Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
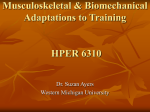
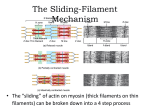
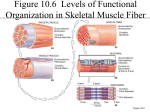
AANA Journal Course 6 Update for Nurse Anesthetists Residual Neuromuscular Blockade Anna L. Plummer-Roberts, MSN, CRNA Christina Trost, MSN, CRNA Shawn Collins, DNP, PhD, CRNA Ian Hewer, MSN, MA, CRNA This article provides an update on residual neuromuscular blockade for nurse anesthetists. The neuromuscular junction, pharmacology for producing and reversing neuromuscular blockade, monitoring sites and methods, and patient implications relating to incomplete reversal of neuromuscular blockade are reviewed. Overall recommendations include using Objectives At the completion of this course, the reader should be able to: 1.Identify the anatomy and physiology of acetylcholine and nicotinic acetylcholine receptors. 2.Describe the method of action of neuromuscular blocking drugs. 3.Describe the available methods for monitoring recovery from neuromuscular blockade. 4.Discuss the options available to reverse neuromuscular blockade and the optimal timing of reversal. 5.List postoperative implications of residual neuromuscular blockade. Introduction Contemporary anesthesia often requires the use of muscle relaxation for surgical exposure or manipulation of a patient’s airway. If using muscle relaxation, it is important for anesthesia providers to monitor and reverse neuromuscular blockade to ensure that the patient has regained complete neuromuscular function by the end of surgery. Interestingly, a high percentage of anesthesia providers both internationally and in the United States do not monitor neuromuscular recovery and do not use pharmacologic reversal.1 In an evaluation of factors influencing morbidity and mortality in the first 24 hours postoperatively, a tenfold increase in death or coma was associated with the absence of reversal medications.2 multiple settings when employing a peripheral nerve stimulator for monitoring return of neuromuscular function and administering pharmacologic reversal when the train-of-four ratio is below 0.9. Keywords: Neuromuscular blockade, peripheral nerve stimulator, residual neuromuscular blockade. Despite the potential side effects associated with neuromuscular blockade reversal, the potential for serious and life-threatening respiratory complications in the postanesthesia care unit (PACU) warrants the use of a neuromuscular monitoring device and pharmacologic reversal as a standard of care to ensure patient safety. Anatomy and Physiology of Neuromuscular Junction To understand the relationship between skeletal muscle contraction and neuromuscular blockade, some discussion of the physiology is necessary. Acetylcholine (ACh) is the neurotransmitter responsible for communication between the peripheral nervous system and the skeletal muscles. The ACh molecule comprises 1 acetate and 1 choline molecule packaged together in the presynaptic neuron and then stored as ACh in vesicles called quanta. When a signal is propagated, hundreds of quanta spill thousands of ACh molecules out of the presynaptic neuron and into the synaptic cleft. The ACh molecules traverse the neuromuscular junction and bind to nicotinic acetylcholine receptors (nAChRs) on the postsynaptic neuron. These nAChRs are found in a functional area on the postsynaptic motor neuron called the motor end plate (Figure). The nAChR is pentameric and composed of 2 α-subunits, and 1 each of β, δ, and ε-subunits. The α-subunits are the binding sites for ACh. For ACh to cause AANA Journal Course No. 35: AANA Journal course will consist of 6 successive articles, each with an objective for the reader and sources for additional reading. This educational activity is being presented with the understanding that any conflict of interest on behalf of the planners and presenters has been reported by the author(s). Also, there is no mention of off-label use for drugs or products. Please visit AANALearn.com for information about when the corresponding exam questions for this article will be available. www.aana.com/aanajournalonline AANA Journal February 2016 Vol. 84, No. 1 57 Figure. Neuromuscular Junction Reproduced with permission from Barash P, Cullen BF. Clinical Anesthesia. 7th ed. Riverwoods, IL: Wolters Kluwer Health; 2013. Nondepolarizing muscle relaxants Amino steroids Benzylisoquinolines Depolarizing muscle relaxants (–“curoniums”) (–“curiums”) Succinylcholine (ultrashort acting) Rocuronium (intermediate acting) Mivacurium (short acting) Vecuronium (intermediate acting) Cisatracurium (intermediate acting) Pancuronium (long acting) Table 1. Common Pharmacologic Muscle Relaxants the ligand-gated sodium ion (Na+) channels to open, ACh must occupy both α subunits. This initiates a depolarization of the motor unit and signals release of calcium ions (Ca2+) from the sarcoplasmic reticulum, which allows actin and myosin to interact within the myofibrils of the muscle, causing a skeletal muscle contraction. Also present on the motor end plate are thousands of acetylcholinesterase molecules, the enzyme responsible for the dissociation of ACh back into its constituents of acetate and choline. These are inactive constituents and are taken back into the presynaptic cell and repackaged into ACh, where they are almost immediately available for the next muscle contraction. Neuromuscular Blocking Drugs Neuromuscular blocking drugs can be classified based on mechanism of action or duration