Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Plasmodium falciparum wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Influenza A virus wikipedia , lookup
Ebola virus disease wikipedia , lookup
Neonatal infection wikipedia , lookup
Antiviral drug wikipedia , lookup
Marburg virus disease wikipedia , lookup
West Nile fever wikipedia , lookup
Oesophagostomum wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Hepatitis C wikipedia , lookup
Henipavirus wikipedia , lookup
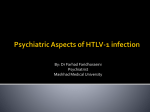
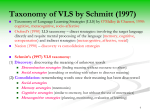
MAJOR ARTICLE Higher Human T Lymphotropic Virus (HTLV) Provirus Load Is Associated with HTLV-I versus HTLV-II, with HTLV-II Subtype A versus B, and with Male Sex and a History of Blood Transfusion Edward L. Murphy,1,2 Tzong-Hae Lee,2 Daniel Chafets,2 Catharie C. Nass,3,a Baoguang Wang,4 Katharine Loughlin,4 and Donna Smith,4 for the HTLV Outcomes Study Investigatorsb 1 Departments of Laboratory Medicine and Epidemiology/Biostatistics, University of California, San Francisco, and 2Blood Systems Research Institute, San Francisco; 3American Red Cross Blood Services, Chesapeake and Potomac Region, Baltimore, and 4Westat, Rockville, Maryland Background. High human T lymphotropic virus (HTLV)–I provirus load (VL) has been associated with an increased risk of HTLV-associated myelopathy, but little is known about variation in HTLV-I or -II VLs by demographic characteristics and risk behaviors. Methods. We measured HTLV-I and HTLV-II VLs in a large cohort of 127 HTLV-I–seropositive and 328 HTLV-II–seropositive former blood donors, by use of real-time polymerase chain reaction using tax primers. Multivariable linear regression was used to control for confounding by relevant covariates. Results. The mean VLs were 3.28 log10 copies/106 peripheral blood mononuclear cells (PBMCs) (range, 0.5– 5.3 log10 copies/106 PBMCs) for HTLV-I and 2.60 log10 copies/106 PBMCs (range, 0.05–5.95 log10 copies/106 PBMCs) for HTLV-II (P ! .0001). HTLV-II VLs were higher in those subjects with subtype A infection (mean, 2.82 log10 copies/106 PBMCs) than in those with subtype B infection (mean, 2.29 log10 copies/106 PBMCs) (P p .005). Higher HTLV-I VL was associated with previous receipt of a blood transfusion (P p .04 ), and lower HTLV-II VL was associated with female sex (P p .007 ). These associations persisted in virus-specific multivariate linear regression models controlling for potential confounding variables. Conclusions. VL was significantly higher in HTLV-I than in HTLV-II infection and was higher in HTLV-II subtype A than in HTLV-II subtype B infection. Chronic HTLV VLs may be related to the infectious dose acquired at the time of infection, with higher VLs following acquisition by blood transfusion and lower VLs following sexual acquisition. Human T lymphotropic virus (HTLV) types I and II are human type C retroviruses derived most likely from simian-to-human transmission thousands of years ago [1, 2]. The 2 HTLV types share ∼60% nucleotide ho- Received 24 December 2003; accepted 18 February 2004; electronically published 6 July 2004. Financial support: National Heart, Lung, and Blood Institute Retrovirus Epidemiology Donor Study (research contracts N01-HB-97077 [superseded by N01-HB47114], N01-HB-97078, N01-HB-97079, N01-HB-97080, N01-HB-97081, N01-HB97082, and R01-HL-62235 [through the HTLV Outcomes Study]). a Present affiliation: C.C.N. is retired from the American Red Cross Blood Services, Chesapeake and Potomac Region. b HOST investigators are listed after the text. Reprints or correspondence: Dr. Edward L. Murphy, c/o Blood Centers of the Pacific, UCSF, 270 Masonic Ave., San Francisco, CA 94118 ([email protected]). The Journal of Infectious Diseases 2004; 190:504–10 2004 by the Infectious Diseases Society of America. All rights reserved. 