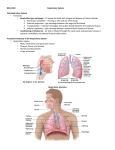
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Faculty/Presenter Disclosure • • • Faculty: Program: Topic : • Relationships with commercial interests: Dr. Anthony Ciavarella MD 51st Annual Scientific Assembly, OCFP Community Acquired Respiratory Tract Infections: The usual suspects – Speakers Bureau/Honoraria: Merck Frosst, Pfizer, Bayer. – Consulting Fees: Merck Frosst, Boehringer Ingelheim Disclosure of Commercial Support Community Acquired Respiratory Tract Infections: The usual suspects Statement : This program has received no commercial financial support. Potential for conflict(s) of interest: Dr. Anthony Ciavarella MD has received honoraria from: Merck Frosst, Pfizer, Bayer, and Boehringer Ingelheim. • None of these organizations are supporting this program. • No associated product is being discussed in this program. Mitigating Potential Bias Community Acquired Respiratory Tract Infections: The usual suspects 1. The content of this talk is not about products or services of any company or group or organization with outside or commercial interest. 2. The information presented is explicitly ‘‘evidence-based’’. 3. Sufficient time will be allowed for the audience to read and comprehend the information being shared. 4. There will be opportunity for the audience to ask questions about the disclosure should they arise. Community Acquired Respiratory Tract Infections CARTI: The Usual Suspects Group A Strep throat Acute Bacterial Rhino Sinusitis Bronchitis ‘Common cold’ The ‘Flu’ Allergic Rhinitis Acute Otitis Media Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections CARTI: The Usual Suspect Tools Allergic Rhinitis1 Sneezing Nasal Obstruction Nasal Itch (pruritus) Nasal Rhinorrhea + Itchy watery Eyes (conjunctivits) SOIRE ABRS2 Facial Pain/pressure/ fullness Nasal Obstruction ‘Cold’ 3 ‘Strep’ 5 Sore throat sneezing Fever+Cough >38°C 1. Fever >38°C Myalgia 2. Tender ant. Cough Rapid Onset < 48 hrs cervical Adenopathy Nasal Chills or Sweating Obstruction 3. Tonsillar swelling Nasal Purulence/ Nasal discoloured Rhinorrhea postnasal Discharge Ill feeling hyposmia/anosmia Everywhere (Smell) PODS ‘Flu’ 4 SCORE or exudate 4. Age 3 to 14 5. No cough Flu Can Make Rapid Chills or Sweating FAT And No cough 1. Small P, Frnkiel S, Becker A, et al.. Journal of Otolaryngology. 2007;36(Supl 1):S5-S27. 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. http://www.ccohs.ca/oshanswers/diseases/common_cold.html accessed 2013 October 21 4. Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 5. McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue-1/0075.ht adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections CARTI: The Unusual Suspects Mononucleosis Acute Frontal Bacterial Rhino Sinusitis Acute Exacerbation COPD Pertussis Community Acquired Pneumonia Asthma worsening Tuberculosis Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections CARTI: The Unusual Suspect Tools WCBC + S CAP1 Cough Fever Pleuritic chest pain Physical Examination Sputum probable CXR necessary CURB -65 Frontal Sinusitis2 Fever; Rapid onset Chills & sweating Frontal sinus pain POSSIBLE Systemic symptoms Neurological symptoms Occular symptoms PODS AECOPD3 Sustained Worsening of dyspnea (SOB), Cough or Phlegm production leading to an increase in the use of Maintenance Medications and/or supplemental with Additional Medications Cough Phlegm SOB Worsening & More Medicine Asthma Worsening4 Asthma symptoms Day > 4 days / wk Any Night time Asthma symptoms Any interference with Usual Activities or exercise 4. Flow < 80% of personal best 5. Reliever medication > 4 doses / wk (including exercise) 6. Sputum Eosinophils > 3%. 7. Employment or school - any days lost 8. Exacerbation frequent within the past year or any not mild exacerbations. 1. 2. 3. DNA FREE E 1. RR, Lemonovich TL. Diagnosis and management of CAPin adults. Am Fam Physician. 2011 Jun 1;83(11):1299-306. PubMed PMID: 21661712 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. O’Donnell DE, Hernandez P, Kaplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.. 4. Lougheed MD et al; Canadian Thoracic Society 2012; Can Respir J Vol 19 No 2 March/April 2012 adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections Viral URTI*: Symptom Severity vs. Time Severity Fever Respiratory Symptoms *URTI Upper Respiratory Tract Infection 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Adapted from Wald E.R. et al; Clinical Practice Guideline for the Diagnosis and Management of Acute Bacterial Sinusitis in Children Aged 1 to 18 Years; American Academy of Pediatrics; (doi: 10.1542/peds.2013-1071) Community Acquired Respiratory Tract Infections CARTI: The Usual Suspects Group A Strep throat Acute Bacterial Rhino Sinusitis Bronchitis ‘Common cold’ The ‘Flu’ Allergic Rhinitis Acute Otitis Media Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections Common Cold: Symptom