Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
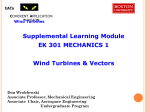
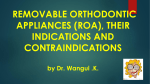
432 JACC Vol. 32, No. 2 August 1998:432–7 Three-Dimensional Echocardiographic Planimetry of Maximal Regurgitant Orifice Area in Myxomatous Mitral Regurgitation: Intraoperative Comparison With Proximal Flow Convergence CHRISTIAN S. BREBURDA, MD,* BRIAN P. GRIFFIN, MD, FACC, MIN PU, MD, LEONARDO RODRIGUEZ, MD, DELOS M. COSGROVE, III, MD, JAMES D. THOMAS, MD, FACC Cleveland, Ohio Objectives. We sought to validate direct planimetry of mitral regurgitant orifice area from three-dimensional echocardiographic reconstructions. Background. Regurgitant orifice area (ROA) is an important measure of the severity of mitral regurgitation (MR) that up to now has been calculated from hemodynamic data rather than measured directly. We hypothesized that improved spatial resolution of the mitral valve (MV) with three-dimensional (3D) echo might allow accurate planimetry of ROA. Methods. We reconstructed the MV using 3D echo with 3° rotational acquisitions (TomTec) using a transesophageal (TEE) multiplane probe in 15 patients undergoing MV repair (age 59 6 11 years). One observer reconstructed the prolapsing mitral leaflet in a left atrial plane parallel to the ROA and planimetered the two-dimensional (2D) projection of the maximal ROA. A second observer, blinded to the results of the first, calculated maximal ROA using the proximal convergence method defined as maximal flow rate (2pr2va, where r is the radius of a color alias contour with velocity va) divided by regurgitant peak velocity (obtained by continuous wave [CW] Doppler) and corrected as necessary for proximal flow constraint. Results. Maximal ROA was 0.79 6 0.39 (mean 6 SD) cm2 by 3D and 0.86 6 0.42 cm2 by proximal convergence (p 5 NS). Maximal ROA by 3D echo (y) was highly correlated with the corresponding flow measurement (x) (y 5 0.87x 1 0.03, r 5 0.95, p < 0.001) with close agreement seen (DROA (y 2 x) 5 0.07 6 0.12 cm2). Conclusions. 3D echo imaging of the MV allows direct visualization and planimetry of the ROA in patients with severe MR with good agreement to flow-based proximal convergence measurements. (J Am Coll Cardiol 1998;32:432–7) ©1998 by the American College of Cardiology The mitral valve (MV) apparatus has a complex threedimensional (3D) structure, especially in the presence of myxomatous degeneration with leaflet prolapse or flail. Although excellent images of the MV are obtainable by twodimensional (2D) echocardiography (1), a full appreciation of the 3D morphology is often lacking. The regurgitant orifice area (ROA) is a fundamental measure of valvular incompetence, which may be used to follow the regurgitant severity over time. ROA may be measured using Doppler echocardiographic examination of the proximal convergence zone (2), the difference in flow across regurgitant and nonregurgitant valves (3), and direct measurement of the jet vena contracta (4), but these techniques are time consuming, technically demanding, and affected by the geometry of the regurgitant flow field and by machine factors, limiting utilization in the clinical setting. Ideally, ROA would be measured directly similar to the orifice area of stenotic valves, but 2D echocardiographic definition of ROA is difficult because of the complex geometry involved. This is unfortunate because an integrated assessment of mitral morphology and regurgitant severity is used in deciding the repairability of the MV and the appropriate timing of surgery (5–7). Three-dimensional echocardiography is an evolving technology (8) that can improve on 2D echo in the depiction of MV pathology (9,10). We have recently used intraoperative 3D reconstruction of the MV to better characterize the location and extent of leaflet prolapse (11), suggesting that the improved spatial orientation and resolution of 3D echo would allow direct planimetry of ROA. The purposes of this study therefore were: (1) to quantify the ‘anatomical’ size of the maximal ROA by 3D echo, comparing the size with that