of action. When classified based on mechanism of action, there are 2 groups: depolarizing muscle relaxants and nondepolarizing muscle relaxants (NDMRs; Table 1). When classified based on duration of action, there are 3 groups: short acting (5-20 minutes), intermediate acting (20-55 minutes), and long acting (60 minutes and longer; see Table 1).3 Muscle relaxants are large molecules with a positively charged quaternary ammonium group that is attracted to the negatively charged nAChR. Depolarizing muscle relaxants, such as succinylcholine, compete with ACh 58 AANA Journal February 2016 Vol. 84, No. 1 to agonize the nAChR. Similar to ACh, succinylcholine binds to both α-subunits, causing the motor end plate to depolarize. The succinylcholine molecule is composed of 2 linked ACh molecules but differs from ACh in its resistance to degradation by acetylcholinesterase. During initial depolarization by succinylcholine, the muscle fiber undergoes repetitive excitation known as fasciculations, followed by a rest period where no excitation occurs, which results in paralysis. In the presence of normal physiology, succinylcholine generally does not cause postoperative weakness, because of its ultrashort duration, and is therefore rarely implicated in residual neuromuscular blockade (RNMB). There are 2 broad categories of NDMRs: benzylisoquinolines and amino steroids. Unlike the endogenous ligand (ACh) and the depolarizer (succinylcholine), NDMRs competitively antagonize the nAChR by binding to only one α-subunit.4 By antagonizing this receptor, the motor end plate cannot depolarize and the muscle cannot contract, resulting in paralysis. Monitoring Sites of Interest and Nerve Stimulation A few types of neuromuscular blockade monitoring devices warrant discussion, as well as their monitoring sites, modes of stimulation, and methods for interpretation. Muscle relaxants affect muscles of the body differ- www.aana.com/aanajournalonline Mode Frequency, Hz Single twitch Train-of-four Double burst stimulation Tetany Duration 0.1-1 2 50 50, 100, or 200 Pattern 0.2 ms 0.2 ms 4 twitches at 500-ms intervals 0.2 ms2-3 twitches followed by 750-ms pause; repeat 2-3 twitches 5s Table 2. Peripheral Nerve Stimulator Settings3,7 ently based on anatomical characteristics (eg, density of nAChR on motor end plate). The most common sites for neuromuscular monitoring are the ulnar nerve with resultant adductor pollicis muscular contraction (adduction of the thumb), temporal branch of the facial nerve with resultant corrugator supercilii contraction (eyebrow twitch), zygomatic branch of the facial nerve with resultant orbicularis oculi contraction (eyelid squint), and posterior tibial nerve with resultant flexor hallucis brevis contraction (plantar flexion of great toe). Again, because these muscles are paralyzed and recover from paralysis at varying times, the site of interest to the anesthesia provider can change (eg, during intubation vs during surgical relaxation), or clinical judgment may be necessary to interpret levels of muscle paralysis. For example, the more central nerves (eg, facial nerve) are paralyzed faster and recover more quickly than peripheral nerves (eg, ulnar nerve).5,6 Thus, the corrugator supercilii may show complete recovery from neuromuscular blockade, whereas the adductor pollicis shows incomplete recovery. This requires clinical judgment to evaluate the amount and timing of pharmacologic reversal. The peripheral nerve stimulator (PNS) is the most common neuromuscular stimulating device in clinical practice and is a qualitative monitoring tool. Electrodes on the skin attached to the PNS supply current to the nerve, causing muscle contraction. This is often colloquially termed twitching. Current, supplied in milliamperes, has a direct relationship with the muscle contraction. The more current applied to the nerve, the more muscle fibers innervated by that nerve contraction.7 This is partly what leads to the qualitative interpretation of the twitch. The PNS also employs frequency, which is measured in hertz or cycles per second, and duration in milliseconds.7 The PNS requires the user to select a mode—single twitch, train-of-four (TOF), double burst stimulation, or tetany—and then to interpret the response. Response interpretation can be accomplished by either visualizing the muscle contraction (if a direct visual can be obtained) or feeling the muscle contract using a hand lightly placed on the muscle. This leads to the inherent subjectivity and variability between providers using the PNS. There is evidence that tactile assessment may be slightly more accurate in detecting residual blockade than visual assessment.7,8 There are slight variations between manufacturers, but the settings can be simplified7 (Table 2). Single twitch operates at a frequency of 0.1 to 1 Hz with a 0.2-millisecond twitch duration. This mode has limited clinical use. The TOF employs 4 twitches at 2 Hz of 0.2 milliseconds in duration. The advantage of this setting is that it allows for a baseline, for example, comparing twitch number 4 (T4) to twitch number 1 (T1). The twitch “depression” of T4 compared with T1 is interpreted as the TOF ratio (TOFR). For example, if T4 is half the twitch strength of T1, then the TOFR equals 0.5. This twitch depression is what anesthetists have come to know as “fade.” Clinical data support that when the TOFR exceeds 0.4, anesthesia providers have trouble assessing the presence of fade, which is a limitation of TOF mode. Double