0022-1899/2004/19003-0012$15.00 504 • JID 2004:190 (1 August) • Murphy et al. mology but differ in their epidemiology and disease associations. HTLV-I is prevalent in Africa, the Caribbean, Brazil, and southern Japan and causes adult T cell leukemia (ATL) and HTLV-associated myelopathy (HAM) [3]. HTLV-II is prevalent among Amerindians, African pygmies, and injection drug users (IDUs) in the Americas and Europe and has been linked to HAM, as well as to a higher occurrence of pneumonia and bronchitis [4, 5]. HTLV-II subtype A is more prevalent among North American and European IDUs and their sex partners, whereas subtype B is more prevalent among Native Americans [4]. HTLV-I and -II viral RNA is low to undetectable in human serum, and viral propagation is thought to occur via the clonal expansion of lymphocytes with integrated proviral DNA [6] or the transfer of viral RNA via direct contact between infected and uninfected cells [7]. How the level of proviral DNA in lymphocytes is regulated is unknown but may involve either the activity of the viral transactivator protein Tax, which differs between HTLV-I and some HTLV-II subtypes [8], or the degree of lymphocyte turnover in the infected host [6]. High levels of HTLV-I proviral DNA, HTLV-I Tax mRNA, and anti-HTLV antibody have been associated with the occurrence of HAM [9, 10]. However, the pathogenic mechanism is unresolved and may be due to either direct viral neurotoxicity [11], an autoimmune response directed at viral proteins homologous to neuronal proteins [12], or “bystander” immunologic damage to neural tissue [13]. Data are less clear with regard to the association between HTLV-I provirus load (VL) and ATL, with one study showing significantly higher prediagnostic VLs in patients with ATL than in asymptomatic carriers [14] and another showing an association between high HTLV-I VLs and the presence of abnormal lymphocytes thought to be indicative of preleukemia, although this was not proven prospectively [15]. HTLV-II VL has received comparatively less study than HTLVI VL. One study found no difference in HTLV-II VLs between IDUs and endemic African Pygmies and no correlation between HTLV-II VLs and CD8+ lymphocyte counts or stage of AIDS, in the IDUs who were coinfected with HIV [16]. Other studies have found high HTLV-II VLs in patients with HIV/HTLV-II coinfection [17, 18] and, notably, in coinfected patients with sensory neuropathy [19]. HTLV-II VLs also increased after the initiation of antiretroviral therapy for HIV in coinfected patients [20, 21]. HTLV-II VL has not been correlated with age or sex, and neither HTLV-I VL nor HTLV-II VL has been studied in relation to the route of infection. We therefore measured HTLV-I and HTLV-II VLs in a well-characterized cohort of former blood donors and correlated these levels with data on demographic characteristics, risk factors for infection, and HTLV-II subtype. SUBJECTS AND METHODS Study design and population. The present study was a crosssectional analysis of blood samples obtained at the baseline visit of the HTLV Outcomes Study cohort, formerly known as the Retrovirus Epidemiology Donor Study HTLV cohort. The study protocol was approved by the Committee on Human Research at the University of California, San Francisco, and by institutional review boards at other participating institutions. Enrollment criteria and methods have been reported in detail elsewhere [22–24]. In brief, blood donors found to be HTLV seropositive during predonation screening at 5 centers across the United States in 1988–1992 had confirmation of seropositivity performed by use of Western blot, followed by HTLV typing by use of type-specific antibody or polymerase chain reaction (PCR) assays [25]. All subjects were seronegative for HIV at baseline. Demographic, risk factor, and health history information was obtained by interview with trained study coordinators. HTLV-II subtypes were determined previously by use of restriction fragment–length polymorphism analysis [26]. Laboratory methods. Peripheral blood mononuclear cell (PBMC) samples were stored at ⫺70C until used, and PBMCs were digested in a PCR solution with proteinase K. Quantitation of proviral DNA of HTLV-I and HTLV-II was performed by use of real-time PCR. We used a single set of primers for both HTLV-I and -II, from highly conserved sequences of the viral tax regions, designated as HTLV-F5 (5-CGG ATA CCC IGT CTA CGT GTT T-3) and HTLV-R4 (5-CTG AGC IGA IAA CGC GTC CA-3). To quantitate the cellular input for each reaction, HLA-DQ-a copy number was measured separately. The primers used for HLA-DQ-a were GH26 (5-GTG CTC CAG GTG TAA ACT TGT ACC AG-3) and GH27 (5-CAC GGA TCC GGT AGC AGC GGT AGA GTT G-3). For each sample, 25 mL of DNA lysate was added to the PCR mixture (5 mL for the HLA-DQ-a reactions). Real-time PCR was performed by use of the GeneAmp 5700 machine (Applied Biosystems), with the