Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Umbilical cord wikipedia , lookup
Embryonic stem cell wikipedia , lookup
Large intestine wikipedia , lookup
Prenatal development wikipedia , lookup
Anatomical terms of location wikipedia , lookup
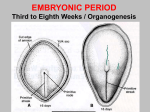
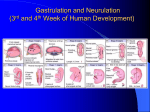
Drosophila embryogenesis wikipedia , lookup
Circulatory system wikipedia , lookup
STUDY TIPS FOR THE EMBRYO FINAL SPRING 1999 1. Where do somites come from? What structures do they form? Paraxial mesoderm somites skin, bone and muscle Tongue myoblasts derived from occipital somites 2. How do the fates of the mesonephric and paramesonephric ducts differ in the male and female? In males the Paramesonephric ducts regress Mesonephric Wolfian ducts epididymus, ductus deferens, ejaculatory duct In females the Mesonephric ducts regress Paramesonephric Müllerian ducts oviducts, uterus, upper vagina 3. Where does fertilization occur? Fertilization occurs in the ampulla mostly, other locations may result in inappropriate implantation. 4. When does the lung complete development? Alveolar development is from late fetal development to about age 8 years. During this time the alveoli mature completely, their walls become very thin to allow for extensive capillary contact. 5. How does the gut rotate and how much? The stomach? During the 6th week the duodenum rotates 270 degrees counterclockwise around the axis of the superior mesenteric artery accompanied by further elongation and coiling. The stomach rotates around the longitudinal axis first, by 90 degrees clockwise, leaving the anterior side inferiorly. Next it rotates around the anterior posterior axis by 90 degrees clockwise, so the left side is inferior and forms the greater curvature. 6. What cells arise from neuroepithelium of the neural tube? Neural crest? Neural tube gives rise to cells of the CNS Retina Pineal body Neurohypophysis Neural crest gives rise to cells that form most of the PNS and ANS cranial, spinal, and autonomic ganglia sensory ganglia of spinal nerves (dorsal root g. ) postganglionic neurons of the ANS Schwann cells Odontoblasts meninges Medulla of the adrenal gland Melanocytes Pharyngeal arch mesenchyme (First arch syndrome – failure of neural crest migration ) Head mesenchyme and CT ( cranial facial bones ) Bulbar and conal ridges of the heart (Abnormal valve leaflets – neural crest defect ) 7. Where is the primitive streak? What does it do? When does it form? The first thing to appear during gastrulation is the primitive streak. It forms at the caudal end of epiblast ( ~day 16 – beginning of the 3rd week) and is a thickened linear band of epiblast. It results from the proliferation and migration of cells of the epiblast to the median plane of the embryonic disc. As it elongates, it forms the primitive node. The primitive streak helps differentiate cranial /caudal end, dorsal /ventral surfaces, and right/ left sides. Shortly after the P.S. appears, cells leave its deep surface and form a loose network of embryonic CT called mesenchyme supporting tissue of the embryo, most of the body CT and stromal components of the glands and mesenchyme intraembryonic mesoderm. The primitive streak actively forms mesoderm until the early part of the 4th week, then it diminishes in size to become an insignificant structure in the sacrococcygeal region of the embryo. Normally it disappears by the end of the fourth week. 8. Syncytiotrophoblast: what does it do? Where does it come from? Develops about 6 days after fertilization. The outer mass of the trophoblast, consisting of a multinucleated protoplasmic mass in which no cell boundaries can be seen. The syncytiotrophoblast’s fingerlike projections extend through the endometrial epithelium and invade the connective tissue, thereby allowing the blastocyst to superficially implant. The syncytiotrophoblast expands quickly adjacent to the inner cell mass. It is probably responsible for hormone production. The Cytotrophoblast is highly mitotic and contributes cells to syncytiotrophoblast . 9. Know the phases of the ovarian and uterine cycles and the hormones responsible. 