Pattern • Early signs of a cold are a: ‘Common cold’ – Sore, Scratchy throat Sore throat sneezing – Sneezing Cough – Runny nose Nasal Obstruction • Other symptoms that may occur later include: Nasal Rhinorrhea ill feeling Everywhere – Headache – Stuffy nose (Obstruction) – Watering eyes – Hacking Cough – ill-feeling Everywhere: Chills, muscle aches, and general malaise Duration 2 to 7 days Some Cases May Last for 2 Weeks Canadian Centre for Occupational Health and Safety; http://www.ccohs.ca/oshanswers/diseases/common_cold.html#_1_2 accessed 2013 October Community Acquired Respiratory Tract Infections CARTI: ‘common cold’ symptoms Severity ‘Common cold’ Sore throat sneezing Cough Nasal Obstruction Fever Nasal Rhinorrhea ‘cold’ symptoms ill feeling Everywhere Duration 2 to 7 days 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 Canadian Centre for Occupational Health and Safety; http://www.ccohs.ca/oshanswers/diseases/common_cold.html#_1_2 18 19 20 accessed 2013 October 21 Community Acquired Respiratory Tract Infections CARTI: ‘common cold’ SCORE Severity ‘Common cold’ Sore throat sneezing Cough Nasal Obstruction Fever Nasal Rhinorrhea SCORE ill feeling Everywhere Duration 2 to 7 days 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 Canadian Centre for Occupational Health and Safety; http://www.ccohs.ca/oshanswers/diseases/common_cold.html#_1_2 18 19 20 accessed 2013 October 21 Community Acquired Respiratory Tract Infections Acute Bacterial Rhino Sinusitis: Biphasic Pattern Severity ABRS Facial Pain/pressure/fullness Nasal Obstruction Nasal Purulence/discoloured postnasal Discharge hyposmia/anosmia (Smell) SCORE worsening after 5 to 7 days with similar symptoms 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Community Acquired Respiratory Tract Infections Acute Bacterial Rhino Sinusitis: PODS Severity ABRS Facial Pain/pressure/fullness Nasal Obstruction Nasal Purulence/discoloured postnasal Discharge SCORE hyposmia/anosmia (Smell) PODS worsening after 5 to 7 days with similar symptoms 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Community Acquired Respiratory Tract Infections Acute Bacterial Rhino Sinusitis: Diagnosis P Facial Pain/Pressure/ Fullness O Nasal Obstruction D Nasal Purulence/ Discolored Postnasal Discharge S Hyposmia/ Anosmia (Smell) ABRS diagnosis requires the presence of at least 2 major PODS symptoms; Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Community Acquired Respiratory Tract Infections Acute Bacterial Rhino Sinusitis: Diagnosis P Facial Pain/Pressure/ Fullness O Nasal Obstruction D Nasal Purulence/ Discolored Postnasal Discharge S Hyposmia/ Anosmia (Smell) ABRS diagnosis requires the presence of at least 2 major PODS symptoms; 1 symptom must be: nasal Obstruction or nasal purulence/discoloured postnasal Discharge 1. Worsening after 5 to 7 days (biphasic illness) with similar symptoms 2. Symptoms persist more than 7 days without improvement 3. Presence of purulence for 3 to 4 days with high fever Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Community Acquired Respiratory Tract Infections Acute Bacterial Rhino Sinusitis: Persistent Pattern Severity *ABRS Facial Pain/pressure/fullness Nasal Obstruction Nasal Purulence/discoloured postnasal Discharge PODS hyposmia/anosmia (Smell) more than 7 days without improvement 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Community Acquired Respiratory Tract Infections Acute Bacterial Rhino Sinusitis: Purulence with high fever Severity Fever ABRS PODS Facial Pain/pressure/fullness Nasal Obstruction Nasal Purulence/discoloured postnasal Discharge Presence of purulence for 3 to 4 days with high fever 00 01 02 03 04 05 06 07 08 09 10 hyposmia/anosmia (Smell) 11 12 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Community Acquired Respiratory Tract Infections CARTI: The Usual Suspects Group A Strep throat Acute Bacterial Rhino Sinusitis Bronchitis ‘Common cold’ The ‘Flu’ Allergic Rhinitis Acute Otitis Media Dr. Anthony Ciavarella BA MA MD0Common Respiratory Tract Infections: CARTI: The Usual Suspects; FMF 20136 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections CARTI: The Unusual Suspects Mononucleosis Acute Frontal Bacterial Rhino Sinusitis Acute Exacerbation COPD Pertussis Community Acquired Pneumonia Asthma worsening Tuberculosis Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School CARTI: an unusual suspect Acute Frontal Sinusitis: Purulence with high fever Severity Fever PODS PODS: Rapid onset with fever Chills & sweating Frontal sinus pain Any of: Acute Frontal sinusitis Requires urgent care. 00 01 02 03 04 05 06 07 08 09 10 11 12 Systemic symptoms Neurological symptoms Occular symptoms 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Canadian Centre for Occupational Health and Safety; http://www.ccohs.ca/oshanswers/diseases/common_cold.html#_1_2 accessed 2013 October CARTI: an unusual suspect Acute Frontal Sinusitis: Requires urgent care Severity Fever PODS PODS: Rapid onset with fever Chills & sweating Frontal sinus pain Any of: Acute Frontal sinusitis Requires urgent care. 00 01 02 03 04 05 06 07 08 09 10 11 12 Systemic symptoms Neurological symptoms Occular symptoms 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Canadian Centre for Occupational Health and Safety; http://www.ccohs.ca/oshanswers/diseases/common_cold.html#_1_2 accessed 2013 October Community Acquired Respiratory Tract Infections CARTI: The Usual Suspects Group A Strep throat Acute Bacterial Rhino Sinusitis Bronchitis ‘Common cold’ The ‘Flu’ Allergic Rhinitis Acute Otitis Media Dr. Anthony Ciavarella BA MA MD0Common Respiratory Tract Infections: CARTI: The Usual Suspects; FMF 20136 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections Rapid Onset with Fever Severity Fever+Cough Fever Rapid Onset < 48 hrs Fever + Cough Myalgia Flu Can Make Rapid Chills or Sweating 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections Rapid Onset with Fever: Influenza Fever+Cough Influenza Fever+Cough >38°C Severity Myalgia Rapid Onset < 48 hrs Myalgia Rapid Onset < 48 hrs Chills or Sweating Chills or Sweating Fever + Cough Myalgia Flu Can Make Rapid Chills or Sweating 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections Influenza Diagnosis Tool This Influenza Diagnosis Tool gives direction. The clinical diagnosis of influenza by exclusion. Fever + Cough = 2 points Myalgia = 2 points Rapid Onset < 48 hrs = 1 points Chills or Sweats = 1 point High risk 4 - 6 points = 59% Flu Can Make Rapid Chills or Sweating Ebell M.H. et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. J Am Board Fam Med. January-February 2012 vol. 25 no. 1 55-62 Community Acquired Respiratory Tract Infections Rapid Onset with Fever and No cough Severity Fever No cough Fever Adenopathy Tonsillar swelling or exudate FAT And No cough 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue1/0075.ht adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections Rapid Onset with Fever and No cough: Group A Strep Fever Group A Strep Severity Tender ant. cervical Adenopathy Fever >38°C Tender ant. cervical Adenopathy Tonsillar swelling or exudate Age 3 to 14 No cough Tonsillar swelling or exudate Age 3 to 14 No cough Fever Adenopathy Tonsillar swelling or exudate FAT And No cough 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue-1/0075.ht adapted by Dr. A. Ciavarella MD CARTI: Group A Strep throat GAS Assessment FAT And No cough Point Fever; temperature >38°C 1 AdenopathyTender Anterior cervical 1 Tonsillar swelling or exudate 1 Age 3–14 year 1 No cough 1 Age 15–44 year 0 Age ≥45 year -1 McIsaac WJ et al. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ 1998;158:75-83 McIsaac WJ et.al. The validity of a sore throat score in family practice; CMAJ October 3, 2000 vol. 163 no. 7 CARTI: Group A Strep throat GAS Management F A T And No cough Score < 1 Score = 2 Score = 3 Score > 4 Risk <6% Risk 10–28% Risk 38-63% No Culture or antibiotic is required Culture all. Treat only if culture result is positive Culture all. Treat with penicillin on clinical grounds* *If patient has high temperature or is clinically unwell, and presents early in disease course McIsaac WJ et al.; A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ 1998;158:75-83 McIsaac WJ et.al.;The validity of a sore throat score in family practice; CMAJ October 3, 2000 vol. 163 no. 7 Community Acquired Respiratory Tract Infections CARTI: The Usual Suspect Tools Allergic Rhinitis1 Sneezing Nasal Obstruction Nasal Itch (pruritus) Nasal Rhinorrhea + Itchy watery Eyes (conjunctivits) SOIRE ABRS2 Facial Pain/pressure/ fullness Nasal Obstruction ‘Cold’ 3 ‘Strep’ 5 Sore throat sneezing Fever+Cough >38°C 1. Fever >38°C Myalgia 2. Tender ant. Cough Rapid Onset < 48 hrs cervical Adenopathy Nasal Chills or Sweating Obstruction 3. Tonsillar swelling Nasal Purulence/ Nasal discoloured Rhinorrhea postnasal Discharge Ill feeling hyposmia/anosmia Everywhere (Smell) PODS ‘Flu’ 4 SCORE or exudate 4. Age 3 to 14 5. No cough Flu Can Make Rapid Chills or Sweating FAT And No cough 1. Small P, Frnkiel S, Becker A, et al.. Journal of Otolaryngology. 2007;36(Supl 1):S5-S27. 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. http://www.ccohs.ca/oshanswers/diseases/common_cold.html accessed 2013 October 21 4. Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 5. McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue-1/0075.ht adapted by Dr. A. Ciavarella MD Allergic Rhinitis S O I R E Sneezing Nasal Obstruction Nasal Itch (pruritus) Nasal Rhinorrhea + Itchy Watery Eyes (conjunctivits) Allergic Rhinitis Diagnosis: 2 or More of ‘S O I R E’ Symptoms for More Than 1 Hour on Most Days ● The previous classification of seasonal or perennial Allergic Rhinitis is being replaced with intermittent and persistent Allergic Rhinitis1 ● Intermittent episode = symptoms last <6 weeks ● Persistent episode = symptoms last >6 weeks 1. Small P. et al. Rhinitis: A practical and comprehensive approach to assessment and therapy. Journal of Otolaryngology. 