Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
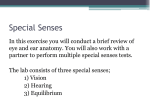
Telecommunications relay service wikipedia , lookup
Olivocochlear system wikipedia , lookup
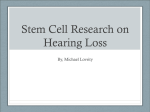
Sound localization wikipedia , lookup
Lip reading wikipedia , lookup
Hearing loss wikipedia , lookup
Auditory system wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
ComD 3700 Basic Audiology Lesson 2 The Human Ear and Simple Tests of Hearing Highlighted information refers to a change between the audio recording (using 10th edition) and the 11th edition of the textbook 1. This is lesson 2, the human ear and simple tests of hearing. We'll discuss the pathways of sound along with different tuning fork tests. These two topic areas will give us a good foundation to move into and begin a discussion of pure tone audiometry and some of the specific elements contained there. Therefore, we'll begin with a discussion on the pathways of sound and move from here into the different tuning fork tests. 2. First, as you observe this slide, note the basic parts of the ear anatomy. Those who of anatomy and physiology of hearing will recognize this. If there is someone in the class who hasn't had that class yet, you won't necessarily recognize this. But you can see the anatomical part of the drawing and should recognize the outer ear or auricle and ear canal. You should remember the outer ear and auricle are part of the outer ear. Then you see the middle ear and continuing to your right, the coiled up cochlea then the nerve to the brain. Now if you would picture a vertical dashed line through the center of the slide. The line divides the middle and outer ear from the cochlea and nerve to the brain. The outer ear and middle ear, we'll call the conductive part of our auditory mechanism because the major function of that part of the anatomy is to conduct sound to the sense organ. The cochlea is the sense organ of hearing. So on the left of the vertical line we have the conductive mechanism and on the right, we have the sensory neural part of our auditory mechanism. We can refine that a bit by looking at the cochlea as the sensory part and the nerve to the brain, the eighth auditory brain as the neural part of the auditory mechanism. That's being combined ... many people speak of that as sensory neural hearing or the sensorineural mechanism. 3. Under normal conditions, on a daily basis from hour to hour, minute to minute we are almost always perceiving sound by way of air conduction. So as I speak to you, as you're listening in your normal environment, and as I listen in my normal environment, we hear by air conduction. This means the sound is generated in the environment around our head and is directed toward our outer ear toward the auricle, the ear canal, strikes the tympanic membrane then sets the middle ear mechanism, the malleus, incus, and stapes, vibratory patterns from the stapes acts on the oval window, which produces that energy into the sense organ or the cochlea. There it is set into neural impulses, which are carried along the eighth nerve to the brain stem and to the cortex and perceived as sound. 4. This slide is similar to the previous slide we looked at in that you see the anatomy of the ear sketched here. The picture isn’t very clear on the slide. But you can use Figure 2.1 on page 18 of your book to get a clear picture. You can find the auricle and the external auditory meatus, the tympanic membrane and if you look closely you can see the middle ear with the malleus, incus and stapes. Then you see the inner ear with the semi circular canals for balance. Below is the cochlea for hearing. You see here the nerve comes off the cochlea and proceeds to the brain. Note there is a slight dashed vertical line coming through the drawing. Up at the top toward the left side, it says conductive mechanism. On the right is the sensorineural mechanism as we discussed previously. So the conductive mechanism and the sensorineural mechanism. In the picture you have this tuning fork, and it's the same one in two positions. The upright tuning fork is outside the auricle. When struck, it sends the signal through the external ear, through the auricle and the eardrum, through the middle ear, to deliver it to the cochlea or the inner ear. Again, we explained that's called air-conducted sound. That is our normal way of hearing in a daily environment, natural way of hearing. We do more air conduction than we do bone conduction. Now you see the other tuning fork which is lying horizontally at the bottom, somewhat. You see in the lower left hand corner bone conduction. This tuning fork is struck then the base is placed on the side of the head. That vibrates the bones of the skull in such a way that the energy from the tuning fork is delivered to the cochlea, bypassing the middle and outer ear. It goes more directly to the cochlea. We have air conducted sound and bone conducted sound. We'll use this principle in diagnosing hearing and talking about different problems with hearing and the ability