measured by Doppler techniques; and (2) to determine whether the area and volume of prolapsing tissue measured by 3D echo correlates with the severity of mitral regurgitation. From the Cardiovascular Imaging Center, Department of Cardiology, The Cleveland Clinic Foundation, Cleveland, Ohio. This report was presented in part at the 69th Annual Meeting of the American Heart Association, November 1996, New Orleans, Louisiana. Dr. Thomas was supported in part by Grant NCC 9-60, from the National Aeronautics and Space Administration, Houston, Texas and Grant 1R01HL56688, National Heart Lung and Blood Institute, Bethesda, Maryland. Manuscript received December 11, 1997; revised manuscript received March 19, 1998, accepted April 17, 1998. *Present address: The Thoraxcentre, Rotterdam, The Netherlands. Address for correspondence: Dr. James D. Thomas, Department of Cardiology/F-15, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, Ohio 44195. E-mail: [email protected]. ©1998 by the American College of Cardiology Published by Elsevier Science Inc. 0735-1097/98/$19.00 PII S0735-1097(98)00239-3 JACC Vol. 32, No. 2 August 1998:432–7 BREBURDA ET AL. QUANTIFICATION OF MITRAL REGURGITATION BY THREE-DIMENSIONAL ECHO Abbreviations and Acronyms 2D 5 Two-dimensional 3D 5 Three-dimensional CW 5 Continuous wave MR 5 Mitral regurgitation MV 5 Mitral valve ROA 5 Regurgitant orifice area RSV 5 Regurgitant stroke volume TEE 5 Transesophageal echocardiography Methods Patient selection. We studied 15 patients (32–75 years, mean 59 6 11 years, nine men and six women) with myxomatous MV prolapse or leaflet flail with severe mitral regurgitation (MR) undergoing MV repair. The patients were selected at random based on the logistics of the intraoperative echocardiography schedule, with typically one patient per day being studied. Patients were not excluded on the basis of image quality, although patients in atrial fibrillation were excluded because of difficulties in 3D reconstruction. All patients underwent a preoperative transthoracic echo and an intraoperative transesophageal echocardiography (TEE) pre- and postcardiac bypass. The prebypass intraoperative exam preceded the 3D acquisition and was recorded on 0.5 in. VHS video tape by an experienced independent clinician with complete interrogation of the MV apparatus. Three-dimensional echocardiography and reconstruction. Three-dimensional TEE was performed in conjunction with the preoperative exam, utilizing a 5-MHz phased-array multiplane probe (12), interfaced with a Hewlett-Packard Sonos 1500 (77035A) or 2500 (M2406A) (Andover, MA), equipped with investigational 3D acquisition software. Electrocardiographic gating was obtained from the Hewlett-Packard system leads using a preset RR interval to reject data from all heart cycles .100 ms above or below this limit. Images were acquired only at expiration using input from a nasal thermistor placed in the endotracheal tube. After completing the clinical study, the probe was positioned in the midesophagus, with the central axis placed at the leaflet coaptation point around which the image plane was rotated to encompass the whole MV apparatus. A TomTec Echo Scan (3.0, TomTec Imaging Systems, Inc., Boulder, CO) was interfaced with the HewlettPackard system via the composite video output port. Data were stored on videotape and digitally on the TomTec hard disk with later transfer to 650 MB magneto-optical discs. Conical data sets consisted of 60 sequential cross sections acquired at 3° increments for a complete heart cycle (20 to 25 frames) (13). Data were processed off-line by the TomTec analysis program, synchronizing the cross sections with the phase of the cardiac cycle, converting from polar to Cartesian coordinates, and interpolating to fill gaps between the sequential cross sections. The images were displayed in a dynamic 2D format, allowing arbitrarily oriented planes to be viewed independently of the original ultrasonic window. From a selected cut plane, up to 433 eight parallel planes were computed at predetermined intervals and displayed in