burst stimulation is essentially 2 or 3 bursts at 50 Hz, followed by a 750-millisecond pause followed by the initial burst pattern. Double burst stimulation allows detection of fade at a TOFR at 0.6 to 0.7, which is most likely because of the provider’s ability to better assess differences between 2 stimuli instead of 4.8 Tetany uses a frequency of 50, 100, or 200 Hz for 5 seconds, which can also assess fade, although it is intensely painful in a semi-awake patient. Tetany also produces a posttetanic facilitation in which a neuromuscular response is elicited more easily.9,10 This may indicate more recovery than has actually occurred. Posttetanic count is not a formal mode but can assess levels of deeper blockade. Posttetanic count uses tetany followed by TOF at frequency of 1 Hz. The provider counts the posttetanic TOF twitches (with no attention to fade). The number of posttetanic count twitches is inversely related to time until the first regular (without tetany) TOF twitch returns. There is some argument among authorities as to the best test for detecting RNMB. Laboratory work suggests that mechanomyography (MMG) is the gold standard for assessing neuromuscular blockade because it quantitatively measures the force of muscle contraction.3,7 However, MMG is not useful in the clinical setting because of bulky equipment and the need for controlled variables such as muscle temperature.7 In clinical use, it is easier for clinicians to assess fade with double burst stimulation vs TOF, but 100-Hz tetanus over 5 seconds appears to be the most sensitive test for assessing RNMB.10-12 Although this is the most sensitive method, it has shortcomings (eg, painful for an emerging patient) and thus cannot be used in every situation. www.aana.com/aanajournalonline AANA Journal February 2016 Vol. 84, No. 1 59 Assessment Devicemodality Advantages Small, portable, common in practice Disadvantages PNS Uses current, multiple modes MMG Measures force of muscle Gold standard, no user interpretation contraction Bulky, difficult to set up, affected by temperature AMG Measures acceleration of muscle response Susceptible to artifact due to movement Converts to numerical ratio, inexpensive, easy to use Requires user interpretation KMG Measures bend in sensor Multiple modes corresponding to muscle contraction May inaccurately assess recovery from paralysis EMG Measures electrical activity Equipment is less bulky, requires less space Affected by temperature and positioning, needs multiple electrodes, requires calibration Table 3. Neuromuscular Blockade Monitoring Devices7 Abbreviations: AMG, acceleromyography; EMG, electromyography; KMG, kinemyography; MMG, mechanomyography; PNS, peripheral nerve stimulator. There are several quantitative methods of assessing neuromuscular blockade, including acceleromyography (AMG), kinemyography (KMG), electromyography (EMG), and MMG (Table 3).7 All these methods use the ulnar nerve and adductor pollicis muscle (ie, thumb twitch). These methods are more reliable than qualitative methods. However, all have notable disadvantages. Ultimately, no current method guarantees complete detection of RNMB. Acceleromyography measures the acceleration of a muscle response and converts it to a ratio.7 For example, rather than the anesthesia provider using the TOF mode and assessing response, the AMG displays a TOFR based on the conversion of acceleration. In some models, the TOFR can exceed 1.0, and in others it does not, leading to some confusion for interpretation. In clinical practice, the displayed value is susceptible to artifact during patient movement. Kinemyography measures the amount of bend in a sensor when the muscle is stimulated. Sensors on the thumb and forefinger are responsible for interpreting the bend. It has single twitch, double burst stimulation, and TOF modes but may be less useful than MMG in determining recovery.7 Electromyography measures electrical activity in the nerve being stimulated. It does not require the arm preparation that AMG needs, but its major disadvantage is that measured electrical activity is influenced by temperature, which is difficult to keep constant on an extremity even during short surgeries in a cold operating room. Mechanomyography converts the force of muscle contraction to correspond to twitch height, tetany, and TOFR. Like EMG, muscle temperature affects results, and thus it is rarely used clinically. Although PNS and tools for myography, including AMG, KMG, EMG, and MMG, are useful in the patient under general anesthesia, other methods are useful in an awake patient. These methods are flawed by subjectivity 60 AANA Journal February 2016 Vol. 84, No. 1 Drug Onset, min Duration of action, min Edrophonium 5-10 Neostigmine 5-15 30-60 45-90 Pyridostigmine 10-20 60-120 Table 4. Common Cholinesterase Inhibitors3 as well. The most potentially useful test is the patient’s ability to sustain a forceful bite, although the timing of this test is limited to after extubation. This demonstrates the strength of the masseter muscle and is associated with a TOFR of 0.86.10 As will soon be discussed, the gold standard for adequate recovery is a TOFR greater than 0.9. The traditional 5-second head lift can be successfully performed with a TOFR of 0.5 and thus is not an appropriate measure of full reversal.8 Analysis of current evidence reveals that no clinically used test of neuromuscular function can reliably exclude the presence of residual paralysis less TOFR less than 0.9.8 Reversal of