to diagnose hearing loss. There is another way or mode possible to stimulate the cochlea or organ of hearing and perceive sound. This is by vibrating the bones in the skull or the bones that surround the cochlea or the organ of hearing. This is called bone conduction because of that. In most clinical settings, where testing hearing is being performed, and it's necessary to test a person's hearing of air conduction versus bone conduction, the bone conduction signal is generated by a vibrating object placed on the head. In most clinical environments, this is done with a small plastic vibrating device that is strapped to the side of the head. So it fits just behind the auricle. We'll talk about another way to generate boneconducted signals to the cochlea. We are going to initially use tuning forks to do that. And we will talk about tuning forks later in the lesson. The major point I want you to get here is that if you look at the air conducted signal, the dashed line goes through the entire mechanism where it goes through the outer ear, the middle ear, through the cochlea and from there to the nerve to the brain. On the other hand, if you look at the bone conduction path for stimulating the cochlea, we don't use the outer ear or middle ear. We go to the cochlea to stimulate hearing. This is going to be helpful to us as in an attempt to diagnose hearing loss and particularly the part of the anatomy involved in the hearing loss. Just to summarize quickly here, to stimulate hearing by air conduction, which is our normal way of hearing. Sound waves go through the outer ear, through the middle ear, generate electrical impulses in the cochlea and are sent to the eighth auditory nerve to the brain. In bone conduction stimulation we bypass the outer ear in the hearing test and stimulate the inner ear directly by sending impulses to the cochlea that are sent along the eighth nerve in the brain. 5. Now we are going to discuss the different types of hearing loss. In addition to normal hearing, there are four conditions that define the type of hearing gloss someone has. They are conductive hearing loss, sensorineural hearing loss, mixed hearing loss and nonorganic hearing loss. These are four conditions we're going to discuss extensively throughout this course. So it's very important that you review this material and other materials to get a good concept of these four different conditions. 6. Here we have a busy slide. I wish the print were larger. I put it here only as a reference. You should refer to figure 2.2 in your textbook on page 19 to review the diagram as we are discussing the different types of hearing loss. Again we're talking about pathways of sound. You'll see similarities in this and other slides we've had. If you look at the top, you'll see the vertical line passing from top to bottom, separating boxes on either side. The left side is the conductive mechanism and the right side is sensorineural mechanism. Each box represents a part of the anatomy. If you look at the left hand box, you will see the outer ear. The next box to the right is the middle ear. The next boxes represent the inner ear and the nerve and the brain. We have outer ear, middle ear, inner ear, and the brain. If you look at the top, you will see the first horizontal row of boxes here are going to represent normal hearing. Again, you will see air conduction, AC. You will see the arrow pass through the outer ear, the middle ear, to the inner ear to the nerve and on to the brain. That's the normal way of hearing. You will also see the long darkened arrow before. Bone conduction, BC. Note the arrow does not pass through the outer ear or middle ear but goes right to the inner ear. That's bone conduction. Then of course from the inner ear, the pathway is similar to that of air conduction in the other part of this slide. Let's move down to the next slide and examine this for a moment. You'll notice one of the boxes has slashed lines in it. Those slashed lines represent hearing loss caused by some disorder or defect of the middle ear in this box. A deficit of hearing caused by a disorder in the middle ear. Look over to the left. It's conductive hearing loss. So when our air conduction passes through the outer ear, things are fine. However, as it attempts to pass through the middle ear, it encounters the difficulty or the disorder and therefore, at that point, we would notice a diminished response from a patient. Their hearing would not be normal. Their hearing would be impaired or their conduction impaired if you take this same patient or person and we put the tuning fork or bone conduction vibrating device on their head and stimulates their hearing through the way of bone conduction. You can see the large, long darkened arrow leading directly to the inner ear. It bypasses the outer and middle ear. It is therefore unimpeded and will stimulate the hearing mechanism in a normal fashion by way of bone conduction. So you see normal bone conduction and impaired air conduction add up to a conductive hearing loss because of the conductive mechanism that is impaired. 