2007;36(Supl 1):S5-S27. CARTI: The Usual Suspects Diagnoses Clinical Clinical Clinical Clinical Throat Swab Allergic Rhinitis1 ABRS2 ‘Cold’ 3 ‘Flu’ 4 ‘Strep’ 5 Sneezing Nasal Obstruction Nasal Itch (pruritus) Nasal Rhinorrhea + Itchy watery Eyes (conjunctivits) allergy testing when convenient Facial Pain/pressure/ fullness Nasal Obstruction Sore throat sneezing Fever+Cough >38°C 1. Fever >38°C Myalgia 2. Tender ant. Cough Rapid Onset < 48 hrs cervical Adenopathy Nasal Chills or Sweating Obstruction 3. Tonsillar swelling Nasal Purulence/ Nasal discoloured Rhinorrhea postnasal Discharge Ill feeling hyposmia/anosmia Everywhere (Smell) nasal swabs or sinus x-rays not necessary no investigations Investigations not necessary. Posterior nasophryngeal swab optional. or exudate 4. Age 3 to 14 5. No cough Throat Swab Necessary. 1. Small P, Frnkiel S, Becker A, et al.. Journal of Otolaryngology. 2007;36(Supl 1):S5-S27. 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. http://www.ccohs.ca/oshanswers/diseases/common_cold.html accessed 2013 October 21 4. Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 5. McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue-1/0075.ht adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections CARTI: The Usual Suspects Group A Strep throat Acute Bacterial Rhino Sinusitis Bronchitis ‘Common cold’ The ‘Flu’ Allergic Rhinitis Acute Otitis Media Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections CARTI: Bronchitis symptoms self limiting respiratory symptoms lasting up to 3 weeks 2 Severity Fever < 3 days Chest discomfort Sputum production Wheezes might be present 00 1. 2. 3. 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 ROSS H. ALBERT ; Diagnosis and Treatment of Acute Bronchitis Am Fam Physician. 2010 Dec 1;82(11):1345-1350. http://www.aafp.org/afp/2010/1201/p1345.html Little P. et al. Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial. JAMA. 2005;293(24):3029–3035.. Gwaltney J. Acute bronchitis. In: Mandell G, Bennett J, and Dolin R (eds.). Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 5th edition, Churchill and Livingstone, Edinburgh, 2000. 21 Community Acquired Respiratory Tract Infections CARTI: Bronchitis self limiting respiratory symptoms lasting up to 3 weeks 2 Severity Fever < 3 days Chest discomfort Green/yellow sputum production is indicative of inflammation and does not reliably differentiate between bacterial and viral lower respiratory tract infections.2 00 1. 2. 3. 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 Sputum production Wheezes might be present 17 18 19 20 ROSS H. ALBERT ; Diagnosis and Treatment of Acute Bronchitis Am Fam Physician. 2010 Dec 1;82(11):1345-1350. http://www.aafp.org/afp/2010/1201/p1345.html Little P. et al. Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial. JAMA. 2005;293(24):3029–3035.. Gwaltney J. Acute bronchitis. In: Mandell G, Bennett J, and Dolin R (eds.). Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 5th edition, Churchill and Livingstone, Edinburgh, 2000. 21 Community Acquired Respiratory Tract Infections CARTI: Bronchitis symptoms Severity Antibiotics are generally not indicated for bronchitis, and should be used only if pertussis is suspected to reduce transmission or if the patient is at increased risk of developing pneumonia (e.g., patients 65 years or older*). Fever < 3 days Chest discomfort Green/yellow sputum production is indicative of inflammation and does not reliably differentiate between bacterial and viral lower respiratory tract infections.2 00 1. 2. 3. 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 Sputum production Wheezes might be present 17 18 19 20 ROSS H. ALBERT ; Diagnosis and Treatment of Acute Bronchitis Am Fam Physician. 2010 Dec 1;82(11):1345-1350. http://www.aafp.org/afp/2010/1201/p1345.html Little P. et al. Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial. JAMA. 2005;293(24):3029–3035.. Gwaltney J. Acute bronchitis. In: Mandell G, Bennett J, and Dolin R (eds.). Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 5th edition, Churchill and Livingstone, Edinburgh, 2000. 21 Community Acquired Respiratory Tract Infections CARTI: Bronchitis symptoms Severity Antibiotics are generally not indicated for bronchitis, and should be used only if pertussis is suspected to reduce transmission or if the patient is at increased risk of developing pneumonia (e.g., patients 65 years or older*). *NNT is 39 in patients 65 years or older 1 . Fever < 3 days Chest discomfort Green/yellow sputum production is indicative of inflammation and does not reliably differentiate between bacterial and viral lower respiratory tract infections.2 00 1. 2. 3. 