Neuromuscular Blockade Until recently, the only methods of reversing neuromuscular blockade available in the United States were acetylcholinesterase inhibitors (AChIs): neostigmine, edrophonium, and pyridostigmine (Table 4).3 These agents work on acetylcholinesterase, the enzyme that breaks down ACh. By inhibiting this breakdown, the lifespan of ACh increases as well as the concentration available for action at the neuromuscular junction.3 The increased quantity of ACh outcompetes any NDMR remaining in the neuromuscular junction, and the recovery of skeletal muscle begins. There is a clinical ceiling effect of AChIs when 100% of acetylcholinesterase has been inhibited, termed maximal inhibition. At maximal inhibition, additional doses of AChIs will not improve recovery and could lead to paradoxical muscle weakness.13 The resultant muscle www.aana.com/aanajournalonline weakness may be due to desensitization of ACh receptors leading to transmission failure, a depolarization block or open channel block.13 This effect can be seen at clinically used doses of neostigmine, 0.04 to 0.07 mg/kg.10 The use of high-dose neostigmine, above 0.06 mg/kg, has been associated with a threefold increase in the risk of postoperative atelectasis, longer time to PACU discharge readiness, and longer postoperative hospital stay.14 The researchers theorized that these effects could be due to neostigmine being used in a patient who has complete, spontaneous recovery from NDMR, resulting in a depolarizing block or an incomplete reversal from a profound neuromuscular blockade.14 The clinical ceiling effect also limits the ability of AChIs to reverse profound neuromuscular blockade when the concentration of NDMR is high at the neuromuscular junction, such as that corresponding to a TOFR less than 0.2.15 Use of AChIs to achieve adequate recovery to a TOFR greater than 0.9 can only occur if endogenous recovery at the neuromuscular junction has already begun. Research has shown that achieving the gold standard of a TOFR greater than 0.9 within 10 minutes of neostigmine delivery from any degree of paralysis during a volatile-based anesthetic is not an achievable goal.16 Pharmacologic reversal with neostigmine paired with glycopyrrolate following muscle relaxation by cisatracurium or rocuronium from a TOF of 2/4 with tactile assessment at the adductor pollicis required an average of 15 minutes to obtain a TOFR of 0.9 or greater; some patients had residual block (TOFR < 0.9) even at 30 minutes.17 Kim and colleagues18 found that time from reversal to a TOFR greater than 0.9 took significantly longer periods of time in sevoflurane-based anesthetic vs propofol-based anesthetic, demonstrating that volatile anesthetics can alter the effective onset time of AChIs. They also found that reversal to a TOFR greater than 0.9 occurred from 2 tactile TOF counts in the propofol-based group, on average, in 10 minutes. In contrast, from 4 tactile TOF counts the sevoflurane group took 15 minutes to obtain a TOFR greater than 0.9 in 95% of patients. From 2 tactile TOF counts it took the sevoflurane group an average of 22 minutes to achieve a TOFR greater than 0.9. Current recommendations include waiting until 4 tactile TOF counts are visible at the adductor pollicis before administering reversal medication; this will allow for adequate spontaneous recovery and optimization of AChIs action while allowing approximately 20 minutes after a reversal agent is given to obtain a TOF greater than 0.9.8,10,15 Aside from nicotinic ACh receptors on skeletal muscles, ACh can stimulate muscarinic ACh receptors on sites such as the heart, lungs, and gastrointestinal tract. Systemic increases in ACh (due to administration of AChI) can lead to adverse effects such as bradycardia, arrhythmias, hypotension, bronchoconstriction, hypersalivation, diarrhea, and increased gastric secretions.19 These adverse parasympathetic effects can be prevented with simultaneous administration of an antimuscarinic drug (either atropine or glycopyrrolate), which acts by blocking muscarinic ACh receptors. Because the antimuscarinic drug prevents the ill effects of the AChI, it is important that the anesthetist selects drugs with similar onset time and duration of action. Glycopyrrolate is best paired with neostigmine, whereas atropine is best paired with edrophonium. Anesthesia providers cite AChIs’ muscarinic effects on the gastrointestinal tract (eg, increased motility and stimulation of gastric secretions and acid) as a cause for increased incidence of postoperative nausea and vomiting.20 A meta-analysis by Cheng et al21 in 2005 found that neostigmine paired with an antimuscarinic was not associated with an increase in the risk of postoperative vomiting. Insufficient evidence was found to make a conclusion about postoperative nausea. Interestingly, they found a significant decrease in postoperative vomiting when atropine was used vs glycopyrrolate. The authors theorized that the effect of atropine was due to its ability to cross the blood-brain barrier and exert central effects. Plagued with muscarinic side effects, AChIs are no longer the only method of pharmaceutical reversal of neuromuscular blockade available. Following the recent FDA decision sugammadex is now available to providers in the United States, as well as the United Kingdom, Europe, and Asia. Sugammadex is the first of a new class of medications called selective relaxant binding agents, available to reverse neuromuscular blockade. Its method