following cycle conditions: 10 min at 95C, followed by 45 cycles of 30 s at 95C, 30 s at 64C, and 45 s at 72C. Reactions were performed in triplicate [27]. Fluorescense intensity of Syber green incorporated into the amplified product was measured at every PCR cycle, and the threshold cycle number of each sample was recorded. For each run, a standard curve was generated from 1:10 serial dilutions of MT2 (HTLV-I; obtained from American Type Culture Collection) or MoT (HTLV-II) cell lines, with a range of 10⫺1–104 copies/reaction. Mean HTLV copy numbers for these cell lines were 2.1 HTLV-I copies/cell for MT2, as determined elsewhere [28], and 11.7 HTLV-II copies/cell for MoT, determined experimentally using HTLV-II plasmids of known concentration (provided by J. Kropp, Gladstone Institute of Virology and Immunology, San Francisco, CA, and E. Wattel, Centre Leon Bernard, Lyon, France). The number of copies in the test sample was then calculated by interpolation of the experimentally determined threshold cycle number onto the control standard regression curve. To determine the VL of each sample, the number of copies of HTLV-I or HTLV-II was divided by the HLA-DQ-a copy number. The lower limit of detection for the assay was 1 copy/105 cells. Reproducibility of the assay was measured by testing 40 specimens in duplicate and comparing the results, by use of linear regression with R 2 p 0.97. Statistical analysis. VLs, expressed as HTLV-I or -II copies per 106 PBMCs, were log10 transformed for all analyses, to approximate the normal distribution. Undetectable VLs were assigned the value of 1 copy/106 cells, which is below the lower limit of detection of the VL assay, before log10 transformation. Means, SEs, and ranges were calculated for each HTLV type and in subsets defined by demographic and risk factor variables. HTLV-I and -II Provirus Load • JID 2004:190 (1 August) • 505 Table 1. Demographic and risk factor profile of the study population from the baseline visit of the HTLV Outcomes Study. Variable All subjects Age, years !20 20–29 30–39 40–49 50–59 ⭓60 Sex Female Male Race/ethnicitya White Black Hispanic Asian Other/unspecified Lifetime no. of sex partnersa !4 5–8 9–20 ⭓21 History of IDUa No Yes History of sex with an IDUa No/unlikely Yes/likely History of blood transfusiona No Yes NOTE. user. HTLV-I HTLV-II 127 (100) 328 (100) 2 9 25 55 16 20 (2) (7) (20) (43) (13) (16) 2 19 144 110 35 18 (1) (6) (44) (34) (11) (5) 93 (73) 34 (27) 243 (74) 85 (26) 46 54 6 15 4 (36) (43) (5) (12) (3) 112 107 86 6 14 (34) (33) (26) (2) (4) 42 31 38 14 (33) (24) (30) (11) 73 81 89 78 (22) (25) (27) (24) 125 (98) 1 (1) 243 (74) 84 (26) 104 (82) 10 (8) 136 (42) 182 (55) 85 (67) 42 (33) 251 (77) 69 (21) Data are no. (%) of subjects. IDU, injection drug HTLV-II group. A greater proportion of subjects with HTLVI than subjects with HTLV-II had !4 lifetime sex partners, whereas a greater proportion of subjects with HTLV-II admitted to having had 120 partners. A history of IDU was reported by 25% of the subjects with HTLV-II (48 men and 36 women), although only ∼1% said they currently injected drugs. More than half of the subjects with HTLV-II (37 men and 145 women) reported (yes or likely) sexual intercourse with an IDU. Onethird of the HTLV-I group and one-fifth of the HTLV-II group had a history of blood transfusion; in comparison, !10% of HTLV-seronegative blood donors enrolled in the cohort reported such a history. VLs for both viral types ranged from 0.05 to 5.95 log10 copies/ 6 10 PBMCs. HTLV-I VLs (mean [SE], 3.28 [0.12] log10 copies/ 106 PBMCs) were significantly higher than HTLV-II VLs (mean [SE], 2.60 [0.09] log10 copies/106 PBMCs; P ! .0001; figure 1A and 1B). Among subjects with HTLV-II, HTLV-II VLs were significantly higher in the 190 subjects with subtype A (mean [SE], 2.82 [0.11] log10 copies/106 PBMCs), compared with the 138 subjects with subtype B (mean [SE], 2.29 [0.15] log10 copies/106 PBMCs; P p .005; figure 2D). All analyses by demographic and risk factor variables were performed separately for HTLV-I and for HTLV-II. HTLV-I VLs were lower in white (mean [SE], 3.03 [0.22] log10 copies/106 PBMCs) than in nonwhite (mean [SE], 3.48 [0.14] log10 copies/106 PBMCs) subjects, although this difference was not statistically significant (P p .08 ; figure 2A). HTLVI VLs were higher in those with a history of blood transfusion (mean [SE], 3.62 [0.14] log10 copies/106 PBMCs) than in those without a history of blood transfusion (mean [SE], 3.1 [0.16] log10 copies/106 PBMCs; P p .04; figure 2B). HTLV-I VLs did not differ significantly by age, sex, number of sex partners, a Nos. may not add to totals, because of missing data (!10% per variable). Differences in log10 VLs between groups were tested by use of 2-sample t tests. Associations between log10 VLs and each continuous variable were tested by use of separate linear regression models. Finally, multivariate linear regression models were constructed to assess independent associations between variables found to be significantly associated in the univariate analyses. All analyses were performed using SAS statistical software (version 8.2; SAS Institute). RESULTS VLs and epidemiologic data were available for 127 subjects with HTLV-I and 328 subjects with HTLV-II (∼85 % of the HTLV cohort). Demographic and risk factor characteristics of the subjects are presented in table 1. Most subjects were middle-aged and women, and there was a substantial proportion of black persons in both HTLV groups and of Hispanic persons in the 506 • JID 2004:190 (1 August) • Murphy et al. Figure 1. Difference in human T lymphotropic virus (HTLV) provirus load (VL) between HTLV-I– and HTLV-II–infected subjects (P ! .0001), from the baseline visit of the HTLV Outcomes Study (HOST). VL is presented as median (central line), 25th and 75th percentiles (box boundaries), and 10th and 90th percentiles (error bars). PBMCs, peripheral blood mononuclear cells. Figure 2. Human T lymphotropic virus (HTLV) provirus load (VL) presented as median (central line), 25th and 75th percentiles (box boundaries), and 10th and 90th percentiles (error bars). A, HTLV-II VL by HTLV-II subtype A vs. B (P p .005). B, HTLV-II VL by sex (P p .007). C, HTLV-I VL by nonwhite vs. white race/ethnicity (P p .08). D, HTLV-I VL by history of blood transfusion (P p .04). PBMCs, peripheral blood mononuclear cells. history of IDU, or history of sex with an IDU. In the multivariate linear regression analysis, HTLV-I VL retained its association with a history of blood transfusion (b p 0.68; P p .02) but had only a borderline association with white race (b p ⫺0.51; P p .06). HTLV-II VLs were significantly lower among women (mean [SE], 2.45 [0.10] log10 copies/106 PBMCs) than among men (mean [SE], 3.02 [0.18] log10 copies/106 PBMCs; P p .007; figure 2C). There was no association between HTLV-II VL and age, race, number of sex partners, history of IDU, or history of sex with an IDU. In the multivariate linear regression analysis, HTLVII VL remained independently and inversely associated with female sex (b p ⫺0.68; P p .01) and positively associated with HTLV-II subtype A (b p 0.54; P p .008). In an analysis restricted to women only, there was an inverse association between HTLV-II VL and increasing number of sex partners (b p ⫺0.22; P p .03), which did not persist after adjusting for other covariates (b p ⫺0.18; P p .12), although the association with HTLV-II subtype A remained (b p 0.65; P p .004). DISCUSSION The present study of HTLV VLs at the baseline visit of a large cohort of generally asymptomatic former blood donors found that HTLV-I VLs were significantly higher than HTLV-II VLs and that HTLV-II VLs were significantly higher in subtype A than in subtype B infections. Analyses by demographic and behavioral characteristics revealed higher HTLV-I VLs in those subjects with a history of blood transfusion and borderline lower HTLV-I VLs in white subjects. HTLV-II VLs were significantly lower in women than in men. There was a borderline association of lower VLs with increasing numbers of sex partners, but this did not persist after adjusting for covariates. HTLV-I VLs have been reported in numerous studies, ranging from !1 copy/10,000 lymphocytes to 11 copy/10 lymphocytes [6, 9, 10, 14]. The results of the present study are consistent with those of previous reports, with a mean HTLV-I VL of ∼1000 copies/106 PBMCs and a range of 1–100,000 copies/ 106 PBMCs. By use of an end-point dilution PCR assay, a previous study revealed VLs of 20–200,000 copies/106 PBMCs in 49 subjects with HTLV-II, with and without HIV coinfection [17]. A competitive PCR assay found 50–162,390 copies/106 PBMCs in Italian IDUs [16], and those with the highest VLs were found to have