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 Sputum production Wheezes might be present 17 18 19 20 ROSS H. ALBERT ; Diagnosis and Treatment of Acute Bronchitis Am Fam Physician. 2010 Dec 1;82(11):1345-1350. http://www.aafp.org/afp/2010/1201/p1345.html Little P. et al. Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial. JAMA. 2005;293(24):3029–3035.. Gwaltney J. Acute bronchitis. In: Mandell G, Bennett J, and Dolin R (eds.). Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 5th edition, Churchill and Livingstone, Edinburgh, 2000. 21 Community Acquired Respiratory Tract Infections CARTI: The Unusual Suspect Tools CAP1 Cough Fever Pleuritic chest pain Physical Examination Sputum probable CXR necessary CURB -65 1. RR, Lemonovich TL. Diagnosis and management of CAPin adults. Am Fam Physician. 2011 Jun 1;83(11):1299-306. PubMed PMID: 21661712 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. O’Donnell DE, Hernandez P, Kaplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.. 4. Lougheed MD et al; Canadian Thoracic Society 2012; Can Respir J Vol 19 No 2 March/April 2012 adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections CARTI: Bronchitis symptoms Severity Antibiotics are generally not indicated for bronchitis, and should be used only if pertussis is suspected to reduce transmission or if the patient is at increased risk of developing pneumonia (e.g., patients 65 years or older*). *NNT is 39 in patients 65 years or older 1 . Fever < 3 days Chest discomfort Sputum production Wheezes might be present Green/yellow sputum production: is indicative of inflammation and does not reliably differentiate between bacterial and viral lower respiratory tract infections.2 00 1. 2. 3. 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 ROSS H. ALBERT ; Diagnosis and Treatment of Acute Bronchitis Am Fam Physician. 2010 Dec 1;82(11):1345-1350. http://www.aafp.org/afp/2010/1201/p1345.html Little P. et al. Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial. JAMA. 2005;293(24):3029–3035.. Gwaltney J. Acute bronchitis. In: Mandell G, Bennett J, and Dolin R (eds.). Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 5th edition, Churchill and Livingstone, Edinburgh, 2000. 21 CARTI: Unusual Suspects Pertussis Typical Clinical Phases* Paroxysmal Cough Cough Paroxysmal Cough Whooping Vomiting Cyanosis Apnea Catarrhal: Mild cough Runny nose Mild fever Apnea in infants Convalescent: Cough less paroxysmal disappears in weeks *The illness can be milder and the typical "whoop" absent in children, teens, and adults who have been vaccinated with a pertussis vaccine. Incubation 7-10 days Catarrhal 00 01 Paroxysmal 02 03 04 05 Convalescent 06 07 Tozzi A.E.; Diagnosis and management of pertussis; CMAJ 2005;172(4):509-15 08 weeks to months Community Acquired Respiratory Tract Infections CARTI: Bronchitis self limiting respiratory symptoms lasting up to 3 weeks 2 Severity Fever < 3 days Chest discomfort Sputum production Wheezes might be present Green/yellow sputum production: is indicative of inflammation and does not reliably differentiate between bacterial and viral lower respiratory tract infections.2 00 1. 2. 3. 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 ROSS H. ALBERT ; Diagnosis and Treatment of Acute Bronchitis Am Fam Physician. 2010 Dec 1;82(11):1345-1350. http://www.aafp.org/afp/2010/1201/p1345.html Little P. et al. Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial. JAMA. 2005;293(24):3029–3035.. Gwaltney J. Acute bronchitis. In: Mandell G, Bennett J, and Dolin R (eds.). Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 5th edition, Churchill and Livingstone, Edinburgh, 2000. 21 Community Acquired Respiratory Tract Infections CARTI: Unusual Suspect AECOPD AECOPD3 Sustained Worsening of dyspnea (SOB), Cough or Phlegm production leading to an increase in the use of Maintenance Medications and/or supplemental with Additional Medications Cough Phlegm SOB Worsening & More Medicine 1. RR, Lemonovich TL. Diagnosis and management of CAPin adults. Am Fam Physician. 2011 Jun 1;83(11):1299-306. PubMed PMID: 21661712 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. O’Donnell DE, Hernandez P, Kaplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.. 4. Lougheed MD et al; Canadian Thoracic Society 2012; Can Respir J Vol 19 No 2 March/April 2012 adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections CARTI: Bronchitis self limiting respiratory symptoms lasting up to 3 weeks 2 Severity Fever < 3 days Chest discomfort Sputum production Wheezes might be present Green/yellow sputum production: is indicative of inflammation and does not reliably differentiate between bacterial and viral lower respiratory tract infections.2 00 1. 2. 3. 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 ROSS H. ALBERT ; Diagnosis and Treatment of Acute Bronchitis Am Fam Physician. 2010 Dec 1;82(11):1345-1350. http://www.aafp.org/afp/2010/1201/p1345.html Little P. et al. Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial. JAMA. 2005;293(24):3029–3035.. Gwaltney J. Acute bronchitis. In: Mandell G, Bennett J, and Dolin R (eds.). Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. 5th edition, Churchill and Livingstone, Edinburgh, 2000. 21 Community Acquired Respiratory Tract Infections CARTI: Unusual Suspect Asthma Worsening WCBC + S Asthma Worsening4 Asthma symptoms Day > 4 days / wk Any Night time Asthma symptoms Any interference with Usual Activities or exercise 4. Flow < 80% of personal best 5. Reliever medication > 4 doses / wk (including exercise) 6. Sputum Eosinophils > 3%. 7. Employment or school - any days lost 8. Exacerbation frequent within the past year or any not mild exacerbations. 1. 2. 3. DNA FREE E 1. RR, Lemonovich TL. Diagnosis and management of CAPin adults. Am Fam Physician. 2011 Jun 1;83(11):1299-306. PubMed PMID: 21661712 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. O’Donnell DE, Hernandez P, Kaplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.. 4. Lougheed MD et al; Canadian Thoracic Society 2012; Can Respir J Vol 19 No 2 March/April 2012 adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections CARTI: Unusual Suspect Tools WCBC + S CAP1 Cough Fever Pleuritic chest pain Physical Examination Sputum probable CXR necessary CURB -65 Frontal Sinusitis2 Fever; Rapid onset Chills & sweating Frontal sinus pain POSSIBLE Systemic symptoms Neurological symptoms Occular symptoms PODS AECOPD3 Sustained Worsening of dyspnea (SOB), Cough or Phlegm production leading to an increase in the use of Maintenance Medications and/or supplemental with Additional Medications Cough Phlegm SOB Worsening & More Medicine Asthma Worsening4 Asthma symptoms Day > 4 days / wk Any Night time Asthma symptoms Any interference with Usual Activities or exercise 4. Flow < 80% of personal best 5. Reliever medication > 4 doses / wk (including exercise) 6. Sputum Eosinophils > 3%. 7. Employment or school - any days lost 8. Exacerbation frequent within the past year or any not mild exacerbations. 1. 2. 3. DNA FREE E 1. RR, Lemonovich TL. Diagnosis and management of CAPin adults. Am Fam Physician. 2011 Jun 1;83(11):1299-306. PubMed PMID: 21661712 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. O’Donnell DE, Hernandez P, Kaplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.. 4. Lougheed MD et al; Canadian Thoracic Society 2012; Can Respir J Vol 19 No 2 March/April 2012 adapted by Dr. A. Ciavarella MD CARTI: The Usual Suspects ?Antibiotics? NO NO Allergic Rhinitis1 Sneezing Nasal Obstruction Nasal Itch (pruritus) Nasal Rhinorrhea + Itchy watery Eyes (conjunctivits) ABRS2 Facial Pain/pressure/ fullness Nasal Obstruction ‘Cold’ 3 NO ‘Flu’ 4 YES ‘Strep’ 5 Sore throat sneezing Fever+Cough >38°C 1. Fever >38°C Myalgia 2. Tender ant. Cough Rapid Onset < 48 hrs cervical Adenopathy Nasal Chills or Sweating Obstruction 3. Tonsillar swelling Nasal Purulence/ Nasal discoloured Rhinorrhea postnasal Discharge Ill feeling hyposmia/anosmia Everywhere (Smell) or exudate 4. Age 3 to 14 5. No cough Culture all. Treat with penicillin on clinical grounds* 1. Small P, Frnkiel S, Becker A, et al.. Journal of Otolaryngology. 2007;36(Supl 1):S5-S27. 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. http://www.ccohs.ca/oshanswers/diseases/common_cold.html accessed 2013 October 21 4. Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 5. McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue-1/0075.ht adapted by Dr. A. Ciavarella MD CARTI: Group A Strep throat GAS Management F A T And No cough Score < 1 Score = 2 Score = 3 Score > 4 Risk <6% Risk 10–28% Risk 38-63% No Culture or antibiotic is required Culture all. Treat only if culture result is positive Culture all. Treat with penicillin on clinical grounds* *If patient has high temperature or is clinically unwell, and presents early in disease course McIsaac WJ et al.; A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ 1998;158:75-83 McIsaac WJ et.al.;The validity of a sore throat score in family practice; CMAJ October 3, 2000 vol. 163 no. 7 CARTI: The Usual Suspects ?Antibiotics? Maybe Allergic Rhinitis1 Sneezing Nasal Obstruction Nasal Itch (pruritus) Nasal Rhinorrhea + Itchy watery Eyes (conjunctivits) ABRS2 Facial Pain/pressure/ fullness Nasal Obstruction ‘Cold’ 3 ‘Flu’ 4 ‘Strep’ 5 Sore throat sneezing Fever+Cough >38°C 1. Fever >38°C Myalgia 2. Tender ant. Cough Rapid Onset < 48 hrs cervical Adenopathy Nasal Chills or Sweating Obstruction 3. Tonsillar swelling Nasal Purulence/ Nasal discoloured Rhinorrhea postnasal Discharge Ill feeling hyposmia/anosmia Everywhere (Smell) or exudate 4. Age 3 to 14 5. No cough 1. Small P, Frnkiel S, Becker A, et al.. Journal of Otolaryngology. 2007;36(Supl 1):S5-S27. 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. http://www.ccohs.ca/oshanswers/diseases/common_cold.html accessed 2013 October 21 4. Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 5. McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue-1/0075.ht adapted by Dr. A. Ciavarella MD CARTI Treatment: ABRS Purulence with high fever Severity Antibiotics Yes Fever PODS Presence of purulence for 3 to 4 days with high fever 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 CARTI Treatment: ABRS: Persistent or Biphasic illness Severity Antibiotics maybe Persistent Biphasic illness PODS SCORE 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Algorithm for the Diagnosis & Treatment of ABRS Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 ABRS: Mild, Moderate or Severe None Major Symptoms P Facial Pain/ Pressure/Fullness O Nasal Obstruction D Nasal Purulence/Discolored Postnasal Discharge S Hyposmia/Anosmia (Smell) Mild Moderate Severe Occasional Limited Episode Steady Symptoms but Easily Tolerated Hard to Tolerate & May Interfere with Activity or Sleep ABRS diagnosis requires the presence of at least 2 major PODS symptoms; 1 symptom must be nasal Obstruction or nasal purulence/discoloured postnasal Discharge Consider ABRS Under Any One of the Following Conditions 1) Worsening after 5 to 7 days (biphasic illness) with similar symptoms 2) Symptoms persist more than 7 days without improvement 3) Presence of purulence for 3 to 4 days with high fever Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 ABRS: Case 1 • Previously healthy 32-year-old non-smoking mother • Recent onset of symptoms of an upper respiratory tract infection (URTI) – Persistent nasal obstruction – Right-sided maxillary facial pain – Yellowish secretions • Have lasted 9 days from the outset but has not limited work / family activities • Have not responded to OTC medication Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 ABRS: Case 1 • Previously healthy 32-year-old non-smoking mother • Recent onset of symptoms of an upper respiratory tract infection (URTI) – Persistent nasal obstruction – Right-sided maxillary facial pain – Yellowish secretions • Have lasted 9 days from the outset but has not limited work / family activities • Have not responded to OTC medication Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 ABRS: Mild, Moderate None Major Symptoms P Facial Pain/ Pressure/Fullness O Nasal Obstruction D Nasal Purulence/Discolored Postnasal Discharge S Hyposmia/Anosmia (Smell) Mild Moderate Severe Occasional Limited Episode Steady Symptoms but Easily Tolerated Hard to Tolerate & May Interfere with Activity or Sleep ABRS diagnosis requires the presence of at least 2 major PODS symptoms; 1 symptom must be nasal Obstruction or nasal purulence/discoloured postnasal Discharge Consider ABRS Under Any One of the Following Conditions 1) Worsening after 5 to 7 days (biphasic illness) with similar symptoms 2) Symptoms persist more than 7 days without improvement 3) Presence of purulence for 3 to 4 days with high fever Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Algorithm for the Diagnosis & Treatment of ABRS Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 CARTI: ABRS Treatment INCS vs antibiotics Mean change from baseline (days 2-15) Baseline scores: 8.36 8.53 8.17 Placebo (n=247) Amoxicillin 0.5 g TID (n=249) MFNS 200 µg OD (n=240) 8.28 MFNS 200 µg BID (n=234) -3.6 -3.8 -3.75 -4.0 -4.01 -4.13 -4.2 -4.4 -4.51 -4.6 *P<0.05 vs. Placebo P=0.057 vs. Amoxicillin *† Change in mean AM/PM major symptom score from baseline over treatment period (days 2-15) Meltzer et al. J Allergy Clin Immunol. 2005;116:1289. Algorithm for the Diagnosis & Treatment of ABRS Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 ABRS: Case 2 • Previously healthy 32-year-old non-smoking mother • Recent onset of symptoms of an upper respiratory tract infection (URTI) – – – – Persistent nasal obstruction Right-sided maxillary facial pain Yellowish secretions now interfering with sleep • Have lasted 2 weeks from the outset and has not responded to INCS medication Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg ABRS: Case 2 • Previously healthy 32-year-old non-smoking mother • Recent onset of symptoms of an upper respiratory tract infection (URTI) – – – – Persistent nasal obstruction Right-sided maxillary facial pain Yellowish secretions now interfering with sleep • Have lasted 2 weeks from the outset and has not responded to INCS medication Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg ABRS: Severe None Major Symptoms P Facial Pain/ Pressure/Fullness O Nasal Obstruction D Nasal Purulence/Discolored Postnasal Discharge S Hyposmia/Anosmia (Smell) Mild Moderate Severe Occasional Limited Episode Steady Symptoms but Easily Tolerated Hard to Tolerate & May Interfere with Activity or Sleep ABRS diagnosis requires the presence of at least 2 major PODS symptoms; 1 symptom must be nasal Obstruction or nasal purulence/discoloured postnasal Discharge Consider ABRS Under Any One of the Following Conditions 1) Worsening after 5 to 7 days (biphasic illness) with similar symptoms 