of action is to selectively encapsulate neuromuscular blocking drugs by forming tight water-soluble complexes. It encapsulates the amino steroids (eg, rocuronium, vecuronium, pancuronium), thus rendering them unable to antagonize the nAChR. These complexes are then excreted intact via urine.3 The 2 primary advantages of sugammadex are the rapid speed of skeletal muscle recovery (it can reverse any level of blockade when dosed appropriately within 3 minutes3) and the lack of muscarinic adverse effects.22 The proposed disadvantages of sugammadex are rare allergic reactions and short-term transient alterations to prothrombin time.12 Sugammadex has been used in Europe since 2008, but as noted, has only recently become available in the United States. It has potential to revolutionize the reversal of neuromuscular blockade, but owing to its recent introduction, is beyond the scope of this article to analyze fully. It should be noted that numerous factors, including anesthetic management and patient characteristics, might influence the ability of the anesthetist to achieve a timely reversal. Some of these factors include increased levels of inhalation agent, hypothermia, age, and metabolic imbalances.18,19 www.aana.com/aanajournalonline AANA Journal February 2016 Vol. 84, No. 1 61 Residual Neuromuscular Blockade •Definition. To be able to understand the full implications of RNMB, we first must define what RNMB is and establish how often it occurs in patients undergoing general anesthesia. In 1975 RNMB was defined as a TOFR less than 0.7 based on a pulmonary function test in healthy awake volunteers.23 The study subjects were able to maintain normal vital capacity, inspiratory force, and expiratory force with a TOFR of 0.7 or greater. Donati12 concluded that “the recommended target of 0.7 for adequate neuromuscular recovery had to be revised when several groups provided evidence that swallowing, protection from aspiration, ability to clench teeth, and genioglossus activity were considerably depressed at a TOFR of 0.7 and that near-normal function was not present until TOFR reached 0.9.” Normal pulmonary function can be maintained at a TOFR of 0.7 because of the diaphragm’s relative resistance to the effects of NDMR. This resistance leads to less blockade at the diaphragm and a quicker recovery than for peripheral muscles such as the adductor pollicis.5 This results in adequate spontaneous respiration, whereas the TOF is suppressed and pharyngeal function is still impaired. A precurarization dose of NDMR, which is a smaller dose of approximately 10% of the required intubating dose used to speed the onset of the intubating dose, has long been known to reduce the TOFR to as low as 0.64.24 A TOFR of 0.85 has been associated with general discomfort, malaise, ptosis, and blurred vision following a precurarization dose of vecuronium, pancuronium, or atracurium.24,25 The current accepted standard of RNMB is a TOFR less than 0.9. This is based primarily on recovery of laryngeal function. Muscles of the upper airway involved in swallowing and airway protection are sensitive to small amounts of residual block.26 After muscle paralysis with vecuronium and measurement at the adductor pollicis, a TOFR of 0.8 was associated with significantly decreased end-inspiratory upper airway volumes, and pharyngeal function normalized at a TOFR greater than 0.9.27 These authors concluded that partial paralysis at a TOFR of 0.5 and 0.8 leads to partial upper airway obstruction due to weakness of the upper airway dilator muscles.28 Another factor influencing the adjustment upward of the standard for RNMB is impairment of the hypoxic ventilatory drive at small amounts of residual paralysis (eg, TOFR = 0.7), likely due to reduced nerve discharge from carotid body chemoreceptors caused by NDMR.6,29 Hypoxic ventilatory drive has been shown to recover fully with a TOFR greater than 0.9.26 Recent evidence supporting the underestimation of RNMB by anesthesia providers showed a belief that clinically significant RNMB occurred less than 1% of the time.1 This is at odds with historical and recent docu- 62 AANA Journal February 2016 Vol. 84, No. 1 mented rates of RNMB. In the late 1970s when RNMB was defined as TOFR less than 0.7, RNMB was documented to be occurring in 42% of patients arriving in the PACU.30 A reanalysis of the same data adjusting for a TOFR less than 0.9 shows the incidence of RNMB at that time to be 72%.12 A more recent meta-analysis found the average rate of RNMB was 41%31 with RNMB defined as a TOFR less than 0.9. Debaene et al22 showed a similar rate (ie, 45% of patients) of RNMB at admission to the PACU after a single intubating dose (2 times the effective dose required to reduce twitch height by 95%, or ED95) of an intermediateacting NDMR. They also found that 2 hours after administration of the NDMR, 37% patients displayed a TOFR less than 0.9 with no reversal given. Intermediate-acting NDMRs have a duration of action of 30 to 60 minutes.3 An intubating dose of rocuronium has been shown to have a duration of action of 30 to 90 minutes.3 Yet 2 hours after an intubating dose of intermediate-acting NDMR, 37% of patients still had some degree of RNMB. Textbook-cited drug duration times do not guarantee full return of neuromuscular function, and clinically significant RNMB can occur after the proposed duration. There is controversy regarding the role neuromuscular monitoring devices play in the prevention of RNMB. Some of this controversy is due