7. So, some of the defining points of conductive hearing loss are that it involves the breakdown or obstruction of some part of the external or middle ear only. The physical vibrations of sound are no longer transmitted or conducted through air conduction because of the obstruction. Most problems are medically correctable. Physical conduction of sound to sensory organ. Bone conduction test results will be normal 8. Let's move down to the third row on the diagram. Here we have C, this is sensorineural hearing. If we follow our air conduction, we proceed through the outer ear, the middle ear, air, then as we encounter the middle ear, we encounter a deficit in hearing caused by a disorder of the inner ear. So we would have diminished hearing or impaired hearing by air conduction. If we look at our bone conduction mode of hearing, the large darkened arrow going directly to the cochlea, we can see this also has an impairment. You can see the arrow ends at the inner ear and therefore we have the impairment of hearing by bone conduction. So air conduction impairment and bone conduction impairment are about the same in that it signals a sensorineural hearing loss. 9. So to review the information about a sensorineural hearing loss. It results in damage occurring in the inner ear. The damage is to the cochlea and/or VIII Cranial Nerve (CN). It can be further broken down into sensory loss, which involves only the cochlea and neural loss involves only the VIII CN. However, it is usually referred to as combined-sensorineural hearing. With SNHL, testing will reveal the same amount of hearing loss for both air and bone conduction testing. 10. Let's go down to our fourth condition on the diagram, mixed hearing loss. We have an impairment of the middle ear at the same time as we have an impairment of the inner ear. Therefore, we have some conductive and some sensorineural. They are mixed together. However, as we go to the left and proceed through the auditory mechanism, see the impaired air conduction through the outer ear with no problem. We encounter the middle ear and there we encounter some impediment or difficulty with the hearing process. We move on to the inner ear and receive an additional disorder or difficulty. So we have two compounding problems. We have a conductive hearing loss on top of sensory neural hearing loss and therefore the air conduction will be impaired. Look at the bone conduction. Bone conduction bypasses outer and inner ear and goes directly to the inner ear and there encounters a deficit similar to the way it did in the SNHL above. However, the way we know by looking at this is not only is bone and air conduction impaired as it was in the sensorineural hearing loss but air conduction is more impaired than bone conduction so there is a separation between the hearing deficits, air conduction and bone conduction. 11. So, with a mixed hearing loss, you have a combination of conductive and sensorineural hearing loss, occurring simultaneously in the same ear. When you do audiometric testing, the air conduction results will be worse than bone conduction results 12. So in review, by looking at this slide you can see that problems occurring in the red area will result in a conductive hearing loss and an impairment in the blue area is known as a sensorineural hearing loss. If there are problems in both areas, then it is known as a mixed hearing loss. 13. The other type of hearing loss is known as non organic or erroneuos hearing loss. It is not on the diagram or in the picture of the ear because there is nothing wrong with the actual hearing mechanism. Often called a “Functional Loss” and is a result of some sort of psychological cause. There is no known organic cause. There are several types of nonorganic hearing loss: Malingering-Patient willingly & knowingly fabricates a hearing loss for some sort of gain Conversion hysteria-Patient cannot hear, but there is not evidence of organic cause Psychogenic hearing loss-Some psychological disorder that manifests in the symptoms of hearing loss 14. Okay, so now we are going to discuss tuning forks. Tuning fork tests came along long before electronic instrumentation but discussing tuning forks at this point in the course I think is vital. It teaches us a lot about the pathways of sound, normal hearing, hearing loss, conductive neural hearing loss, mixed hearing loss, and there are interesting principles that are involved with the tuning fork tests that come out during these discussions. Hopefully this will help you to understand the principles we will discuss later that are used in modern tests. What we're looking at in this slide is a set of individual tuning forks. Some of you are familiar with tuning forks. For others of you, this is your first exposure to a tuning fork. I'm not sure how to give you an idea of the physical dimensions of one of these tuning forks. I would say if you're looking at the tuning fork in the center, that tuning fork is probably about five inches tall. And so you can get a perspective of