clonal expansion of HTLV-II–infected lymphocytes [29]. These VL results are also similar to those of the present study. In the only other comparative study of HTLV-I and HTLVHTLV-I and -II Provirus Load • JID 2004:190 (1 August) • 507 II VLs that we were able to find, Kaplan et al. reported that HTLV-I VLs were significantly higher than HTLV-II VLs [27]. Their study included a subset of individuals from the present study but used a different assay to measure VLs. The present report is the only published in vivo study of HTLV-II VLs according to HTLV-II subtype. Differences in VLs between HTLV-I and HTLV-II, and between HTLV-II subtype A and subtype B, may be related to differences in tax gene structure and protein expression among the HTLV types and subtypes. HTLV-II Tax has been shown to have a lower transforming activity than HTLV-I Tax [30], which may account for the lack of leukemogenesis by HTLV-II. Compared with HTLV-II subtype B, HTLV-II subtype A has less ability to inhibit p53 function in T lymphocytes [8, 31] and to induce CREB- and NFkB–mediated transactivation [32]. These in vitro data would suggest lower VLs in HTLV-II subtype A infection, which is the opposite of our finding. One explanation may be that tax genes from wild-type HTLV-II subtype A isolates may have different biologic activity than the HTLV-II prototypes commonly used for in vitro experiments [31–33]. It is also possible that differences in VLs between HTLV types and subtypes are due to differences in modes of transmission or to host factors, and not to biological characteristics of each virus. The association of higher HTLV-I VLs with a history of blood transfusion is the most suggestive evidence we found that the route of infection affects HTLV VLs. Fully 34% of our HTLVI cohort had received a blood transfusion, compared with 10% of our HTLV-seronegative comparison group, which is consistent with our previous report of blood transfusion as a risk factor for infection (adjusted odds ratio, 4.5; 95% confidence interval, 2.6–7.8) [34]. These same subjects with HTLV-I and a history of blood transfusion have now been shown to have higher VLs than subjects with HTLV-I without this risk factor. Blood transfusion is associated with a higher dose of HTLV-I– infected lymphocytes, so it is biologically plausible that VLs are higher. Since VLs have been shown to remain relatively constant over time [35], one may infer that a higher infecting dose from blood transfusion translates to a higher persistent VL, such as those detected in our subjects. Alternatively, altered immune function from comorbid illness or severe trauma at the time of blood transfusion could have affected the VL set point. Our data are consistent with those of a previous report of median HTLV-I VLs of 100–200 copies/105 PBMCs in the first year after blood transfusion–transmitted infection in a Jamaican study [14]. However, in the same study, asymptomatic carriers had higher HTLV-I VLs (median, ∼1000 copies/105 PBMCs) than did asymptomatic carriers in the present study, perhaps because of a higher proportion of mother-to-child infection. HTLV-II VLs were significantly lower in women than in men. Two previous studies of HTLV-I VLs found no differences by sex among asymptomatic carriers [9, 36], but we were unable 508 • JID 2004:190 (1 August) • Murphy et al. to find other published reports of differences in HTLV-II VLs by sex. Other reports found that women with HAM have either higher or lower HTLV-I VLs than do men with HAM [9, 10]. Women are clearly overrepresented among both patients with HTLV-I HAM and patients with HTLV-II HAM [37]. Previous epidemiological data suggest that sexual acquisition of HTLVI is associated with development of HAM, whereas mother-tochild acquisition is associated with ATL [38, 39]. We therefore hypothesize that women are more likely to acquire HTLV-II sexually, with a smaller infectious dose, and, hence, to have lower VLs than men, most of whom acquire the virus by parenteral (IDU or blood transfusion) or motherto-child routes. Against this hypothesis are data from the present study, which has showed no association between HTLV-II VLs and the lifetime number of sex partners or history of sex with an IDU, for both sexes. However, in an analysis limited to women, we did find a nonsignificant trend toward lower HTLV-II VLs with increasing