to the lack of clarity in the available research. A meta-analysis of neuromuscular monitoring and RNMB concluded that the use of intraoperative neuromuscular monitoring devices is not associated with a decrease in the incidence of residual paralysis.31 However, the authors suspect the findings may be due to poor quality and design of studies included in the analysis. The findings emphasize that merely monitoring neuromuscular blockade does ensure adequate recovery; in fact, at a TOFR above 0.9, patients can still have residual paralysis, and a clinically appropriate dose of reversal should still be warranted even if recovery appears adequate. In a more recent study, researchers found less incidence of RNMB with quantitative monitoring (AMG) compared with qualitative monitoring (PNS).32 At arrival to the PACU, 14.5% of patients monitored with AMG exhibited RNMB, whereas 50% of patients monitored with PNS exhibited RNMB. The patients monitored with AMG had fewer symptoms of residual paralysis than did patients monitored with PNS. The use of qualitative TOF assessment did not decrease the risk of postoperative respiratory complications and reintubation.33 Aside from impaired respiratory ability, which is of utmost concern for the anesthetist, RNMB manifests in numerous other signs of muscle weakness. A study of healthy volunteers receiving an infusion of mivacurium to obtain a TOFR of 0.7 via PNS at the adductor pollicis reported diplopia, difficulty with visual tracking, difficulty swallowing, flat facial expression, and facial muscle weakness.34 www.aana.com/aanajournalonline Murphy and colleagues32 found that symptoms of muscle weakness are predictive of the presence or absence of a TOFR less than 0.9. Patients’ subjective feelings of muscle weakness were considered symptoms of RNMB. They included the level of perceived difficulty in completing 11 clinical signs of muscle weakness (normal vs impaired), blurry vision, double vision, facial weakness, facial numbness, and general weakness. The most common signs and symptoms at admission to the PACU were generalized weakness, patient-reported difficulty completing 5-second eye opening, difficulty visually tracking and speaking, and blurry vision. These findings are indicative of ocular and pharyngeal muscle sensitivity to RNMB. The most commonly reported symptom in patients with a TOFR greater than 0.9 was difficulty visually tracking.35 All patients with a TOFR less than 0.9 had at least 1 symptom at admission to the PACU, with a median of 7 symptoms. Of the 80% of patients exceeding a TOFR of 0.9, all had at least 1 symptom of RNMB at admission to PACU, with a median of 2 symptoms.35 Interestingly, even after 1 hour in the PACU, 83% of patients who had a TOFR less than 0.9 at admission retained symptoms of residual paralysis. In terms of clinical tests of RNMB (eg, 5-second head lift), it appears that these measurements correlate with a TOFR of 0.6 to 0.7 and are therefore poor indicators of TOFR less than 0.9.32 These clinical tests include 5-second head lift, 5-second hand grip, 5-second eye opening, 5-second tongue protrusion, tongue depressor test, ability to smile, ability to swallow, ability to speak, ability to cough, ability to visually track objects, and ability to breathe easily. The median number of failed clinical tests observed in all patients, despite their level of RNMB, was zero.32 •Postoperative Implications of Residual Neuromuscular Blockade. Numerous large retrospective studies have noted an association between the use of NDMR, residual paralysis, and adverse postoperative outcomes.2,26,33,36 Overall, critical respiratory events occur between 0.8% and 6.9% after extubation in the PACU.33,36 Critical respiratory events include upper airway obstruction, hypoxia, hypoxemia, signs of respiratory failure, inability to breathe deeply when instructed, evidence or suspicion of postextubation aspiration, and reintubation. The most frequently seen critical respiratory events in the first 15 minutes in the PACU are severe hypoxemia (pulse-oximeter saturation < 90%), upper airway obstruction, and mild hypoxia (oxygen saturation, 90%-93%).36 Multiple critical respiratory events may occur concomitantly in the same patient.36 In a study by Murphy et al36 90.5% of patients who experienced a critical respiratory event had a TOFR less than 0.9 as measured by AMG. In patients needing reintubation, researchers found a reintubation rate of 0.8%33 occurring an average of 2.5 days postoperatively. Grosse-Sundrup et al33 concluded that the use of intermediate-acting NDMR is associated with increased risk of postoperative reintubation, requiring admission to the intensive care unit. When intermediate-acting NDMRs are used for surgeries less than 120 minutes, the risk of reintubation is even higher. Interestingly, the researchers found that the use of neostigmine increased the risk of severe postoperative respiratory failure, most likely because of inappropriate use of neostigmine leading to paradoxical neuromuscular blockade. In an evaluation of factors influencing morbidity and mortality in the first 24 hours postoperatively, a tenfold increase in death or coma was associated with the absence of reversal medications.2 The time spent by patients with RNMB in the PACU can be significantly longer than patients who had adequate reversal of neuromuscular blockade. Butterly et al37 documented that patient discharge time from the PACU is, on average, 75 minutes longer for patients