motion for quantitative volumetric analysis. Three-dimensional surface rendering was also performed using border-detection algorithms based on ultrasonic intensity (threshold) and rate of change along the line of sight (gradient), optimized to differentiate cardiac structures from the blood pool, background and noise artifacts; a distance and gradient shading algorithm was applied to enhance the perception of depth. Measurements. Two-dimensional slices from the 3D data set were displayed similar to conventional transesophageal orientations (14). The surgical view from the left atrium facing the mitral annulus was reconstructed using surface rendering, and the location of prolapse was evaluated under direct 3D visualization. Three-dimensional echocardiography. The volume of prolapse was calculated using the short axis view of the mitral annulus as a reference image for multiple parallel 2 chamber long axis views to be reconstructed orthogonal to the mitral annulus from the medial to the lateral commissural point. Multiple, 1-mm-thick equidistant cut planes were displayed, covering the total extent of the prolapse from its maximal area to the edges. The anterior and posterior leaflet hinge points were connected with a line to define the annular plane as described previously (1), and the area of the first parallel plane was highlighted and copied as a label to the next 1-mm slice, allowing a consistent determination of the annular plane in all analyzed cut planes. The 2D area of prolapse between the leaflet and the annular plane was then traced manually in each long axis view and the volume of prolapse calculated as the sum of each traced area multiplied by the slice thickness: O L V5 ADx, M where V 5 volume of prolapse, L 5 lateral, M 5 medial, A 5 area, and Dx 5 multiple 1-mm-thick (planes). The area of prolapse was planimetered in the volume-rendered 3D reconstruction of the MV from a view plane parallel to the mitral annulus in the left atrium facing the mitral annulus just above the maximal extent of prolapse. The maximal area of the regurgitant orifice was visualized from a cut plane parallel to the gap between the prolapsing leaflet and orthogonal to the annular plane in the standard 2D echo long axis view. Thus, the 3D reconstruction imaged the orifice in its maximal extent as viewed from the left atrium above the mitral annulus. The image was then transferred to the Hewlett-Packard system and recalibrated using the 5-cm reference scale on the 3D image. The maximal orifice opening was then traced manually. Proximal convergence method. The proximal convergence field was optimized by baseline shifting the color Doppler aliasing velocity to between 34 and 69 cm/s or ;10% to 15% of peak mitral velocity. The radial distance (r) between the first aliasing contour (red/blue interface) and the center of the regurgitant orifice was measured at the time of the largest 434 BREBURDA ET AL. QUANTIFICATION OF MITRAL REGURGITATION BY THREE-DIMENSIONAL ECHO convergence image. For patients with nonflail mitral leaflets, the orifice was assumed to be at the plane passing through the tips of the mitral leaflets; for flail mitral leaflets, the orifice was assumed to lie in the plane of the nonflail leaflet. Maximal instantaneous regurgitant flow (Qmax) was calculated as Qmax 5 2pr2va, where r is the maximal distance to the contour of velocity va, with a hemispheric contour assumed. The regurgitant orifice area was obtained by dividing maximal flow by the peak regurgitant velocity (vp) obtained by continuous-wave (CW) Doppler: ROA 5 Qmax/vp. Regurgitant stroke volume (RSV) was obtained by multiplying ROA by the velocity–time integral of CW regurgitant velocity (VTICW): ROA 3 VTICW or 2pr2va 3 VTICW/vp. If the proximal flow field was distorted by wall contact in any transesophageal plane, the geometric convergence angle (a) was determined and corrected. ROA (cROA) and RSV (cRSV) were calculated as cROA 5 ROA 3 a/180 and cRSV 5 RSV 3 a/180 as validated previously (15). Statistical analysis. All values are expressed as mean 6 SE. For the