1 At the beginning (day 0) of the menstrual cycle all hormone levels are low. Low levels of GnRH are released, and it stimulates FSH and LH. FSH will stimulate follicular development over the next 14 days, and the LH stimulates estrogen production by the follicle. Estrogen levels subsequently rise and this causes neg. feedback on GnRH. In turn FSH and LH also rise. When levels of estrogen become “high”, it exerts positive feedback on GnRH and in turn on LH (great effect) and FSH (some effect). The LH surge causes rupture of the fully mature secondary oocyte from the Graffian follicle. After this happens, LH luteinizes the corpus hemorrhagicum and it becomes the corpus luteum. The C.L. under influence of LH, secretes Progesterone ( levels now rise ) and some estrogen – not as much as the developing follicle (levels are falling). The life span of the corpus luteum is short and it begins to degenerate into the corpus albicans less than 2 weeks after ovulation. Progesterone and estrogen levels drop off and GnRH is once again stimulated and the cycle starts again. Progesterone Menses 0-4 Proliferative 4-14 destruction of functionalis repair/regeneration Ovulation Luteal Phase 15-28 Graffian follicle UTERINE seretory phase Follicular Phase 1-14 follicle develops Secretory phase 15-28 Ovulation OVARIAN corpus luteum matures corpus albicans 10. How is the notochord formed? Where does it persist in the adult? The notochord is a cellular rod that develops by transformation of the notochordal process. It defines the primordial axis of the embryo and gives it some rigidity. It also serves as the basis for development of the axial skeleton and it is an intricate structure around which the vertebral column forms. The notochord degenerates as the bodies of the vertebrae form but it persists as the nucleus pulposus of each IVD. The developing notochord inducs the overlying embryonic ectoderm to thicken and form the neural plate, the primordium of the the CNS. (page 70) Notochord---mesenchymal(mesoderm) cells in midline from primitive pit to prechordal plate Notochordal process (hollow tube) notochordal plate notochord 11. Know the adult derivatives of the embryonic brain at about 5 weeks 3 primary vescicles 5 secondary vescicles Prosencephalon Telencephalon Diencephalon Mesencephalon Mesencephalon Rhombencephalon metencephalon Myelencephalon adult derivatives of walls … cerebral hemispheres thalamic structures Midbrain Pons Cerebellum Medulla and cavities lateral ventricles 3rd ventricle aqueduct upper part of 4th ventricle lower part of 4th ventricle 12. How are the limbs formed? Limbs come from somatic mesoderm from the lateral plate. Development begins at the 4 th week. The upper limbs appear first, but both upper and lower finish their morphogenesis around the 8th week. The apical ectodermal ridge (AER) is induced by mesoderm and itself induces mesoderm to form specific structures. It is essential for limb outgrowth and develoment and acts as a clock for the mesoderm: it tells when and what to form. The AER keeps underlying mesoderm in a highly mitotic state and the tissues that stay associate with it longer form the more distal structures. Around week 6 a flattened hand and foot plate appear. The AER is confined to the tips of the digital rays. Digits are formed by apoptosis. The zone of polarizing activity ( ZPA) at the caudal tip of the plate is made of 2 ectoderm and determines the order of the digits. It is thought that retinoic acid is responsible for this process. Cell fate determination occurs in steps based on temporal and spatial location and structures develop in proximal to distal sequence. The bones are formed by endochondral development starting at week 6 when cartilage appears, ossification begins during week 7. The upper limbs rotate laterally by 90 degrees, and the lower limbs rotate medially by 90 degrees. 13. What muscles develop from epimeres? hypomeres? Epimere ( dorsal ) extensor muscles of the neck and back Hypomere ( ventral ) thorax – external, internal, and innermost intercostals and transversus thoracic abdomen – external and internal obliques, transverse ebdominal ventral tip – rectus abdominis and infrahyoids diaphragm – myoblast migration into pleuroperitoneal membranes and leteral body wall, innervation by phrenic nerve carried in with myoblasts from cervical somites. Myotome regions of somites most skeletal mm Pharyngeal arch mesoderm some head and neck mm Somites myogenic precursor cells limb mm Splanchnic mesoderm cardiac and smooth mm 14. Know the divisions of the gut and their blood supply. Foregut supplied by celiac artery Esophagus Esophageal artresia, TE fistula ( both polyhydramnios ) Stomach Pyloric stenosis ( hypertrophy of mm) Duodenum Liver Artresia, double gall bladders Gall bladder Mesenteries dorsal greater o., ventral lesser o. Pancreas Annular pancreas ( incomplete rotation or 2 p.buds), accessory p. duct ( often in Meckel’s d. ) Midgut supplied by the superior mesenteric artery small intestine ( including most of the duodenum) cecum vermiform appendix ascending colon proximal 2/3 of the transverse colon Hindgut supplied by inferior mesenteric artery distal 1/3 of the transverse colon descending colon sigmoid colon rectum superior part of the anal canal bladder epithelium most of the urethra 15. What are the flexures of the developing brain and where are they? Flexures appear between the 4th and 8th week. The mesencephalic or cranial flexure is in the area of the midbrain. The cervical flexure is at the brain stem and the spinal cord, approximately at the level of the foramen magnum. Both the mesencephalic and the cervical flexures are ventral flexures. Later, unequal growth of the brain between these 2 flexures produces the pontine flexure which is located in the future pontine region and goes in the opposite direction . It divides the brain into the met- and myelencephalon. 