with RNMB. These researchers also found that the independent risk factors associated with a longer PACU stay were age and RNMB.37 •Patient Satisfaction. Healthcare reform is increasingly linking reimbursement for services with patient satisfaction. Although it has not yet been determined how anesthesia reimbursement will be influenced, patient satisfaction is always an area for concern. Patients’ perception of the quality of their recovery has been found to be more positive with AMG neuromuscular monitoring vs PNS. Patients ranked overall quality of recovery based on a 0 to 100 visual analog scale.32 The quality was ranked higher in the AMG group, who also had significantly less RNMB.32 In global quality of recovery, measured on the www.aana.com/aanajournalonline AANA Journal •The longer the duration of action of NDMR used, the greater the frequency of residual paralysis. •If rocuronium or vecuronium was used, sugammadex may be used for moderate or deep muscle relaxation in adult (including elderly) patients and reversal of rocuroniuminduced moderate muscle relaxation in pediatric patients (aged 2-17 years). •If not using sugammadex, before paralytic reversal, allow some degree of spontaneous recovery, ideally a TOFR > 0.9. •Merely monitoring neuromuscular blockade does ensure adequate recovery; in fact, at a TOFR > 0.9, patients can still have residual paralysis, and a clinically appropriate dose of reversal should still be warranted even if recovery “seems” adequate. •Patients monitored with AMG have fewer symptoms of residual paralysis than do patients monitored with PNS. •If using a PNS, gather information from multiple modes. A reduced reversal dose seems clinically prudent even if the TOFR appears > 0.9. Table 5. Recommendations Abbreviations: AMG, acceleromyography; NDMR, nondepolarizing muscle relaxants; PNS, peripheral nerve stimulator; TOFR, train-offour ratio. February 2016 Vol. 84, No. 1 63 quality of recovery (QoR)-9 scoring system,38 the groups differed in one category, with the AMG group having a higher score in general well-being. Conclusion Residual neuromuscular blockade is a complex and dynamic issue. Because of shortcomings associated with neuromuscular monitoring tools and differing recovery rates based on physiology, interpreting patient recovery can be difficult. Current literature outlines some of the issues that contribute to RNMB and the complications that are associated with it. Understanding the complexity of these issues can lead to increased patient safety. Based on current literature, our recommendations are presented in Table 5. REFERENCES 1. Naguib M, Kopman AF, Lien CA, Hunter JM, Lopez A, Brull SJ. A survey of current management of neuromuscular block in the United States and Europe. Anesth Analg. 2010;111(1):110-119. 2. Arbous MS, Meursing AEE, van Kleef JW, et al. Impact of anesthesia management characteristics on severe morbidity and mortality. Anesthesiology. 2005;102(2):257-268. 3. Nagelhout J. Neuromuscular blocking agents reversal agents, and their monitoring. In: Nagelhout J, Plaus K, eds. Nurse Anesthesia. 5th ed. St Louis, MO: Saunders; 2014:158-185. 4. Naguib MLC, Meistelman C. Pharmacology of neuromuscular blocking drugs. In: Miller RD, ed. Miller’s Anesthesia. 8th ed. Philadelphia, PA: Churchill Livingstone/Elsevier; 2015:958-994. 5. Donati F, Meistelman C, Plaud B. Vecuronium neuromuscular blockade at the diaphragm, orbicularis oculi and adductor pollicis muscles. Can J Anaesth. 1991;37(4 pt 2):S13-S13. 16. Kirkegaard H, Heier T, Caldwell JE. Efficacy of tactile-guided reversal from cisatracurium-induced neuromuscular block. Anesthesiology. 2002;96(1):45-50. 17. Kopman AF, Kopman DJ, Ng J, Zank LM. Antagonism of profound cisatracurium and rocuronium block: the role of objective assessment of neuromuscular function. J Clin Anesth. 2005;17(1):30-35. 18. Kim KS, Cheong MA, Lee HJ, Lee JM. Tactile assessment for the reversibility of rocuronium-induced neuromuscular blockade during propofol or sevoflurane anesthesia. Anesth Analg. 2004;99(4):1080-1085. 19.Nagelhout JJ, Welliver MD. Reversal of neuromuscular blocking agents: current practice. AANA J. 2013(suppl):8-11. 20. Tramèr MR, Fuchs-Buder T. Omitting antagonism of neuromuscular block: effect on postoperative nausea and vomiting and risk of residual paralysis: a systematic review. Br J Anaesth. 1999;82(3):379-386. 21. Cheng C-R, Sessler DI, Apfel CC. Does neostigmine administration produce a clinically important increase in postoperative nausea and vomiting? Anesth Analg. 2005;101(5):1349-1355. 22. Debaene B, Plaud B, Dilly MP, Donati F. Residual paralysis in the PACU after a single intubating dose of nondepolarizing muscle relaxant with an intermediate duration of action. Anesthesiology. 2003;98(5):1042-1048. 23. Ali HH, Wilson RS, Savarese JJ, Kitz RJ. The effect of tubocurarine on indirectly elicited train-of-four muscle response and respiratory measurements in humans. Br J Anaesth. 1975;47(5):570-574. 24. Engbaek J, Howardy-Hansen P, Ôrding H, Viby-Mogensen J. Precurarization with vecuronium and pancuronium in awake healthy volunteers: the influence on neuromuscular transmission and pulmonary function. Acta Anaesthesiol Scand. 1985;29(1):117-120. 25. Howardy-Hansen P, Moller J, Hansen B. Pretreatment with atracurium: the influence on neuromuscular transmission and pulmonary function. Acta Anaesthesiol Scand. 1987;31(7):642-644. 26.Murphy GS, Brull SJ. Residual neuromuscular block: lessons unlearned. Part I: definitions, incidence, and adverse physiologic effects of residual neuromuscular block. Anesth Analg. 