan J. Rowin, Susan A. Casey, Tammy S. Haas, Raymond H.M. Chan, James E. Udelson, Ross F. Garberich, John R. Lesser, Evan Appelbaum, Warren J. Manning and Martin S. Maron Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Circulation. 2013;127:585-593; originally published online December 30, 2012; doi: 10.1161/CIRCULATIONAHA.112.136085 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2012 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/127/5/585 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/