how large of an instrument we're talking about. You will note these tuning forks have two tines on them and a base. They are of different sizes and work from the left across to the right. You will notice the lengths of the tines are shorter on the left and longer on the right, thicker on the left and thinner on the right. You will also note the three on the right have an added mass on their tines because that's necessary to accomplish a certain frequency. The sound emitted by each tuning fork is characteristic of the tuning fork. In other words, the tuning fork on your left will produce a high frequency or high hertz tone and the one on your right will produce a low frequency or low hertz pitch. Then you have the spectrum between. From left to right would be high moving lower… lower… lower until you reach the last tuning fork, which would be the lowest frequency. In this lesson we are gong to discuss the more well known tuning forks tests. They are the Schwabach, the Rinne (ri-nay), the Bing, and the Weber. 15. Tuning forks are designed to be struck in a reasonable manner. And when they are struck they will produce the same frequency over and over. Each tuning fork has its own characteristic frequency. It will produce that same frequency each time it's struck. The tuning fork is set into vibration by holding the stem in the hand and striking he tines against a firm but resilient surface such as the rubber heel of a shoe. 16. Let's begin with the Schwabach test. This is a tuning fork test. The Schwabach is rarely used today. I really can't imagine a situation where anyone in the hearing field would use one of these except someone like me standing in front of students to demonstrate this test and how it works and what it's supposed to reveal and try to extract from that certain principles. It's not used, but it presents interesting points in addition to some of the deficiencies of tuning fork testing. The Schwabach is a test that will estimate the patient's hearing by way of bone conduction. The test uses two basic principles. It makes use of the fact that the tone produced by a tuning fork will diminish over time as a result of damping effects. Consider that. This test makes use of the fact that when a tuning fork is struck and a tone produced, if the fork is allowed to sit and vibrate, it will slow and become less and less intense because of resistive or damping effects. Secondly, the patient's hearing is recorded in relative terms to the examiner's hearing. The test compares how long the tone is heard by the patient compared to how long it is heard by the examiner. Many of you are ahead of me. What if the examiner has a hearing loss? That's one of the flaws in this test. If the examiner has a hearing loss and is comparing the patient's hearing to the examiner's hearing, this is a bad flaw in the testing procedure. The assumption the examiner has regular hearing is a reason the Schwabach is rarely used today. However the procedure is to strike and place the tuning fork on the patient's mastoid bone, right behind the auricle. When the patient can no longer hear the tone, the tuning fork is placed on the examiner's ear and timed as to how long he can hear it. 17. The possible outcomes of the Schwabach are: the patient has normal hearing is if the patient hears for the same amount of time as the person doing the testing. If they have a sensorineural hearing loss, they will hear it for a shorter time than the examiner. That should make sense to you. If it's an older person with hearing loss, and they can't hear it as long as the examiner, they probably have a sensorineural hearing loss. That would be called a Schwabach diminished. If the patient hears for a longer time than the examiner this is called the Schwabach prolonged. So a person with a hearing loss, which is conductive, will hear a bone conducted tone for longer. You might say how can they do that if they have a hearing loss and the examiner doesn't? This leads to an important principle: an impairment of the conductive hearing mechanism will enhance one’s bone conducted perception of sound. We normally hear better by air conduction than we do by bone conduction. However, when we have a conductive impairment, that arrangement is changed so that our more perceptive mode of hearing is by conduction. Keep that in mind-if you have a conductive hearing impairment, that would mean a disorder of the outer or inner ear, then your bone conduction perception is enhanced even beyond a normal listener. 