Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
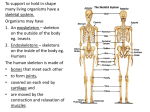
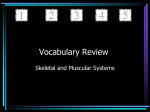
Università degli Studi di Catania Facoltà di Medicina e Chirurgia Corso di laurea in Fisioterapia Equipollenza THE MUSCULOSKELETA L SYSTEM Inglese Scientifico Prof.ssa Mariagrazia Torrisi THE MUSCULOSKELETAL SYSTEM 15 October 2008 Phsiotherapy lesson 1 INTRODUCTION MUSCLES BONES JOINTS LIGAMENTS TENDONS AND BURSAS 1 2 There are three types of muscles: skeletal smooth cardiac (heart). Two of these kinds—skeletal and smooth—are part of the musculoskeletal system. The musculoskeletal system provides form, stability and movement to the human body. It consists of the body's bones (which make up the skeleton), muscles, tendons, ligaments, joints, cartilage, and other connective tissue. tissue The term "connective tissue" is used to describe the tissue that supports and binds tissues and organs together. Its chief components are elastic fibers and collagen, a protein substance Phsiotherapy lesson 1 Phsiotherapy lesson 1 MUSCLES Introduction 15 October 2008 15 October 2008 skeletal muscles is what most people think of as muscle, the type that can be contracted to move the various parts of the body. Skeletal muscles are bundles of contractile fibers that are organized in a regular pattern, so that under a microscope they appear as stripes (hence, they are also called striped or striated muscles). Skeletal muscles vary in their speeds of contraction. Skeletal muscles, which are responsible for posture and movement, are attached to bones and arranged in opposing groups around joints. For example, muscles that bend the elbow (biceps) are countered by muscles that straighten it (triceps). These countering movements are balanced. The balance makes movements smooth, which helps prevent damage to the musculoskeletal system. Skeletal muscles are controlled by the brain and are considered voluntary muscles because they operate with a person's awareness. The size and strength of skeletal muscles are maintained or increased by regular exercise. In addition, growth hormone and testosterone help muscles grow in childhood and maintain their size in adulthood. 3 15 October 2008 Phsiotherapy lesson 1 4 Muscoloskeletal system(front view) Smooth muscles Smooth muscles control certain bodily functions that are not readily under a person's control. Smooth muscle surrounds many arteries and contracts to adjust blood flow. It surrounds the intestines and contracts to move food and feces along the digestive tract. Smooth muscle also is controlled by the brain but not voluntarily. The triggers for contracting and relaxing smooth muscles are controlled by the body's needs, so smooth muscles are considered involuntary muscle because they operate without a person's awareness. Cardiac muscle Cardiac muscle forms the heart and is not part of the musculoskeletal system. Like skeletal muscle, cardiac muscle has a regular pattern of fibers that also appear as stripes under a microscope. However, cardiac muscle contracts and relaxes rhythmically without a person's awareness. 15 October 2008 Phsiotherapy lesson 1 5 15 October 2008 ) Phsiotherapy lesson 1 6 BONES Muscoloskeletal system(back view • Bone, although strong, is a constantly changing tissue that has several functions. Bones serve as rigid structures to the body and as shields to protect delicate internal organs. They provide housing for the bone marrow, where the blood cells are formed. Bones also maintain the body's reserve of calcium. In children, some bones have areas called growth plates. Bones lengthen in these areas until the child reaches full height, at which time the growth plates close. Thereafter, bones grow in thickness rather than in length, based on the body's need for additional bone strength in certain areas. • Bones have two shapes: flat (such as the plates of the skull and the vertebrae) and tubular (such as the thighbones and arm bones, which are called long bones). All bones have essentially the same structure. The hard outer part (cortical bone) consists largely of proteins, such as collagen, and a substance called hydroxyapatite, which is composed mainly of calcium and other minerals. Hydroxyapatite is largely responsible for the strength and density of bones. The inner part of bones (trabecular bone) is softer and less dense than the hard outer part. Bone marrow is the tissue that fills the spaces in the trabecular bone. Bone marrow contains specialized cells (including stem cells) that produce blood cells. Blood vessels supply blood to the bone, and nerves surround the bone. • Bones undergo a continuous process known as remodeling (see Osteoporosis). In this process, old bone tissue is gradually replaced by new bone tissue. Every bone in the body is completely reformed about every 10 years. To maintain bone density and strength, the body requires an adequate supply of calcium, other minerals, and vitamin D and must produce the proper amounts of several hormones, such as parathyroid hormone, growth hormone, calcitonin, estrogen, and testosterone. . Activity (for example, weight-bearing exercises for the legs) helps bones strengthen by remodeling. With activity and optimal amounts of hormones, vitamins, and minerals, trabecular bone develops into a complex lattice structure that is lightweight but strong. • Bones are covered by a thin membrane called the periosteum. Injury to bone transmits pain because of nerves located mostly in the periosteum. Blood enters bones through blood vessels that enter through the periosteum. 