validation of 3D echo, planimetered ROA was compared with proximal convergence ROA by linear regression and analysis of agreement to give the bias and scatter in the measurements. Doppler RSV and ROA as well as the 3D estimate of the severity of prolapse by prolapse area and volume were compared with 3D ROA using linear regression. Interobserver and intraobserver variability. In 10 patients selected randomly, the proximal flow convergence and 3D echo planimetry were obtained independently by two observers. Intraobserver variability was also calculated by repeating measurements 1 month after the initial measurement. Results Table 1 lists the demographic and clinical characteristics of the patients. Salient features include male dominance (60%) and relative lack of symptomatology. Imaging of the regurgitant orifice. Under optimal conditions, the 3D ROA quantification took ;15 min to complete, with 3 to 4 min for image acquisition, 8 to 10 min for processing and reconstruction of the image, and 2 to 3 min for recalibration and planimetry of the ROA. In three patients, electrocautery from adjacent surgical suites interfered with image quality and slowed acquisition, but the regurgitant orifice could be successfully reconstructed in all patients. Figure 1 shows a 3D echo reconstruction of the MV at the level of the mitral annulus. The regurgitant orifice is viewed with a posterior projection from a position in the anterior left atrium, showing deep prolapse and partial flail of the middle scallop of the posterior mitral leaflet. Figure 2 shows an example of an eccentric proximal flow convergence zone with wall constraint. Echocardiographic findings. Table 2 summarizes the findings from the clinical intraoperative echo studies. Cases were divided approximately equally between leaflet flail and pure prolapse, with the expected posterior leaflet predominance. JACC Vol. 32, No. 2 August 1998:432–7 Table 1. Demographic and Clinical Data of the Patient Population Continuous Variables Mean 6 SD (Minimum and Maximum) Age (years) Height (cm) Weight (kg) Systolic BP (mm Hg) Diastolic BP (mm Hg) Heart rate (beats/min) Onset of murmur (years) Ejection fraction (%) 59.1 6 11.2 172.8 6 10.2 75.9 6 14.2 125 6 13 71 6 11 84 6 7 9.4 6 17.2 59 6 8 (32–75) (157–189) (53.7–109) (104 –148) (50 – 86) (76 –100) (0 – 60) (40 –70) Categorical Variables n % Gender Hypertension Coronary artery disease Congestive heart failure CHF class I CHF class II CHF class III Dyspnea Palpitations Chest pain 9 men 5 3 3 8 4 3 5 4 3 60 33 20 20 53 27 20 33 27 20 (BP) blood pressure; (CHF) congestive heart failure (grading based on New York Heart Association). The left ventricular ejection fraction was normal in most cases, although it ranged as low as 40%. Measurements of the regurgitant orifice area. The proximal convergence zone was well visualized in all cases. Because of the preponderance of posterior prolapse and flail pathology, all but one of these zones were constrained by the adjacent posterior wall, requiring correction of the ROA by the constraining angle a. Maximal ROA by 3D echo (y) was 0.79 6 0.39 cm2 (mean and SD, range 0.37 to 1.97 cm2) and 0.86 6 0.42 cm2 (range 0.31 to 1.63 cm2) by proximal convergence (x). Regression analysis demonstrated excellent correlation and Figure 1. Three-dimensional visualization of a flail posterior leaflet. The vantage is of an observer on the anterior mitral annulus looking posterior toward the posterior mitral leaflets, which is flail in its middle scallop. LA 5 left atrium; LV 5 left ventricle; PL 5 posterior leaflet. Medial and Lateral 5 respective mitral commissures. JACC Vol. 32, No. 2 August 1998:432–7 BREBURDA ET AL. QUANTIFICATION OF MITRAL REGURGITATION BY THREE-DIMENSIONAL ECHO 435 Figure 2. Flail posterior leaflet (transesophageal view) demonstrating proximal flow convergence with wall constraint because of the proximetry of the posterior wall. To adjust for the predictable overestimation due to this geometric distortion, regurgitant flow rate and orifica area are adjusted by a/180. LA 5 left atrium; LV 5 left