number of lifetime sex partners. Retrospective interview data may not be the most accurate in assigning the actual mode of transmission. In support of the hypothesis are data showing lower mean HTLV-I VLs in 11 cases of sexually acquired HTLV-I, compared with the 11 transmitting persons [40]. That infectious dose may predict the chronic set point for VLs is consistent with the observation that expansion of HTLV within an infected human is predominantly due to clonal expansion of lymphocytes with integrated HTLV provirus [6]. Thus, the number of initially infected lymphocytes would influence the number of lymphocyte clones, although the size of each clone may depend on factors that cause multiplication of lymphocytes. Recent data from the Wattel laboratory support this hypothesis, in that humans with presumed breast-milk acquisition of HTLV-II as infants had increased clonality and VLs, compared with those with risk factors suggesting infection acquired later in life [41]. An alternative explanation is that infection during infancy or childhood produces higher VLs because of a weaker initial immune response. The borderline association we found between lower HTLVI VLs and white race may be explained either by genetic background or by route of infection associated with a particular racial group. Bangham et al. have previously reported that HTLV-I VLs may be correlated with specific HLA subtypes [42] and that these subtypes are also associated with an increased risk of developing HAM. Since HLA phenotypes differ by racial origin, it is conceivable that the race/ethnicity association we observed is due to genetic background. On the other hand, other host characteristics, such as route of HTLV infection, lymphocyte activation, and concomitant infections, may also differ by race. It has been recognized that the incidence of HTLV-associated diseases, such as ATL, may differ between endemic Japanese and Jamaican populations, perhaps because of differences in biologic response to infection [23]. Furthermore, comparative studies across race and ethnicity populations using similar methodologies to measure VL and controlling for route of infection and HLA type should help resolve this issue. Strengths of the present study include the use of a welldefined, generally asymptomatic group of human subjects and a sensitive, reproducible, and high-throughput assay to measure VLs. Potential weaknesses include the relatively large variability of VLs and the fact that the differences in VLs, although statistically significant, were of relatively small magnitude, compared with the interpersonal range of observed values. Determining causality for the associations we observed is also problematic in this cross-sectional study, since different characteristics of the subjects (i.e., race/ethnicity and mode of acquisition) may be confounded. That associations persisted after multivariable analysis is reassuring but not definitive. In conclusion, we have demonstrated associations between higher HTLV-I VLs and history of blood transfusion and, perhaps, nonwhite race and between lower HTLV-II VLs and female sex. Discovering the biological determinants of VL is important because the incidence of HTLV-associated diseases seems to be related to VL. Although reasons for the race/ethnicity association remain speculative, we hypothesize that associations with sex and history of blood transfusion result from a biological relationship between infectious dose of HTLV-I and HTLV-II and the chronic VL measured in an individual. Further studies in humans with well-defined time and mode of infection or experimental studies in animals are required to investigate this hypothesis. HTLV OUTCOMES STUDY (HOST) MEMBERS The HOST is presently the responsibility of the following persons. Study headquarters. University of California, San Francisco (San Francisco, CA): E. L. Murphy (Principal Investigator) and J. Engstrom. Blood centers. American Red Cross Blood Services Greater Chesapeake and Potomac Region (Baltimore, MD): C. C. Nass, C. Conry-Cantilena, and J. Gibble; American Red Cross Blood Services Southeastern Michigan Region (Detroit, MI): B. Newman; American Red Cross Blood Services Southern California Region (Los Angeles, CA): G. Garratty, S. Hutching, and A. Ziman; Blood Centers of the Pacific (San Francisco, CA): M. P. Busch; and Oklahoma Blood Institute (Oklahoma City, OK): J. W. Smith and E. Moore. Medical coordinating center. Westat (Rockville, MD): G.B. Schreiber, D. Ameti, and B. Wang. Central laboratory. Blood Centers of the Pacific (San Francisco, CA): M. P. Busch and L. H. Tobler. Diagnostic review panel. E. L. Murphy, R. Sacher, and J. Fridey. References 1. Cann AJ, Chen ISY. Human T-cell leukemia virus types I and II. In: Fields B, ed. Virology. 