15 October 2008 Phsiotherapy lesson 1 7 15 October 2008 Phsiotherapy lesson 1 8 JOINTS • • • According to their structure and the range of movements they allow, Joints are the junction between two or more bones. Some joints do not normally move, such as those located between the plates of the skull. Other joints allow a large and complex range of motion. The configuration of a joint determines the degree and direction of possible motion. For example, the shoulder joints, which have a balland-socket design, allow inward and outward rotation as well as forward, backward, and sideways motion of the arms. Hinge joints of the knees, fingers, and toes allow only bending (flexion) and straightening (extension There are two important kinds of joint with quite different functions. Between the secondary centres of ossification or epiphyses of the bones and the metaphyses are joints where movement is positively discouraged: between the femur and the tibia is the synovial knee joint proper, where movement is positively encouraged. So where two or more bones come together we find a joint: the range of movement at joints may be zero or a just a little give, or extremely large. The components of joints provide stability and reduce the risk of damage from constant use. In a joint, the ends of the bones are covered with cartilage—a smooth, tough, resilient, and protective tissue composed of collagen, water, and proteoglycans that reduces friction as joints move. (Collagen is a tough fibrous tissue; proteoglycans are substances that provide the cartilage's resilience.) Joints also have a lining synovial tissue) that encloses them to form the joint capsule. Cells in the synovial tissue produce a small amount of clear fluid (synovial fluid), which provides nourishment to the cartilage and further reduces friction while facilitating movement 15 October 2008 Phsiotherapy lesson 1 9 joints are classified into: FIBROUS AND CARTILAGINOUS JOINTS where two bones are separated by a deformable intermediate Fibrous joints. Sutures Gomphoses Syndesmosis: SYNOVIAL JOINTS where one surface slides freely over another 15 October 2008 FIBROUS JOINTS • Phsiotherapy lesson 1 10 SYNOVIAL JOINTS Fibrous joints. The joint between the bony shaft and cartilage at the ends of long bones. is a synchondrosis, a cartilage sandwich with bone on either side: bone and cartilage fit together perfectly and the whole thing is cup shaped. If movement occurs the growing bone will be damaged (slipped epiphysis) and this is countered by putting in a long nail to fix it again. Sutures: are limited to the skull. They resemble a synchondrosis, but with fibrous tissue instead of cartilage between the bones. Sutures are necessary for skull growth: consequently well marked in the young less so in the adult. The only movement in sutures is at birth when the cranial bones overlap to allow passage through the maternal pelvis. After this movement is discouraged by increasing complexity of the suture, which becomes serrated or denticulate. Later in life, when growth is complete they fuse. gomphoses: are peg and socket joints as seen between teeth and jaws. The joint is maintained by the periodontal ligament which gives only a little to act as a shock absorber when we bite on a ball bearing. syndesmosis: only one of these in the body, the inferior tibio-fibular joint. In this type there is a little movement, limited by a tight ligament. Since many joints are limited by ligaments this is probably a special definition we can do without. symphysis: two bones united by cartilage, but designed to give a bit. The symphysis pubis with ligaments and fibrocartilage is normally closed, but opens in childbirth due to hormonal influences. 15 October 2008 Phsiotherapy lesson 1 11 Inside the knee............. • The knee is designed for its own protection. It is completely surrounded by a joint capsule that is flexible enough to allow movement but strong enough to hold the joint together. The capsule is lined with synovial tissue, which secretes synovial fluid to lubricate the joint. Wear-resistant cartilage covering the ends of the thighbone (femur) and shinbone (tibia) helps reduce friction during movement. Pads of cartilage (menisci) act as cushions between the two bones and help distribute body weight in the joint. Fluid-filled sacs (bursas) provide cushioning between structures such as the tibia and the tendon attached to the kneecap (patellar tendon). Five ligaments along the sides and the back of the knee reinforce the joint capsule, adding stability. The kneecap (patella) protects the front of the joint. 