2010;111(1):120-128. 6. Murphy GS BH, Eriksson LI, Miller RD. Reversal (antagonism) of neuromuscular blockade. In: Miller RD, ed. Miller’s Anesthesia. 8th ed. Philadelphia, PA: Churchill Livingstone/Elsevier; 2015:995-1027. 27. Eriksson LI, Sundman E, Olsson R, et al. Functional assessment of the pharynx at rest and during swallowing in partially paralyzed humans: simultaneous videomanometry and mechanomyography of awake human volunteers. Anesthesiology. 1997;87(5):1035-1043. 7. Dorsch JA, Dorsch SE. Understanding Anesthesia Equipment. 5th ed. Philadelphia PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008:805-827. 28. Eikermann M, Vogt FM, Herbstreit F, et al. The predisposition to inspiratory upper airway collapse during partial neuromuscular blockade. Am J Respir Crit Care Med. 2007;175(1):9-15. 8.Brull SJ, Murphy GS. Residual neuromuscular block: lessons unlearned. Part II: methods to reduce the risk of residual weakness. Anesth Analg. 2010;111(1):129-140. 29. Eriksson LI, Sato M, Severinghaus JW. Effect of a vecuronium-induced partial neuromuscular block on hypoxic ventilatory response. Anesthesiology. 1993;78(4):693-699. 9. Brull SJ, Connelly NR, O’Connor TZ, Silverman DG. Effect of tetanus on subsequent neuromuscular monitoring in patients receiving vecuronium. Anesthesiology. 1991;74(1):64-70. 30. Viby-Mogensen J, Jørgensen BC, Ording H. Residual curarization in the recovery room. Anesthesiology. 1979;50(6):539-541. 10. Plaud B, Debaene B, Donati F, Marty J. Residual paralysis after emergence from anesthesia. Anesthesiology. 2010;112(4):1013-1022. 31. Naguib M, Kopman AF, Ensor JE. Neuromuscular monitoring and postoperative residual curarisation: a meta-analysis. Br J Anaesth. 2007;98(3):302-316. 11. Baurain MJ, Hennart DA, Godschalx A, et al. Visual evaluation of residual curarization in anesthetized patients using one hundredhertz, five-second tetanic stimulation at the adductor pollicis muscle. Anesth Analg. 1998;87(1):185-189. 32. Murphy GS, Szokol JW, Avram MJ, et al. Intraoperative acceleromyography monitoring reduces symptoms of muscle weakness and improves quality of recovery in the early postoperative period. Anesthesiology. 2011;115(5):946-954. 12. Donati F. Residual paralysis: a real problem or did we invent a new disease? Can J Anaesth. 2013;60(7):714-729. 33. Grosse-Sundrup M, Henneman JP, Sandberg WS, et al. Intermediate acting non-depolarizing neuromuscular blocking agents and risk of postoperative respiratory complications: prospective propensity score matched cohort study. Br J Anaesth. 2012;345:e6329. 13. Eikermann M, Fassbender P, Malhotra A, et al. Unwarranted administration of acetylcholinesterase inhibitors can impair genioglossus and diaphragm muscle function. Anesthesiology. 2007;107(4):621-629. 14. Sasaki N, Meyer MJ, Malviya SA, et al. Effects of neostigmine reversal of nondepolarizing neuromuscular blocking agents on postoperative respiratory outcomes: a prospective study. Anesthesiology. 2014;121(5):959-968. 15. Brull SJ, Kopman AF, Naguib M. Management principles to reduce the risk of residual neuromuscular blockade. Curr Anesthesiol Rep. 2013;3:13-138. 64 AANA Journal February 2016 Vol. 84, No. 1 34. Kopman AF, Yee PS, Neuman GG. Relationship of the train-of-four fade ratio to clinical signs and symptoms of residual paralysis in awake volunteers. Anesthesiology. 1997;86(4):765-771. 35. Murphy GS, Szokol JW, Avram MJ, et al. Postoperative residual neuromuscular blockade is associated with impaired clinical recovery. Anesth Analg. 2013;117(1):133-141. 36. Murphy GS, Szokol JW, Marymont JH, Greenberg SB, Avram MJ, Vender JS. Residual neuromuscular blockade and critical respiratory events in www.aana.com/aanajournalonline the postanesthesia care unit. Anesth Analg. 2008;107(1):130-137. 37.Butterly A, Bittner EA, George E, Sandberg WS, Eikermann M, Schmidt U. Postoperative residual curarization from intermediate-acting neuromuscular blocking agents delays recovery room discharge. Br J Anaesth. 2010;105(3):304-309. 38. Myles PS, Hunt JO, Nightingale CE, et al. Development and psychometric testing of a quality of recovery score after general anesthesia and surgery in adults. Anesth Analg. 1999;88(1):83-90. 39. Hibbs RE, Zambon AC. Agents acting at the neuromuscular junction and autonomic ganglia. In: Brunton LL (ed). Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. New York, NY: McGraw-Hill; 2011:254-276. thetist in High Point, North Carolina, and was a student at Western Carolina University, Asheville, North Carolina, at the time this article was written. Christina Trost, MSN, CRNA, is a Certified Registered Nurse Anesthetist in Royal Oak, Michigan, and was a student at Western Carolina University, Asheville, North Carolina, at the time this article was written. Shawn Collins, DNP, PhD, CRNA, is the program director of Western Carolina University Nurse Anesthesia Program, Asheville, North Carolina. Ian Hewer, MSN, MA, CRNA, is the assistant program director of Western Carolina University Nurse Anesthesia Program, Asheville, North Carolina. DISCLOSURES Anna L. Plummer-Roberts, MSN, CRNA, is a Certified Registered Nurse Anes- The authors have declared no financial relationships with any commercial interest related to the content of this activity. The authors did not discuss off-label use within the article. www.aana.com/aanajournalonline AANA Journal AUTHORS February 2016 Vol. 84, No. 1 65