2nd ed. New York: Raven Press, 1990:1501–27. 2. Slattery JP, Franchini G, Gessain A. Genomic evolution, patterns of global dissemination, and interspecies transmission of human and simian T-cell leukemia/lymphotropic viruses. Genome Res 1999; 9:525–40. 3. Manns A, Hisada M, La Grenade L. Human T-lymphotropic virus type I infection. Lancet 1999; 353:1951–8. 4. Hall WW, Ishak R, Zhu SW, et al. Human T lymphotropic virus type II (HTLV-II): epidemiology, molecular properties, and clinical features of infection. J Acquir Immune Defic Syndr Hum Retrovirol 1996; 13(Suppl 1):S204–14. 5. Murphy EL. The clinical epidemiology of human T-lymphotropic virus type II (HTLV- II). J Acquir Immune Defic Syndr Hum Retrovirol 1996; 13(Suppl 1):S215–9. 6. Wattel E, Vartanian JP, Pannetier C, Wain-Hobson S. Clonal expansion of human T-cell leukemia virus type I–infected cells in asymptomatic and symptomatic carriers without malignancy. J Virol 1995; 69:2863–8. 7. Igakura T, Stinchcombe JC, Goon PK, et al. Spread of HTLV-I between lymphocytes by virus-induced polarization of the cytoskeleton. Science 2003; 299:1713–6. 8. Mahieux R, Pise-Masison CA, Nicot C, Green P, Hall WW, Brady JN. Inactivation of p53 by HTLV type 1 and HTLV type 2 Tax transactivators. AIDS Res Hum Retroviruses 2000; 16:1677–81. 9. Nagai M, Usuku K, Matsumoto W, et al. Analysis of HTLV-I proviral load in 202 HAM/TSP patients and 243 asymptomatic HTLV-I carriers: high proviral load strongly predisposes to HAM/TSP. J Neurovirol 1998; 4:586–93. 10. Yamano Y, Nagai M, Brennan M, et al. Correlation of human T-cell lymphotropic virus type 1 (HTLV-1) mRNA with proviral DNA load, virus-specific CD8+ T cells, and disease severity in HTLV-1–associated myelopathy (HAM/TSP). Blood 2002; 99:88–94. 11. Osame M. Overview, epidemiology and clinical features of HTLV-I– associated myelopathy (HAM/TSP). Clin Neurol 1988; 28:1375–8. 12. Levin MC, Lee SM, Kalume F, et al. Autoimmunity due to molecular mimicry as a cause of neurological disease. Nat Med 2002; 8:509–13. 13. Jacobson S. Immunopathogenesis of human T cell lymphotropic virus type I–associated neurologic disease. J Infect Dis 2002; 186(Suppl 2): S187–92. 14. Manns A, Miley WJ, Wilks RJ, et al. Quantitative proviral DNA and antibody levels in the natural history of HTLV-I infection. J Infect Dis 1999; 180:1487–93. 15. Tachibana N, Okayama A, Ishihara S, et al. High HTLV-I proviral DNA level associated with abnormal lymphocytes in peripheral blood from asymptomatic carriers. Int J Cancer 1992; 51:593–5. 16. Cimarelli A, Duclos CA, Gessain A, et al. Quantification of HTLV-II proviral copies by competitive polymerase chain reaction in peripheral blood mononuclear cells of Italian injecting drug users, central Africans, and Amerindians. J Acquir Immune Defic Syndr Hum Retrovirol 1995; 10:198–204. 17. Woods TC, Graber JM, Hershow RC, Khabbaz RF, Kaplan JE, Heneine W. Investigation of proviral load in individuals infected with human T-lymphotropic virus type II. AIDS Res Hum Retroviruses 1995; 11: 1235–9. 18. Beilke MA, Japa S, Vinson DG. HTLV-I and HTLV-II virus expression increase with HIV-1 coinfection. J Acquir Immune Defic Syndr Hum Retrovirol 1998; 17:391–7. 19. Zehender G, Meroni L, Varchetta S, et al. Human T-lymphotropic virus type 2 (HTLV-2) provirus in circulating cells of the monocyte/macrophage lineage in patients dually infected with human immunodeficiency virus type 1 and HTLV-2 and having predominantly sensory polyneuropathy. J Virol 1998; 72:7664–8. 20. Murphy EL, Grant RM, Kropp J, Oliveira A, Lee T-H, Busch MP. Increased HTLV-II proviral load following highly active retroviral therapy in HIV-coinfected patients. J Acquir Immune Defic Syndr 2003; 33: 655–6. HTLV-I and -II Provirus Load • JID 2004:190 (1 August) • 509 21. Machuca A, Soriano V. In vivo fluctuation of HTLV-I and HTLV-II proviral load in patients receiving antiretroviral drugs. J Acquir Immune Defic Syndr 2000; 24:189–93. 