15 October 2008 Phsiotherapy lesson 1 12 Synovial joints have different parameters. Joint surfaces almost in contact but discontinuous, as a great range of movement is often possible, and the surfaces slide over each other. The sliding surfaces are covered with a thin layer of cartilage. This gives a coefficient of friction of <0.002. The joint cavity is sealed by a synovial membrane which secretes synovial fluid, a lubricant and nutrient. Around this, in turn, is a tough fibrous joint capsule which keeps the ends of the bones in proper orientation. This is often locally thickened to form joint ligaments. The synovial cavity is very small between articular surfaces but larger round the edges where it may form a bursa, a sack-like extension which may be in contact with the joint cavity. Various inclusions may be present in the joint cavity: a tendon may pass through, sheathed in synovial membrane. Fat pads may be present, packing the large gaps which occur in some joints between bone ends. Pieces of cartilage are also found, in addition to articular cartilage. These may form 1. a labrum or lip deepening a bony socket 2. menisci - incomplete discs or crescents increasing the size of articular surfaces 3. complete, or nearly complete articular discs of fibrocartilage. This will convert a joint into two in parallel, which can then move in independent directions. The temporomandibular joint of the jaw is a good example of this. 15 October 2008 Phsiotherapy lesson 1 13 Movements in synovial joints. These can be very extensive.The shoulder joint is particularly free and able to move around three axes. Various schemes of classification of synovial joints have been used according to; •Complexity Many joints possess only two articular surfaces and are therefore simple. Usually one surface is convex or larger than the other and termed male. Compound joints have more than one pair of articulating surfaces (e.g. the elbow has two male surfaces on the humerus which articulate with female surfaces on radius and ulna) and are thus compound. Complex joints have an intracapsular disc or menisci. •Degrees of freedom A joint which moves substantially in one plane (like an elbow) is uniaxial. One which moves in two planes is biaxial, one which moves in three is triaxial. A ball and socket is multiaxial, but is equivalent to a triaxial as it has three degrees of freedom i.e. all movements can be reduced to XYZ axes. Not a good classification as there are often small but vital movements in other planes (e.g. knee rotation at end of flexing) and cannot . take account of sliding movement 15 October 2008 • • • Shape Probably the most widely used classification, but still tries to simplify. Surfaces hinge joints: permit flexion and extension (knee) pivot joints: allow rotation (superior radioulnar) plane joints: have flat surfaces and allow gliding in several directions (carpus and tarsus) condylar joints: usually regarded as two hinge joints with separate articulations (TMJ) saddle joints: have surfaces shaped like two saddles - allow movement in two planes at right angles and a little rotation (base of thumb) ball and socket: allows very free movement around any axis through ball (hip) ellipsoid: ball and sockets which are not round : rotation therefore impossible (radiocarpal joint) Functional approach. This is the best classification as regards understanding what is going on. All above classifications are approximations and have holes in them which fit uneasily. joint movement is always made up of:– – – – gliding - of one surface over another- slide angulation - flexion, extension etc. - roll rotation about axis of bone - spin approximation of soft parts. 15 October 2008 Phsiotherapy lesson 1 15 • Phsiotherapy lesson 1 14 Movement always occurs at articular surfaces, which are never planes nor spheres nor cones but always spheroids egg shapes, either male or female i.e. convex or concave. A point moving between A and B on a surface can take the shortest great circle route a chord, or can take a longer, prettier arc. Any movement can be described by a trigone (a bendy triangle) or three arcs. The imaginary point which traces these movements is the end of the axis of rotation. In the simplest case this is the end of the long axis of the bone: for something like a femur it obviously isn't. Lets try this on a real movement, extending the knee. If we hold the tibia still and move the femur extension has three bits. – the femur rolls on the tibia – the femur slides posteriorly – the femur spins to lock the joint. The third of these is most important because it tells us something about how joints work. Take an egg and cut it in half. The resulting curved surface has a variable radius of curvature. If we try to fit this to another spheroid we see that it only fits well at one point. Elsewhere there are wedgeshaped gaps and smaller areas of contact. Joints exploit this: the position of best fit, or close packed position usually occurs at the end of the range of habitual movement. As a joint approaches this position ligaments are stretched and often some spin is imparted by them to screw the joint home. In this position the joint is virtually 15 October 2008 Phsiotherapy lesson 1 16 