ventricle. agreement: y 5 0.87x 1 0.03, r 5 0.95, p , 0.001, DROA (y 2 x) 5 20.07 6 0.13 cm2 (mean 6 SD), with a range of 20.31 to 0.14 cm2 (Fig. 3). Figure 4 shows the difference between ROA planimetered by 3D echo and calculated by proximal convergence plotted against the mean of these measurements. Correlation of ROA with area and volume of prolapse. The area (x) and volume (y) of prolapse, each quantified by 3D echo, were closely correlated with r 5 0.79, p , 0.001, y 5 0.91x 1 0.39. Three-dimensional area of prolapse correlated slightly better with the 3D ROA (r 5 0.58, p , 0.04) than with calculated ROA by proximal convergence (r 5 0.43, p 5 NS), although wide scatter was seen in the relationship. Threedimensional prolapse volume correlated neither with 3D nor flow ROA (see Table 3). Reproducibility. The intraobserver and intraobserver variability averaged 1.1 6 11% (mean difference 6 SD) for radius measurement, 6.7 6 11% (mean difference 6 SD) for convergence angle measurement and 1 6 10% (mean difference 6 SD) for 3D ROA planimetry, 1.3 6 12% for area and 1.2 6 8% volume of 3D mitral valve prolapse. Discussion This study demonstrates that MV ROA planimetry is feasible with 3D echocardiography even in patients with severely Table 2. Two-Dimensional Echocardiographic Findings Findings n % Flail posterior leaflet Pure prolapse Posterior involvement Bileaflet involvement Moderately severe MR Severe MR Ejection fraction (%) 8 7 12 3 1 14 59 6 8 53 47 80 20 7 93 (40 –70) distorted valvular geometries resulting from leaflet flail. ROA measured by 3D echo correlated well with that calculated by the proximal convergence method. Quantification of mitral regurgitation. Despite the importance of accurate quantitation of mitral regurgitation (MR) for surgical timing and assessing medical therapy, semiquantitative methods such as contrast ventriculography (15) and visual assessment of color Doppler regurgitant jet size (17) and morphology (18) within the left atrium are mostly used to characterize MR in the routine clinical setting. Although quantitative angiography (19) and 2D Doppler methods (20) are well validated and considered reference standards, they are technically demanding and not used routinely. Semiquantitative methods are easy to use but grade regurgitant severity on a simple linear scale from 1 to 4. Extremes of regurgitant severity are easily differentiated, but the classification of moderate lesions is difficult, especially because these tech- Figure 3. Regression analysis relating effective ROA calculated by flow convergence and planimetered regurgitant orifice area by 3D echocardiography. (r 5 0.95; p , 0.001; y 5 0.87x 1 0.03; standard error of estimate (SEE) 5 0.125.) 436 BREBURDA ET AL. QUANTIFICATION OF MITRAL REGURGITATION BY THREE-DIMENSIONAL ECHO Figure 4. Difference in ROA estimation by 3D echo and proximal convergence plotted against mean ROA by the two techniques. niques are influenced by technical factors and loading conditions. Convergence method. The proximal convergence method has been proposed as a simple quantitative method, requiring only a single acoustic window. Regurgitant flow is measured directly and can be combined with CW Doppler estimate of peak regurgitant velocity to predict ROA. It is generally based on an assumed hemispherical contour shape (2), although prior experimental studies have shown this to be incorrect near the regurgitant orifice (21) or when the proximal flow is constrained by surrounding structures (15,22). Although formulae have been proposed to overcome the overestimation because of proximal constraint (15); in practice only onedimensional corrections have been applied (as in this study), rather than the more valid 3D adjustment (23). This and other technical difficulties in performing the proximal convergence method have limited its use in practice. Three-dimensional echo planimetry. Planimetry is an established method for stenotic orifices, especially in mitral stenosis (24). More recently, multiplane TEE has allowed direct planimetry of the stenotic aortic valve (25). Planimetry is thus potentially a method to measure ROA as a flow-independent measure of regurgitant severity, but 2D echo can only occasionally define the area of malcoaptation and ROA, typically in cases of incomplete MV closure due to severe left ventricular dilatation (26). In myxomatous MV disease, however, the Table 3. Correlations among Three-Dimensional Area of Prolapse, 3D Volume of Prolapse Compared to ROA by Convergence Method, and 3D Echo Planimetry Parameter Parameter r p Value 3D area 3D area 3D volume 3D volume 3D volume 3D ROA ROAPC 3D ROA ROAPC 3D area 0.58 0.43 0.25 0.14 0.79 , 0.04 NS NS NS , 0.001 ROAPC 5 calculated regurgitant orifice area using the proximal flow convergence method; area 5 prolapse area; volume 5 prolapse volume. JACC Vol. 32, No. 2 August 1998:432–7 ROA occurs in planes not readily imaged by conventional 2D imaging, necessitating 3D imaging. Several approaches have been described for 3D echo, not all of them applicable to planimetry of the ROA. Levine and coworkers have used acoustic and electromagnetic localizing devices to position randomly acquired 2D echo planes in 3D space (8). Manual segmentation is required to identify endocardial borders and other structures from which volumes and areas may be calculated. Although good accuracy has been reported for LV volume (27–30) and ventricular septal defect size (31), the inhomogeneous sampling of this technique would make characterization of the mitral regurgitant orifice difficult. In contrast, the TomTec device adopts a structured data acquisition strategy from a single echocardiographic window to yield a nearly isotropic data set. Such a structured approach can be a linear or fan-like sweep or a rotational acquisition from either the transthoracic or (as done here) TEE approach, which is especially effective for reconstructing the MV, as it is in the near field of the TEE probe, allowing it to be densely sampled by the rotating 3D plane. At a 5-cm depth, the edges of successive 3° sector scans are ,2 mm apart, becoming progressively closer as one moves toward the center of the imaging field (where the ROA usually fell). A potential problem is the misregistration of planes when patient or probe movement occurs during the acquisition, a problem exacerbated when arrhythmia or artifact from electrocautery prolongs the acquisition. Finally, an instrument that performs 3D echo in real time has recently been developed (31). Using 16:1 parallel processing and a 2D-phased array crystal, it is capable of generating 3D data sets consisting of 64 scan lines and 64 scan planes at 20 to 40 Hz. Although very promising—and likely the long-term approach to 3D echo—this device cannot yet be used with TEE, and the resolution from the chest wall is likely to be inferior (pending technical improvements) to the approach used in this study. Limitations. We demonstrated that the MV ROA may be imaged and measured by 3D echocardiography, even in patients with distorted MV geometry. One limitation is the lack of a true reference standard for regurgitant severity, especially as the 3D and Doppler methods used in this study measured slightly different entities. Three-dimensional planimetry defines the anatomical ROA, whereas the proximal convergence method should yield the narrowest flow stream (vena contracta), which is smaller than the anatomic orifice by the coefficient of contraction (generally 0.8 to 0.9). Thus, it may be surprising that planimetered areas were slightly smaller than the flow areas. Although this likely relates in large part to measurement noise in both data sets, there may be some systematic overestimation of the flow areas because of incomplete adjustment for flow constraint. The previously validated one-dimensional angle adjustment corrects ;80% of the overestimation; in the future, 3D echo may be used to more fully correct for this complex geometric constraint. Another potential source of error is that 3D ROA was based on a planar projection of the largest apparent orifice but might have JACC Vol. 32, No. 2 August 1998:432–7 BREBURDA ET