22. Murphy EL, Watanabe K, Nass CC, Ownby H, Williams A, Nemo G. Evidence among blood donors for a 30-year-old epidemic of human T lymphotropic virus type II infection in the United States. J Infect Dis 1999; 180:1777–83. 23. Murphy EL, Glynn SA, Fridey J, et al. Increased incidence of infectious diseases during prospective follow-up of human T-lymphotropic virus type II– and I–infected blood donors. Retrovirus Epidemiology Donor Study. Arch Intern Med 1999; 159:1485–91. 24. Murphy EL, Wang B, Sacher RA, et al. Respiratory and urinary tract infections, arthritis and asthma associated with HTLV-I and HTLV-II infection. Emerg Infect Dis 2004; 10:109–16. 25. Busch MP, Laycock M, Kleinman SH, et al. Accuracy of supplementary serologic testing for human T-lymphotropic virus types I and II in US blood donors. Retrovirus Epidemiology Donor Study. Blood 1994; 83: 1143–8. 26. Liu H, Leung P, Glynn S, Murphy EL. Human T-lymphotropic virus type II RFLP subtypes a0 and b4/b5 are associated with different demographic and geographic characteristics in the United States. Virology 2001; 279:90–6. 27. Kaplan JE, Khabbaz RF, Murphy EL, et al. Male-to-female transmission of human T-cell lymphotropic virus types I and II: association with viral load. The Retrovirus Epidemiology Donor Study Group. J Acquir Immune Defic Syndr Hum Retrovirol 1996; 12:193–201. 28. Albrecht B, Collins ND, Newbound GC, Ratner L, Lairmore MD. Quantification of human T-cell lymphotropic virus type 1 proviral load by quantitative competitive polymerase chain reaction. J Virol Methods 1998; 75:123–40. 29. Cimarelli A, Duclos CA, Gessain A, Casoli C, Bertazzoni U. Clonal expansion of human T-cell leukemia virus type II in patients with high proviral load. Virology 1996; 223:362–4. 30. Endo K, Hirata A, Iwai K, et al. Human T-cell leukemia virus type 2 (HTLV-2) Tax protein transforms a rat fibroblast cell line but less efficiently than HTLV-1 Tax. J Virol 2002; 76:2648–53. 31. Mahieux R, Pise-Masison CA, Lambert PF, et al. Differences in the ability of human T-cell lymphotropic virus type 1 (HTLV-1) and HTLV2 Tax to inhibit p53 function. J Virol 2000; 74:6866–74. 510 • JID 2004:190 (1 August) • Murphy et al. 32. Lewis MJ, Sheehy N, Salemi M, VanDamme AM, Hall WW. Comparison of CREB- and NF-kB–mediated transactivation by human T lymphotropic virus type II (HTLV-II) and type I (HTLV-I) Tax proteins. Virology 2002; 295:182–9. 33. Ross TM, Minella AC, Fang ZY, Pettiford SM, Green PL. Mutational analysis of human T-cell leukemia virus type 2 Tax. J Virol 1997; 71: 8912–7. 34. Schreiber GB, Murphy EL, Horton JA, et al. Risk factors for human T-cell lymphotropic virus types I and II (HTLV-I and -II) in blood donors: the Retrovirus Epidemiology Donor Study. NHLBI Retrovirus Epidemiology Donor Study. J Acquir Immune Defic Syndr Hum Retrovirol 1997; 14:263–71. 35. Taylor GP, Tosswill JH, Matutes E, et al. Prospective study of HTLVI infection in an initially asymptomatic cohort. J Acquir Immune Defic Syndr 1999; 22:92–100. 36. Etoh K, Yamaguchi K, Tokudome S, et al. Rapid quantification of HTLV-I provirus load: detection of monoclonal proliferation of HTLVI–infected cells among blood donors. Int J Cancer 1999; 81:859–64. 37. Orland JR, Engstrom J, Fridey J, et al. Prevalence and clinical features of HTLV neurologic disease in the HTLV outcomes study. Neurology 2003; 61:1588–94. 38. Kramer A, Maloney EM, Morgan OS, et al. Risk factors and cofactors for human T-cell lymphotropic virus type I (HTLV-I)–associated myelopathy/tropical spastic paraparesis (HAM/TSP) in Jamaica. Am J Epidemiol 1995; 142:1212–20. 39. Wilks R, Hanchard B, Morgan O, et al. Patterns of HTLV-I infection among family members of patients with adult T-cell leukemia/lymphoma and HTLV-I associated myelopathy/tropical spastic paraparesis. Int J Cancer 1996; 65:272–3. 40. Iga M, Okayama A, Stuver S, et al. Genetic evidence of transmission of human T cell lymphotropic virus type 1 between spouses. J Infect Dis 2002; 185:691–5. 41. Moules V, Gabet AS, Nass CC, et al. Endemic versus epidemic viral spreads display distinct patterns of intraindividual HTLV-2 replication (abstract O60). AIDS Res Hum Retroviruses 2003; 19(Suppl):S24. 42. Jeffery KJ, Usuku K, Hall SE, et al. HLA alleles determine human Tlymphotropic virus–I (HTLV-I) proviral load and the risk of HTLVI–associated myelopathy. Proc Natl Acad Sci USA 1999; 96:3848–53.