16. What is the choroid plexus and where does it come from? The choroid plexus is a differentiation of the tela choroida, which consists of ependymal cells plus vascular mesenchyme. There are a total of 4 plexi, one in each ventricle. Their function is to secrete CSF which circulates around the brain and the spinal chord in the subarachnoid space which it enters from the fourth ventricle. 17. Know the anomalies associated with the CNS development. Spina bifida cystica – failure of neural arch to form over SC, leaving neural tissues &/or meninges exposed deficits loss of motor function potentially due to mechanical injury in utero or during delivery Spina bifida occulta – failure of bony structure to form no neural deficits but localized hypertrichosis Meningiocele – herniation of the meninges Meningioencephalocele – herniation of part of the brain 3 Meningiohydroencephalocele – herniation of brain and maybe ventricles Anencephaly – due to failure of anterior neural tube closure degeneration of neural tissues Hydrocephalus –abnormal accumulation of CSF due to obstruction of drainage into subarachnoid space, most commonly foramen of Luschka or cerebral aqueduct. Arnold-Chiari malformation – herniation of cerebellar tissue through the foramen magnum, sometimes associated with spina bifida cystica 18. Know the derivatives of the pharyngeal arches, pouches and clefts. ARCH BONES MUSCLES Arch I Maxillary process: maxilla, lat palatine Mm of mastication, process, zygomatic, lat. part of upper myelohyoid, ant. belly of lip, part of temporal. digastric, tensor tympani, Mandibular process: Meckel’s cart., tensor palatine mandible, incus, malleus Arch II Stapes, styloid process of temporal, Stapedius, stylohyoid, post. stylohyoid ligament, Reichert’s cart. belly of digastric, mm of facial lesser horn/upper body of hyoid, expression, zygomaticus Arch III Greater horn/ lower body of hyoid Stylopharyngeus Arch IV Cartilage of the larynx: thyroid, cricoid, arytenoid, corniculate, cuneiform Arch VI ( poorly developed) Cricothyroid Constrictors of pharynx ( swallow) Intrinsic mm of the pharynx (voice production) BLOOD SUPPLY ( mostly regresses ) maxillary arteries, external carotid artery NERVES CN V2 – motor V 1, 2, 3 – sensory (mostly regresses) hyoid arteries, stapedial aa of middle ear Proximal: common & external carotid Distal: proximal internal carotids Lpart of aorta btwn L com carotid & L subclavian Rproximal portion of R subclavian Pulmonary arch L proximal L pulmonary artery; distal ductus arteriosus; Pulmonary arch R proximal R pulmonary artery; distal degenerates CN VII CN IX CN X, Superior laryngeal nerve CN X, recurrent laryngeal PHARYNGEAL POUCHES DERIVATIVES POUCH I Tubotympanic recess – contacts cleft I – between arch I & II Distal portion middle ear ( primitive tympanic cavity ) Proximal portion Eustacian tube POUCH II Invaginates into mesenchyme stroma of palatine tonsil POUCH III 2 wings dorsal wing inferior parathyroid gland ventral wing thymus POUCH IV & V Never distinctly separated, always found together IV superior parathyroid gland V ultimobranchial body incorporated into thyroid parafollicular cells Calcitonin PHARYNGEAL CLEFTS – ( external ) – between Arch I & II First cleft external accoustic meatus – lined with ectoderm Second – fourth cleft cut off from surface by rapid growth of Arch II temporary cervical sinus 19. Remember the anomalies of the heart ASDs PDA – if accompanied by pulmonary stenosis cyanosis as ostium secundum defect: due to faulty septum primum or septum secundum Common atrium – failure of septum primum and secundum Endocardial cushions and AV septal defects – need surgical correction since these contribute to Bi- and Tricuspid valves VSDs Membranous VSD – most common – bulbar ridges start too high Muscular VSD – usually multiple small openings 4 Absence of interventricular septum – failure of muscular septum to form Persistent trunkus arteriosus – no formation of trunkal ridges or aorticopulmonary septum – always w/ VSD Transposition of the great vessels – always w/ VSD, maybe a PDA, failure of aorticopulmonary septum to spiral Coarctation of the aorta Postductal – no problems post-natally Pre-ductal – BIG problems post-natally Double aortic arch – failure of distal right aorta