Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
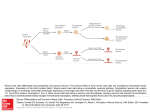
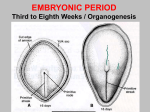
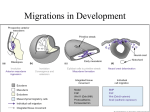
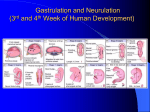
Craniofacial embryology and growth Embryology Week 1 Fertilization Cleavage o Mitotic division o Morula (32 cell) – day 3-4 o Blastocyst as develops fluid filled cavity – day 5 Implantation Week 2 Forms 2 layers o Epiblast (primary ectoderm) o Hypoblast (primary endoderm) Week 3 Gastrulation o Under control of homeobox gene o Cells from epiblast layer develop pseudopodia and migrate between epiblast and hypoblast in the midline forming the primitive streak. (mesoderm) o The migrating cells that ingress through the primitive node migrate caudally to form the prechordal plate and notochordal process 1. Notochordal process induces development of vertebral bodies o Those that ingress through the primitive groove form the mesoderm lying on either side of the midline – condensing into rod-like structures 1. paraxial mesoderm – forms axial skeleton, voluntary muscle, dermis 2. intermediate mesoderm – urinary system 3. lateral plate mesoderm ventral layer – mesothelial covering for organs dorsal area – body lining, majority of dermis, tendons o The hypoblast is replaced by the migrating epiblast = this forms the definitive endoderm o Thus the trilaminar germ disc are all derived from the epiblast Paraxial mesoderm o Cells form rounded whorl like structures – somitomeres o Over next few days, become organized into discrete blocks – somites o The first seven pairs of somitomeres do not go on to form somites o The first 4 pairs of somites contribute to development of: 1. basi-occipital bone 2. tongue muscles Origins of craniofacial muscles: Mesodermal Muscles Innervation Origin Somitomeres 1, 2 Superior, medial and ventral recti CN III Somitomere 3 Somitomere 4 Somitomere 5 Somitomere 6 Somitomere 7 Somites 1, 2 Somites 2-5 Superior oblique Muscles of mastication Lateral rectus 2nd arch muscles Stylopharyngeus Intrinsic laryngeals Tongue muscles CN IV CN V CN VI CN VII CN IX CN X CN XII Week 4 Somites separates into 3 components 1. sclerotome develops into vertebrae abnormal development leads to spina bifida 2. myotome 3. dermatome Neurulation o Folding of the neural plate into neural tube o PAX6, Sonic Hedge-Hog (SHH), and FGF signaling are involved with neurulation o Neural crest cells from the lateral margins of the folding neural tube detach and migrate o timing and extent of neural cell migration and differentiation is dependent on a complex patterning of inductive homeobox gene (HOX, MSX) signaling between the neural crest and adjacent neural tube, lateral plate mesoderm, and epidermis o All of the skeletal and connective tissue components of the face (except enamel) – dentin, cartilage, bone dermis, smooth muscle, subcutaneous fat and connective tissue surrounding blood vessels, glands, muscle are neural crest derived o Skull bone superior to the sella turcica are neural crest derived o Problems in neurulation may result in midline neurologic and craniofacial malformations such as holoprosencephaly (single cavity forebrain), cycloplegias, neural tube defects, and midline orofacial clefts o Deficiencies in neural crest tissue migration or proliferation produces a varied and extensive group of craniofacial malformations referred to as neurocristopathies, which include von Recklingshausen neurofibromatosis, hemifacial microsomia, orofacial clefts, and DiGeorge and Treacher Collin syndromes Facial development A series of inductive events between the prosencephalon, mesencephalon, and rhombencephalon and the neural crest tissue that migrates into the craniofacial complex and pharyngeal arch apparatus helps to form the five facial prominences (the frontonasal and the bilateral maxillary and mandibular prominences) Groove between lateral nasal process and median nasal process forms nasolacrimal duct In the region rostral to the somites, neural crest emigrate as 3 distinct populations (J Anatomy Nov 2005) 1. trigeminal crest – migrates to the frontonasal and first branchial arch a. contributes to the neural crest component of trigeminal ganglion 2. hyoid crest – migrates to the second branchial arch 3. vagal crest – migrates to the third and subsequent arches and also extensively within the trunk The two migrating populations (trigeminal and hyoid) do not mix – suggesting the deployment of an inhibiting mechanism The trigeminal neural crest cells also maintain separation from the adjacent cranial mesenchyme cells. The crest cells migrate immediately under the surface ectoderm, forming a pathway between ectoderm and mesodermal mesenchyme Craniofacial growth Overview of facial growth Maxilla lengthens in a posterior direction at the maxillary tuberosity Posterior lengthening rotates the maxilla anteriorly and inferiorly Simultaneously posterior lengthening of the condyle and ramus displaces the mandible anteriorly Growth of the middle cranial fossa secondarily displaces the maxilla and the mandible forwards. Theories of craniofacial growth Herring describes three theories of cranial facial epigenesis. 1. The first theory embraces the notion that the initial form of the skull is genetically determined, but that when function begins(after birth or hatching), epigenetic regulation takes over. Emphasis here is on the onset of function as the marker for the start of epigenetic regulation. 2. The second theory considers cartilage as the pacemaker for skeletal growth. Here, the form of facial cranial cartilages is genetically dictated, whereas the form of bones is epigenetically regulated by the cartilage. This theory was forwarded by Scott, who thought that the cartilage of the cranial base, nasal capsule and Meckel's cartilage act as pace-makers for the early growth of the facial skeleton. 