2) Symptoms persist more than 7 days without improvement 3) Presence of purulence for 3 to 4 days with high fever Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Algorithm for the Diagnosis & Treatment of ABRS Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 First-line Therapy • In severe ABRS • In Moderate ABRS if INCS are not efficacious • Antibiotics recommended: – Amoxicillin 500 mg TID – Macrolide for penicillin-allergic Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 Algorithm for the Diagnosis & Treatment of ABRS Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 April;40(2):S91 Second-line Therapy • Risk factors for immunosuppression • Symptoms suggesting frontal or sphenoid sinusitis • Presence of risk factors for antibiotic resistance – Previous antibiotic ≤3 months – Day care exposure – Failure of first-line antibiotic • Initial therapy with a second-line antibiotic – Amoxicillin/clavulanic acid 875 mg BID x 10–14d – Moxifloxacin 400 mg QD x 10–14d Canadian clinical practice guidelines for acute and chronic rhinosinusitis; Desrosiers M, Evans G, Keith P, Wright E, Kaplan A, Bouchard J, Ciavarella A et al. ; Allergy Asthma Clin Immunol. 2011 Feb 10;7(1):2., And J Otolaryngol Head Neck Surg. 2011 Community Acquired Respiratory Tract Infections CARTI: The Usual Suspects Group A Strep throat Acute Bacterial Rhino Sinusitis Bronchitis ‘Common cold’ The ‘Flu’ Allergic Rhinitis Acute Otitis Media Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections CARTI: The Unusual Suspects Mononucleosis Acute Frontal Bacterial Rhino Sinusitis Acute Exacerbation COPD Pertussis Community Acquired Pneumonia Asthma worsening Tuberculosis Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School Community Acquired Respiratory Tract Infections CARTI: Usual Suspect Tools Allergic Rhinitis1 Sneezing Nasal Obstruction Nasal Itch (pruritus) Nasal Rhinorrhea + Itchy watery Eyes (conjunctivits) SOIRE ABRS2 Facial Pain/pressure/ fullness Nasal Obstruction ‘Cold’ 3 ‘Strep’ 5 Sore throat sneezing Fever+Cough >38°C 1. Fever >38°C Myalgia 2. Tender ant. Cough Rapid Onset < 48 hrs cervical Adenopathy Nasal Chills or Sweating Obstruction 3. Tonsillar swelling Nasal Purulence/ Nasal discoloured Rhinorrhea postnasal Discharge Ill feeling hyposmia/anosmia Everywhere (Smell) PODS ‘Flu’ 4 SCORE or exudate 4. Age 3 to 14 5. No cough Flu Can Make Rapid Chills or Sweating FAT And No cough 1. Small P, Frnkiel S, Becker A, et al.. Journal of Otolaryngology. 2007;36(Supl 1):S5-S27. 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. http://www.ccohs.ca/oshanswers/diseases/common_cold.html accessed 2013 October 21 4. Ebell et al. ‘Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza’. JABFM Jan-Feb 2012 vol. 25 no. 1 55-62 5. McIsaac WJ et.al.CMAJ 1998;158:75-83. Available: www.cma.ca/cmaj/vol-158/issue-1/0075.ht adapted by Dr. A. Ciavarella MD Community Acquired Respiratory Tract Infections CARTI: Unusual Suspect Tools WCBC + S CAP1 Cough Fever Pleuritic chest pain Physical Examination Sputum probable CXR necessary CURB -65 Frontal Sinusitis2 Fever; Rapid onset Chills & sweating Frontal sinus pain POSSIBLE Systemic symptoms Neurological symptoms Occular symptoms PODS AECOPD3 Sustained Worsening of dyspnea (SOB), Cough or Phlegm production leading to an increase in the use of Maintenance Medications and/or supplemental with Additional Medications Cough Phlegm SOB Worsening & More Medicine Asthma Worsening4 Asthma symptoms Day > 4 days / wk Any Night time Asthma symptoms Any interference with Usual Activities or exercise 4. Flow < 80% of personal best 5. Reliever medication > 4 doses / wk (including exercise) 6. Sputum Eosinophils > 3%. 7. Employment or school - any days lost 8. Exacerbation frequent within the past year or any not mild exacerbations. 1. 2. 3. DNA FREE E 1. RR, Lemonovich TL. Diagnosis and management of CAPin adults. Am Fam Physician. 2011 Jun 1;83(11):1299-306. PubMed PMID: 21661712 2. Desrosiers et al.; Allergy, Asthma & Clinical Immunology 2011, 7:2 doi:10.1186/1710-1492-7-2; 3. O’Donnell DE, Hernandez P, Kaplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary care. Can Respir J. 2008;15(Suppl A):1A-8A.. 4. Lougheed MD et al; Canadian Thoracic Society 2012; Can Respir J Vol 19 No 2 March/April 2012 adapted by Dr. A. Ciavarella MD CARTI: Suspects Usual Acute Bacterial Rhino Sinusitis Influenza Group A Strep throat ‘Common cold’ Bronchitis & Unusual Acute frontal Bacterial Rhino Sinusitis Community Acquired Pneumonia Mononucleosis Pertussis Asthma worsening Acute Exacerbation COPD Allergic Rhinitis Tuberculosis Acute Otitis Media Dr. A. Ciavarella MD; Community Acquired Respiratory Tract Infections CARTI The Usual Suspects; FMF 2013 Gimli Glider Pilot School Family Medicine Forum College of Family Physicians of Canada Common Respiratory Tract Infections CARTI: The usual suspects Dr. Anthony Ciavarella BA MA MD MCFP FMF 2013 Vancouver BC