to regress constriction of trachea Tetralogy of Fallot – cono-trunkal region due to unequal division of trunkus 1. Pulmonary stenosis 2. VSD 3. Overriding aorta 4. R ventricular hypertrophy 20. Remember how and where the foramen ovale is formed. The septum primum grows down from the roof of the primordial atrium towards the fusing endocardial cushions. As this septum grows, the foramen primum forms between the free edge and the endocardial cushions. As it gets smaller and smaller the septum primum grows and fuses with the endocardial cushions. Before the foramen primum completely closes, a number of small holes appear that eventually make the foramen secundum within the septum primum. The purpose of the foramen secundum is to ensure the continued blood flow between the left and right atria. The septum secundum grows on the right side of the septum primum. It grows inferiorily, overlaps the foramen secundum in the septum primum. The septum secundum forms an incomplete partition between the atria which results in the foramen ovale. 21. Know the unique characteristics of the fetal circulation and how it changes at birth. Nutrient and O2 rich blood from umbilical vein bypasses liver by way of ductus venosus to inferior vena cava to R atrium. Here most blood goes through foramen ovale into L atrium to L ventricle and from there into the ascending aorta to supply the head, neck, heart, and upper limbs. The blood that stays in the R atrium goes into the R ventricle then up the pulmonary trunk but bypasses the lungs by way of ductus arteriosus to go into the descending aorta to supply the lower body. At birth several changes take place: 1. loss of placenta lowers BP in the inferior vena cava and in the R atrium 2. aeration of lungs lowers pulmonary resistance increases pulmonary blood flow increases BP in L atrium, lowers BP in R atrium 3. closure of foramen ovale 4. closure of ductus arteriosus due to decreased pulmonary and increased systemic resistance 5 22. What is the adult fate of embryonic structures of the heart and vessels; or what is the embryonic origin of adult vessels and chambers of the heart. EMBRYONIC ADULT Umbilical veins ligamentum teres Ductus venosus ligamentum venosus – w/i the liver between the portal vein and inferior vena cava Foramen ovale fossa ovalis Ducuts arteriosus ligamentum arteriosum Umbilical artery medial umbilical ligament EMBRYONIC ARCH I ARCH II ARCH III ARCH IV ARCH VI Dorsal aortae Vitelline arteries Aortic sac Cardinal veins R subcardinal btwn liver & kidney Hepatic vein btwn liver & heart Sub-/supracardinal anastemosis R supracardinal vein ADULT ( arch mostly regresses ) maxillary arteries, external carotid artery ( arch mostly regresses ) hyoid arteries, stapedial aa of middle ear Proximal: common & external carotid Distal: proximal internal carotids Lpart of aorta btwn L com carotid & L subclavian Rproximal portion of R subclavian Pulmonary arch L proximal L pulmonary artery; distal ductus arteriosus; Pulmonary arch R proximal R pulmonary artery; distal degenerates Median sacral artery Distal portion of internal carotids Intersegmental arteries vertebral arteries in neck intercostal arteries in thorax 5th lumbar intersegmentals common iliac aa 7th intersegmental L L subclavian R distal R subclavian branches umbilical arteries fuse with common iliac artery Celiac trunk Superior mesenteric Inferior mesenteric Ascending aorta 2 horns 1. L horn arch of the aorta 2. R horn brachiocephalic trunk Anterior L brachiocephalic vein R anterior cardinal & common cardinal veins superior vena cava Posterior cardinals azygos vein & common iliac veins replaced by: Subcardinals & Supracardinals Inferior vena cava: 4 segments Pre-renal segment Hepatic segment Renal segment Post-renal vein Finally, in your spare time think about all of the tissues and organs you studied in histology and give the embryonic germ layer of origin for each. 6 Bilaminar embryonic disc Hypoblast endoderm of yolk sac extraembryonic mesoderm Epiblast ectoderm of amnion embryonic ectoderm primitive streak extraembryonic mesoderm embryonic mesoderm notochordal process embryonic endoderm 3 germ layers Ectoderm epidermis epidermal derivatives CNS and PNS ( neural plate fold neural tube , neural crest ) pituitary gland sensory epithelia of the eye, ear, and nose ( otic and lens placodes ) Endoderm epithelial lining of gut – 3 regions – foregut, midgut, hindgut epithelial lining of respiratory tract parts of urinary system liver pancreas thyroid parathyroid glands Mesoderm paraxial mesoderm somites skin, bone, muscle intermediate mesoderm kidneys and gonads lateral plate mesoderm somatic / parietal mesoderm lines the body wall splanchnic / visceral mesoderm covers viscera CT muscle circulatory system kidneys gonads 7