AL. QUANTIFICATION OF MITRAL REGURGITATION BY THREE-DIMENSIONAL ECHO missed additional areas in other planes. Additionally it is possible that ROA may be underestimated (if beam width artifact thickens the mitral leaflets) or overestimated (if the thin mitral leaflets are not captured in the surfacing algorithm, resulting in drop-out). Artifact from electrocautery is a major problem, sometimes seen even from an adjacent operating room. Atrial fibrillation can significantly prolong 3D reconstruction (although no patients in the current study were in this rhythm) but may be less important with real-time 3D imaging. These results should thus only be considered applicable to patients in sinus rhythm. To minimize the effects of dynamic changes in ROA between the two techniques (33,34), we compared maximal rather than mean values. Conclusions. In this study we have demonstrated that it is feasible to perform quantitative 3D echocardiography for measurement of the mitral ROA in the intraoperative setting. We further showed that 3D ROA agrees closely with that derived by the flow-based proximal convergence method. As 3D acquisition and analysis become faster, quantitative applications such as this should become more common. We thank Sheila Wallace for assistance with the manuscript and Paula Shalling for assistance with the illustrations. References 1. Nishigami K, Yoshikawa J, Yoshida K, et al. Reliability of biplane transesophageal color Doppler echocardiography in evaluating mitral valve prolapse: comparison with surgical findings. J Am Coll Cardiol 1993;2: 263– 8. 2. Vandervoort PM, Rivera JM, Mele D, et al. Application of color Doppler flow mapping to calculate effective regurgitant orifice area: an in vitro study with initial clinical observations. Circulation 1993;88:1150 – 6. 3. Sarano ME, Seward JB, Bailey KR, Tajik AJ. Effective regurgitant orifice area: a noninvasive Doppler development of an old hemodynamic concept. J Am Coll Cardiol 1994;23:443–51. 4. Hall SA, Brickner ME, Willett DL, Irani WN, Afridi I, Grayburn PA. Assessment of mitral regurgitant severity by Doppler color flow mapping of the vena contracta. Circulation 1997;95:636 – 42. 5. Perier P, Clausnitzer B, Mistarz K. Carpentier “sliding leaflet” technique for repair of the mitral valve: early results. Ann Thoracic Surg 1994;57:383– 6. 6. Cosgrove DM III, Arcidi JM, Rodriguez L, Stewart JS, Powell K, Thomas JD. Initial experience with the Cosgrove-Edwards annuloplasty system. Ann Thorac Surg 1995;60:499 –504. 7. Schiller NB, Foster E, Redberg RF. Transesophageal echocardiography in the evaluation of mitral regurgitation. The twenty four signs of severe mitral regurgitation. Cardiol Clin 1993;11:399 – 408. 8. Levine RA, Weyman AE, Handschumacher MD. Three-dimensional echocardiography: techniques and applications. Am J Cardiol 1989;69:121H–130H. 9. Cheng TO, Wang XF, Zheng LH, Li ZA, Lu P. Three-dimensional transesophageal echocardiography in the diagnosis of mitral valve prolapse. Am Heart J 1994;129:1218 –24. 10. Roelandt JRTC, Ten Cate FJ, Vletter WB, Taams MA. Ultrasonic dynamic three-dimensional visualization of the heart with a multiplane transesophageal imaging transducer. J Am Soc Echocardiogr 1994;7:217–29. 11. Breburda CS, Kondo H, Griffin BP, Cosgrove DM III, Thomas JD. Intraooperative three dimensional transesophageal echocardiography in mitral valve repair of mitral valve prolapse: comparison to quadrilateral tissue resection (abstr). J Am Soc Echocardiogr 1996;9:368. 12. Flachskampf FA, Hoffman R, Verlande M, Schneider W, Ameling W, Hanrath P. Initial experience with a multiplane transesophageal echotransducer: assessment of diagnostic potential. Eur Heart J 1992;13:1201– 6. 