18. Let's talk about the Rinne test, the tuning fork test for a moment. To understand this test, you have to understand certain principles. The test compares hearing by air conduction to hearing by bone conduction. We stay on one side of the head with the tuning fork and compare that ear, the hearing by air conduction in that ear, and the hearing by bone conduction in the same ear. Normally, without disorders, the hearing mechanism is more sensitive by air conduction than by bone conduction. Remember that. This air conduction advantage is lost whenever there's a conductive hearing loss. So the tuning fork will sound louder by bone conduction than by air conduction. And remember when we say the tuning fork will sound louder, it is because it is being delivered by way of bone conduction, placing the tuning fork on the skull or bone of the head. Whenever there's a conductive disorder, it influences bone perception. To perform a Rinne test, the fork is struck and alternately placed on the mastoid bone and at the opening of the ear canal. The patient is asked if the tone is louder with the mastoid placement or ear canal placement. If you have a conduction hearing loss, the patient will report the tone being more intense with the mastoid placement than the air conduction placement. And if you have normal or sensorineural hearing loss, then the patient may report the tone being more intense via air conduction than bone conduction. Masking must be placed in the non-test ear to make sure the tone is being heard in the test ear. We must put noise or masking sound in the non-test ear so it cannot perceive a tone crossing from the test ear. In that way, we've isolated the test ear and hopefully we've done this correctly and made the test ear secure for our test. 19. The results of the Rinne are: Rinne positive is when the fork is heard louder at the ear canal and this indicates either normal hearing acuity or a sensory neural hearing loss. A Rinne negative is when the fork is heard louder at the mastoid and indicates a conductive hearing loss. A false negative Rinne is when there was not sufficient mask and the test tone crossed the head and was heard in the non-test ear. That's a false negative because the non-test ear participated and shouldn't have. That's what makes it a false negative. 20. The next tuning fork test, the Bing, takes advantage of the occlusion effect. The occlusion effect like it's stated here when the ear, the conductive mechanism, outer, or middle ear, causes the ear to become occluded. Occlusion occurs when the ear canal is obstructed but the occlusion effect can extend to having the middle ear disordered. But think more of the ear canal and having it occluded. This enhances the bone conduction. That should make sense because you occlude the ear you get a disorder. Remember conductive disorder enhance bone conduction. Recall when the ear canal is occluded hearing loss is present. There is an enhanced perception tone when delivered to the ear, the inner ear, via bone conduction. With normal or sensory hearing, they will hear the tone from the tuning fork better when the examiner occludes the outer ear by pushing on the tragus, therefore occluding the outer ear. On the other hand, if the person has a conductive hearing loss, pressing and releasing the tragus will not affect a change in the patient's perception of the tone. 21. So therefore, the examiner asks the patient many times as I press and release on the side of your ear, do you hear an enhanced or a warbling effect on the tone? If they do hear a warbling or a heightened and lowered intensity, they probably have a sensorineural or normal hearing, this is known as a positive Bing. If they do not hear a change in the tone from occluded to nonoccluded, they probably have an effected hearing loss, which is known as a negative Bing. 22. Now we have the Weber test. It's one of the simpler tests to administer and probably has the least amount of problems that it could encounter to distort the result. The Weber test is used to tell whether a unilateral hearing loss is conductive or sensorineural. We're talking unilateral, one sided hearing loss. Here, it is a test of lateralization because the patient is asked to indicate from which direction the sound seems to be coming. In other words, when the patient comes in, the patient is asked which is your worst ear. The patient has to tell you which it is. You have to have the knowledge before you proceed. 23. So, the testing procedure is to have the patient indicates which ear is poorer and which better. The tuning fork is then placed on the forehead. The patient is asked where they hear the tone. If the tone is heard in the better ear, then the poorer ear must be a sensorineural hearing loss. If the tone is heard in the poor ear, and this seems contradictory to our senses, but it's true. If the tone is heard in the poorer ear, that ear must have a conductive hearing loss. In conclusion, tuning fork tests are nowhere near as accurate, qualitative, or quantitative as audiometric testing. We discuss them here to help us understand certain principles as to the pathways of hearing and the nature of certain types of hearing loss. I hope this has opened some thought processes, given us a chance to talk about conductive pathways, air conduction pathways, and bone conduction pathways, and some the different of hearing losses like conductive and sensorineural and started us to thinking in the area of hearing loss because that's going to be the nature of this course is to describe tests and the test results and the implications of those results.