3. The third theory of skull growth, proposed by Moss, is the functional matrix hypothesis. In Moss' view, overall growth and development of the head is regulated by the development of its soft, nonskeletal parts, with skull growth being completely secondary to the prior development and constraints of its enveloping soft tissues. The hypothesis is rooted in an approach to anatomy in which the head and neck are conceived as performing a set of functions, such as vision, hearing, or digestion A functional matrix is the set of all soft tissues, i.e., cells, tissues, organs, and air volumes that carry out a specific function. For each soft-tissue matrix, a skeletal unit composed of hard tissues exists, i.e., bone, cartilage, and dense connective tissue, which protects and supports the matrix The most fundamental dictum of the hypothesis is succinctly stated by Moss as bones do not grow, they are grown (within functional matrices). Cranium Vertebral skull is formed from 2 tissues 1. neural crest - Only the trigeminal population contributes to the skull 2. mesoderm cranium is made up of 1. neurocranium - which includes the chondrocranium of the skull base and the membranous bone of the calvarium 2. viscerocranium that forms the membranous bones of the face. The various areas of the craniomaxillofacial skeleton grow by very different methods. Neurocranium a. The cranial vault sutures are skeletal joints of the syndesmosis type b. The sagital, metopic and lambdoid are formed by narrowing of membranous gaps between bones that are initially widely separate. They overlie areas in which brain tissue does not lie close to the surface c. The coronal suture is different and the parietal bone can be seen to overlap the frontal bone from the outset – this is a flexible/sliding joint. d. Its base is formed by endochondral ossification and the joints are of the synchondrosis type. The cartilaginous precursors form around the preexisting cranial nerves and blood vessels. Thus the foramina around the great vessels occur within the endochondral bones of the skull base e. Thus endocondral ossification in the cranium exists in the petrous and mastoid process of temporal bone, occipital, ethmoid, sphenoid and Meckel’s part of the mandible Viscerocranium a. zygomatic, maxillary, and palatine i. overlapping or sliding joints where the direction of bone growth tends to parallel the plane of the suture. ii. This arrangement provides for adaptive adjustments to pressure in utero and early infancy. Growth of cranial vault The sutures are growth sites where cells undergo proliferation and differentiation into osteoblasts. The interlocking peg-and-socket arrangement allows osteogenesis to occur mainly at the bottom of the socket and point of the peg (suture front) for simultaneous jointing and growth of the bone against the suture. The sutures produce new bone in response to the expanding neurocranium The dura contains osteoprogenitor cells which is not present in the periosteum layer. In very young animals, if skull is excised but dura left behind, the dura has the ability to regenerate the cranium and its sutures. Maxilla Growth Horizontal growth Horizontal lengthening of the maxillary arch is produced by remodeling at the maxillary tuberosity (deposition site) – a major (but not only) growth site Deposition occurs in 3 directions – posteriorly, laterally and inferiorly. The endosteal surface is resorptive and contributes to the formation of the maxillary sinus. Vertical growth Nasal septum theory Maxilla remodels in a posterosuperior manner becoming displaced in an opposite anteriorinferior direction Expansion of cartilage in the nasal septum exerts an anterior and inferior pull at the septomaxillary ligament. This sets up tension in all maxillary sutures – the bones secondarily enlarge at their sutures in response to the tension created Most sutures in the facial complex do not simply grow in perpendicular plane to suture (as in calvarial sutures) – sutures of maxilla, lacrimal, zygomatic, nasal and ethmoidal bones also undergo slide Zygoma growth mirrors maxilla – malar deposition laterally and posteriorly, rotating nose anterior-inferiorly Moss functional matrix Soft tissue parts and their growth and functioning orchestrate the remodeling pattern Palatal remodeling Lining surfaces of the bony walls and floor of the nasal chambers are resorptive. Produces a lateral and anterior expansion of the nasal chambers and a downward relocation of the palate The oral side of the bony palate is depository, The external side of the anterior part of the maxillary arch is resorptive, with bone being added onto the inside of the arch – this increases arch width, widening the palate. Mandibular growth Largely membranous ossification but has endochodral component with Meckel’s cartilage) Principle growth vectors are posterior and superior Ramus remodeling is important as it positions the lower arch in occlusion with the upper The body principally undergoes anterior-inferior displacement Ramus growth Lingual tuberosity is the anatomic equivalent of maxillary tuberosity – a major growth site Deposition occurs on its posterior facing surface Coronoid process grows superiorly and posteriorly Soft tissue parts and their growth and functioning orchestrate the remodeling pattern (Moss functional matrix) Single field of surface resorption is present at the inferior edge of the mandible at the body-ramus junction – this forms the antegonial notch Condylar growth A secondary growth center (once thought to be a pacesetting master center) – it is not a primary determinant of mandibular growth Grows superiorly and posteriorly following the growth of the ramus but not leading it Condylar growth is primarily mediated by traction from surrounding soft tissues (muscles of mastication,tongue)