13. Magni G, Hijazi ZM, Pandian NG, et al. Two- and three-dimensional 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 437 transesophageal echocardiography in patient selection and assessment of atrial septal defect closure by the new DAS-Angel Wings device. Circulation 1997;96:1722– 8. Pandian NG, Nanda NC, Schwartz SL, et al. Three-dimensional transesophageal echocardiographic imaging of the heart and aorta in humans using a computed tomographic imaging probe. Echocardiography 1992;9:677– 87. Pu M, Vandervoort PM, Griffin BP, et al. Quantification of mitral regurgitation by the proximal convergence method using transesophageal echocardiography. Clinical validation of a geometric correction for the proximal flow constraint. Circulation 1995;92:2169 –77. Sellers RD, Levy MJ, Amplatz K, Lillehei CW. Left retrograde cardioangiography in acquired cardiac diseases: technique, indications and interpretations in 700 cases. Am J Cardiol 1964;14:437– 47. Miyatake K, Okamoto M, Kinoshita N, et al. Semiquantitative grading of the severity of mitral regurgitation by real-time two-dimensional Doppler flow imaging technique. J Am Coll Cardiol 1986;7:82– 8. Spain MG, Smith MD, Grayburn PA, Harlament EA, DeMaria AN. Quantificative assessment of mitral regurgitation by Doppler color flow imaging: angiographic and hemodynamic correlations. J Am Coll Cardiol 1989;13:585–90. Croft CH, Lipscomb K, Mathis K, et al. Limitation of qualitative angiographic grading in aortic or mitral regurgitation. Am J Cardiol 1984;53:1593–8. Ascah KJ, Stewart WJ, Jiang L, et al. A Doppler two dimensional echocardiographic method for quantification of mitral regurgitation. Circulation 1985;72:377– 83. Rodriguez L, Anconina J, Flachskampf FA, Weyman AE, Levine RA, Thomas JD. Impact of finite orifice size on proximal flow convergence: implications for Doppler quantification of valvular regurgitation. Circ Res 1992;70:923–30. Chen C, Koschyk D, Brockhoff C, et al. Noninvasive estimation of regurgitant flow rate and volumes in patients with mitral regurgitation by Doppler color mapping of the accelerating flow field. J Am Coll Cardiol 1993;21:374–83. Cape EG, Thomas JD, Weyman AE, Yoganathan AP, Levine RA. Three dimensional orifice correction is required for calculation flow rate by proximal isovelocity surface area technique. J Am Soc Echocardiogr 1995; 8:585–94. Henry WL, Griffith JM, Michaelis LL, McIntosh CL, Morrow AG, Epstein SE. Measurement of mitral orifice area in patients with mitral valve disease by real-time, two-dimensional echocardiography. Circulation 1975;51:827–31. Hoffmann R, Flachskampf FA, Hanrath P. Planimetry of orifice area in aortic stenosis using multiplane transesophageal echocardiography. J Am Coll Cardiol 1993;22:529 –34. Izumi S, Miyatake K, Beppu S, et al. The gap between mitral leaflets as the cause of mitral regurgitation: relationship to mitral valve prolapse. Int Med 1992;31:28 –32. Siu SC, Rivera JM, Guerrero JL, et al. Three-dimensional echocardiography. In vivo validation for left ventricular volume and function. Circulation 1993;88:1715–23. Siu SC, Levine RA, Rivera JM, et al. Three-dimensional echocardiography improves noninvasive assessment of left ventricular volume and performance. Am Heart J 1995;130:812–22. Jiang L, Morrissey R, Handschumacher MD, et al. Quantitative threedimensional reconstruction of left ventricular volume with complete borders detected by acoustic quantification underestimates volume. Am Heart J 1996;131:553–9. King DL, Harrison MR, King DL, Jr., Gopal AS, Martin RP, DeMaria AN. Improved reproducibility of left atrial and left ventricular measurements by guided three-dimensional echocardiography. J Am Coll Cardiol 1992;20: 1238 – 45. Rivera JM, Siu SC, Handschumacher MD, et al. Three-dimensional reconstruction of ventricular septal defects: validation studies and in vivo feasibility. J Am Coll Cardiol 1994;23:201– 8. Sheikh KH, Smith SW, Von Ramm O, Kisslo J. Real-time, threedimensional echocardiography: feasibility and initial use. Echocardiography 1991;8:119 –25. Schwammenthal E, Chen C, Benning F, Block M, Breithardt G, Levine RA. Dynamics of mitral regurgitation flow and orifice area. Circulation 1994;90: 307–22. Enriquez-Sarano M, Sinak LJ, Tajik AJ, Bailey KR, Seward JB. Changes in effective regurgitant orifice throughout systole in patients with mitral valve prolapse. A clinical study using the proximal isovelocity surface area method. Circulation 1995;92:295– 8.