LIGAMENTS • abolished: in practice it is only fully reached under strain and may damage articular surfaces and pull ligaments. So usually it is approached but not realised. This position is comfortable because it uses little muscular energy and can be maintained for long periods. The loose packed position is also important because it allows – loosely fitting surfaces to spin, roll and slide – a reduced area of contact, so little friction – wedge shaped gaps, continually changing circulate synovial fluid like a peristaltic pump. • Limitation of movement is also important. Usually achieved by – tension in ligament, which have strain and pain receptors – tension of muscles around a joint - passive resistance to stretch followed by reflex contraction when stimuli from mechanoreceptors becomes critical. These explain Hilton's law: that joints and the muscles acting on them share a nerve supply. Paralysis of muscles thus affects joints. In spastic paralysis muscle tone is increased and movement restricted. In other paralyses joints become lax, flail joints or actually disrupted. Charcot elbow in syphilis. – Running out of articular surface. – approximation of soft parts. 15 October 2008 Phsiotherapy lesson 1 17 Ligaments are tough fibrous cords composed of connective tissue that contains both collagen and elastic fibers. The elastic fibers allow the ligaments to stretch to some extent. Ligaments surround joints and bind them together. They help strengthen and stabilize joints, permitting movement only in certain directions. Ligaments also connect one bone to another (such as inside the knee). 15 October 2008 TENDONS AND BURSAS 18 Nerve/Muscle Connections • Tendons are tough bands of connective tissue made up mostly of a rigid protein called collagen. Tendons firmly attach each end of a muscle to a bone. They are often located within sheaths, which are lubricated to allow the tendons to move without friction. • • Bursas are small fluid-filled sacs that can lie under a tendon, cushioning the tendon and protecting it from injury. Bursas also provide extra cushioning to adjacent structures that otherwise might rub against each other, causing wear and tear—for example, between a bone and a ligament or a bony prominence and overlying skin (such as in the elbow, kneecap, or shoulder area). • Tendonitis is the inflammation, irritation, and swelling of a • Phsiotherapy lesson 1 tendon. It can occur as a result of injury, overuse, or with aging as the tendon loses elasticity. Any action that places prolonged repetitive strain on the forearm muscles can cause tendonitis. The most common symptom of tendonitis is pain, tenderness, and the increase of pain with movement. Nerves, known as sensory neurons, come from every part of the body to carry impulses to the brain or spinal cord concerning the condition of every nook and cranny in the body, including the muscles. In the same way, motor neurons send impulses to the muscles, often through intermediate connections or "interneurons" in the spinal cord. These messages cross the gap at a junction between nerves and muscles, setting off a chain of events that ends in contraction. Within a second, millions of impulses reach the motor neurons. Some of the impulses are sent from various parts of the brain and spinal cord; some come from sense organs located in the joints, ligaments, and tendons; and some come from the muscles themselves. The seeds of movement are sown by the brain, in its primary cortex, an area of the brain's wrinkled surface which spans both cerebral hemispheres. Another patch of cortex directly in front of the primary area also houses neurons which are involved in movement. This area is thought to be important to speech and delicately coordinated movements such as those performed by the hand. Electrical impulses from many regions of the brain feed into the motor areas. The brain must collect and analyze all the sensory messages it receives before it can direct a coordinated movement. This interplay is continuous and elaborate sight, sound, smell, pressure and pain are all important, but so are messages bringing information about the angles and position of joints, the length and tension of muscles, or even the speed of movements. At every point along the descent from brain to muscle, impulses can influence interneurons to vary the precision of muscular control. An average motor neuron may have as many as 15,000 connections each, providing information from all over the body. Some parts, like the back, which have a limited precision of motion, are only equipped with a few - perhaps 50,000. Hand muscles, which perform very delicate and precise movements are driven by about 200,000 neurons. A second major transmission network produces contractions of groups of muscles and is responsible for larger muscular functions, such as running, walking or swimming. A "muscle spindle" is a sensory end organ in a muscle that is sensitive to stretching of the muscle. • 15 October 2008 Phsiotherapy lesson 1 19 15 October 2008 Phsiotherapy lesson 1 20 Nerve/muscles connection Nerve/Muscle Connections 15 October 2008 Phsiotherapy lesson 1 21