Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
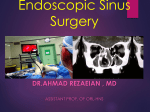
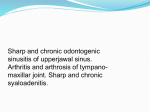
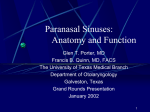
The ethmoid bone: clinical imaging anatomy from an embryological point of view Poster No.: C-2208 Congress: ECR 2013 Type: Educational Exhibit Authors: T. Hiyama, M. Shiigai, T. Masumoto, M. Minami; Tsukuba, Ibaraki/ JP Keywords: Education and training, Congenital, Normal variants, Education, CT, Head and neck, Anatomy DOI: 10.1594/ecr2013/C-2208 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 74 Learning objectives To explain imaging anatomy of the ethmoid bone from an embryological point of view. This exhibit will be shown according to the next content list (Table 1). Table 1: Table of contents. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Images for this section: Page 2 of 74 Table 1: Table of contents. Page 3 of 74 Background The ethmoid bone is centrally located in the paranasal sinuses, affecting drainage pathways from the frontal and maxillary sinuses (ostiomeatal complex). It contains the ethmoid air cells, which play an important role in olfactory sensation, humidification, ventilation, and phonation. The ethmoid bone consists of 4 parts: the perpendicular plate, cribriform plate, and 2 ethmoidal labyrinths (Fig 1). Because it forms the medial wall of the orbit and floor of the anterior cranial fossa, inflammation or trauma, including endoscopic surgery, may invade these adjacent structures. An understanding of the complex anatomy of the ethmoid bone is therefore crucial for radiologic diagnosis of paranasal pathology and planning of functional endoscopic sinus surgery. Fig. 1: Ethmoid bone. The ethmoid bone is a cuboidal structure with some prominences, forming the boundary of the orbit laterally and anterior cranial fossa superiorly. It has 4 main parts: the perpendicular plate, cribriform plate, and 2 ethmoidal labyrinths.Other prominent structures include the uncinate process, middle turbinate, superior turbinate, and crista galli. References: Michael Schunke, ES. PROMETHEUS LernAtras der Anatomie. First Japanease edition ed. 2009: Thieme. This exhibit illustrates the radiological normal anatomy and variants of the ethmoid bone from an embryological point of view, specifically addressing the 5 basal-lamellae concept and migration of air cells. Page 4 of 74 Images for this section: Fig. 1: Ethmoid bone. The ethmoid bone is a cuboidal structure with some prominences, forming the boundary of the orbit laterally and anterior cranial fossa superiorly. It has 4 main parts: the perpendicular plate, cribriform plate, and 2 ethmoidal labyrinths.Other prominent structures include the uncinate process, middle turbinate, superior turbinate, and crista galli. Page 5 of 74 Imaging findings OR Procedure details I. Embryology A. Embryology Ethmoturbinals, the origin of the basal lamellae, arise at the lateral wall of the nasal cavity. Development continues up to the seventh month of the gestation with regression thereafter until birth. Four to 5 ethmoturbinals eventually remain as the uncinate process, ethmoid bulla, middle turbinate, superior turbinate, and supreme turbinate (Fig 2)[1]. The ethmoturbinal is divided into an ascending portion, descending portion, and genu, which is angle between ascending and descending portions. The nasal meatus is similarly divided into the ascending and descending portions and the genu (Figs 3, 4)[2]. The ascending portion of the middle meatus (or recessus superior) develops into the hiatus semilunaris and frontal sinus. The descending portion (or recessus inferior) develops into infundibulum and the maxillary sinus (Fig 3)[3]. Development of the ascending portion is rudimentary, except for the middle turbinate and middle meatus. The ethmoid air cells develop from the descending portion. Fig. 2: Lateral aspect of nasal cavity. This schematic diagram (a) shows 5 ethmoturbinals which develop into 1) the uncinate process, 2) ethmoid bulla, 3) middle turbinate, 4) superior turbinate, and 5) supreme turbinate (b). References: Howard Levine, MC. Sinus Surgery: Endoscopic and Microscopic Approaches. 2004: Thieme. Michael Schunke, ES. PROMETHEUS LernAtras der Anatomie. First Japanease edition ed. 2009: Thieme. Page 6 of 74 Fig. 3: Coronal section of the nasal sinus, 12 weeks gestation. Ascending portion of the middle meatus (*) develops into frontal recess and frontal sinus. The descending portion (**) develops into infundibulum and maxillary sinus. (Uncinate process [UP], ethmoid bulla [EB], middle turbinate [MT]) References: Mizukoshi, O. Clinical Otorhinolaryngology and Head and Neck Surgery. Vol. 6A. 1989. Page 7 of 74 Fig. 4: Ascending and descending portions of the middle turbinate, lateral aspect of nasal cavity, and coronal section. Ethmoturbinal is divided into lamina basilaris (red dotted line) and lamina recurvata (blue line). The lamina basilaris forms part of the lateral wall attachment. The lamina recurvata is more medial with a curled configuration. The lamina basilaris separates the draining pathway. The genu is the angle between the ascending and descending portions (yellow line). The other portion of ethmoturbinals show similar development. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP B. The 5 basal-lamellae concept Seydel divided the ethmoturbinals into "Basallamelle" and "Einrollungen", which are named as the lamina basilaris (basal lamellae) and lamina recurvata by Killian, respectively (Fig 4)[4]. The lamina basilaris forms part of the attachment of the ethmoturbinals to the lateral wall of the nasal cavity. The lamina recurvata is a medially protruding structure with a rolling configuration. The uncinate process and ethmoid bulla are mainly derived from the basal lamella and lamina recurvata does not develop well [1]. In addition to the middle and superior turbinates, the uncinate process and ethmoid bulla are derived from the ethmoturbinals, leading Killian to establish the concept of at least 4 basal lamellae, 5 if the supreme turbinate is included [5]. The basal lamellae demarcate the anatomical pathways of sinus drainage. C. Ethmoid anatomy from an embryological point of view Ethmoid air cells can grow in any direction and invade adjacent bones [6]. This migration of ethmoid cells, in addition to the 5 basal-lamellae concept, is the key to understanding ethmoid anatomy. The first basal lamella develops into the uncinate process and the agger nasi cells, derived from pneumatization of the anterior portion of the first basal lamella. The second basal lamella is also pneumatized and is called the ethmoid bulla. The frontal recess and ethmoid infundibulum open into the middle meatus between the uncinate process (the first basal lamella) and ethmoid bulla (the second basal lamella). The embryology of the ostiomeatal complex explains its anatomy. The frontal sinus and maxillary sinus originate from the ascending and descending portions of nasal meatus, which continue to the middle meatus between the first and second basal lamellae (Fig 3). The ethmoid bulla drains into the hiatus semilunaris superior located between the second and third basal lamellae. The third basal lamella divides ethmoid air cells into anterior and posterior ethmoid cells, and the fourth basal lamella separates posterior ethmoid air cells into posterior and postreme cells (Fig 5). Page 8 of 74 Fig. 5: Ethmoid anatomy: The 5 basal-lamellae concept. The basal lamellae (blue arrows) separate the draining pathways (red arrows). The frontal and maxillary sinuses drain into the middle meatus via the frontal recess and hiatus semilunaris between the first (agger nasi cells and uncinate process) and second (ethmoid bulla) basal lamellae. The hiatus semilunaris superior opens between the second and third lamellae (middle turbinate). The third basal lamella separates the anterior and posterior ethmoid cells. The fourth basal lamella (superior turbinate) divides the posterior and postreme meatus. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Pneumatization around the ethmoid bulla is called the suprabullar cells, frontal bullar cells, and sinus lateralis (suprabullar recess and retrobullar recess). The infraorbital, or Haller, cells and supraorbital ethmoid cells represent invasive pneumatization of the floor or roof of orbit respectively. Anterior ethmoid cells may invade the interfrontal sinus septa and crista galli, and posterior air cells may extend to the turbinate (concha bullosa) or above the sphenoid sinus (Onodi cells) (Fig 6). Page 9 of 74 The ethmoid air cells are classified into intramural and extramural based on migration into or out of the ethmoid bone. Extramural cells contain Haller cells, frontal cells, supraorbital ethmoid cells, interfrontal sinus septal cell, and Onodi cells [6, 7]. Fig. 6: Migration of ethmoid cells. Agger nasi cells (AN) and ethmoid bulla (EB) are derived from pneumatization of the first and second basal lamellae. Agger nasi cells are the most anterior air cells and can invade uncinate process. The frontal cells, located above the agger nasi cells, form the anterior wall of the frontal recess. Additional anterior ethmoid cells are located around the ethmoid bulla (suprabullar recess, suprabullar cells, frontal bullar cells, and retrobullar recess) or orbital wall (supraorbital ethmoid cells, and Haller cells). Anterior ethmoid cells can extend to interfrontal sinus septa and crista galli. Posteriorly, they may extend to the turbinate (concha bullosa) or above the sphenoid sinus (Onodi cells). (Air cells around agger nasi cells [blue], ethmoid bulla [red], posterior air cells [yellow]) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP II. Bone anatomy and variants A. Bone anatomy and variants derived from the 5 basal lamellae 1. Uncinate process and agger nasi cells a) Uncinate process The uncinate process is derived from the first basal lamella. It forms the boundaries of the hiatus semilunaris and the ethmoid infundibulum. The uncinate process has many anatomical variants, some of which may obstruct the ethmoid infundibulum: Page 10 of 74 • • • Medially bent uncinate process may cause obstruction because of contact with the middle turbinate (Fig 7). Elongated or enlarged uncinate process (Fig 8) Pneumatized uncinate process believed to represent an extension of agger nasi cells (Fig 9) [8]. Fig. 7: Medially bent uncinate process. The uncinate process is bent medially, contacting the middle turbinate and occluding the infundibulum (red arrow). Mucus drains through the accessory foramen (yellow arrow). In this case, mucosal thickening is caused by dental caries (blue arrow). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 11 of 74 Fig. 8: Elongated or enlarged uncinate processes. This patient presented with left maxillary sinusitis. An elongated or enlarged uncinate process (red arrow in b) was found after cleaning of the nasal cavity. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Fig. 9: Pneumatized uncinate process. Pneumatized uncinate process (red arrow) is believed to represent extension of agger nasi cells. In this case, the agger nasi cell extends to the uncinate process (yellow arrow, c). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Attachment variants Page 12 of 74 Attachment of the uncinate process is important for surgery and sinus pathology, as it allows determination of whether the frontal sinus drains into or laterally to the ethmoid infundibulum. The uncinate process may be attached to: • • • Lamina papyracea or agger nasi (lamina terminalis). The frontal recess opens directly into middle meatus. The lamina terminalis is the blind pouch between the uncinate process and lamina papyracea (Figs 10a,b)[9]. Skull base or middle turbinate. The frontal recess drains into the ethmoid infundibulum (Figs 10c, d, 11)[9]. Orbital floor or inferior aspect of the lamina papyracea (silent sinus syndrome, atelectatic uncinate process). This variant is associated with hypoplastic, ipsilateral maxillary sinus secondary to closure of the infundibulum. Enophthalmos may result from the inferior retraction of the orbital wall [8]. Page 13 of 74 Fig. 10: Four different attachments of the uncinate process. When the uncinate process attaches to ethmoid bulla or lamina papyracea (red arrows, a and b), the frontal recess opens directly into middle meatus. When the attachment is at the skull base or middle turbinate (red arrows, c and d), the frontal recess opens into the ethmoid infundibulum. Yellow dotted line shows drainage pathway. (Lamina terminalis (*)) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 14 of 74 Fig. 11: Uncinate process attachment to the middle turbinate (red arrows). Anterior to posterior coronal CT images of the same patient as Fig 10d. In this condition, frontal recess opens into the ethmoid infundibulum.(yellow dots). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP b) Agger nasi cells The agger nasi cells, from the Latin agger meaning small mound, are the most anterior air cells (Fig 12). They are derived from pneumatization of the anterior part of the first basal lamella [8]. The agger nasi cells are located anterior to the uncinate process and Page 15 of 74 posteromedial to the lacrimal sac (Fig 12d) and may invade the lacrimal bone. The agger nasi is an important surgical landmark. Fig. 12: Agger nasi cells. Agger nasi cells (green arrows) are the most anterior of the ethmoid cells. The agger nasi cells drain to the middle nasal meatus (orange arrows).The agger nasi cells are located posteromedial to the lacrimal sac and are the anatomical landmark for this sac during surgery. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP 2. Ethmoid bulla Page 16 of 74 The ethmoid bulla is derived from pneumatization of the second basal lamella (Fig 13). It lacks a distinct posterior wall and therefore is not a separate cell but rather a bony lamella with an air space behind it [10]. The ethmoid bulla is the largest and most consistent anterior ethmoid cell, and constitutes a reliable anatomical landmark. The degree of pneumatization is variable. Giant ethmoid bulla may cause obstruction of the ostiomeatal complex. The term torus lateralis designates the second basal lamella that is not pneumatized (Fig 14)[11]. Fig. 13: Ethmoid bulla. The ethmoid bulla (EB) is located in the anterior air cells and is usually the largest cell. EB is formed by pneumatization of the second basal lamella. (Agger nasi cell [AN], uncinate process [UP], sinus lateralis [SL], frontal recess [FR]) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 17 of 74 Fig. 14: Torus lateralis. The torus lateralis (green arrows) represents an ethmoid bulla without pnenumatization. (Agger nasi cell [AN]) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP 3. Middle turbinate The middle turbinate, derived from the third lamella, separates the ethmoid cells into the anterior and posterior ethmoid cells. The anterior ethmoid cells drain into the middle meatus, while the posterior ethmoid cells drain into the superior meatus. The insertion of the middle turbinate can be divided into 3 parts. The first or vertical part lies in the anterior one-third of the middle turbinate, oriented in the sagittal plane. In this part, the middle turbinate attaches to the cribriform plate. The second or oblique part attaches to the basal lamella or lamina papyracea. The third or horizontal part lies horizontally in the posterior one-third of the middle turbinate. In this part, the middle turbinate attaches to the perpendicular plate of the palatine bone (Fig 15). These attachments provide stability to the middle turbinate. The middle turbinate has many variants. • • • Concha bullosa: This aerated turbinate may be the site of inflammatory processes ranging from simple mucosal thickening to a mucocele (Fig 16)[12]. Paradoxical middle turbinate: A paradoxical middle turbinate is formed by the inverse curling of the middle turbinate. This variant is not associated with sinus pathology (Fig 17a)[13]. Turbinate sinus: A curved middle turbinate may curl upon itself to form an internal concavity, called a turbinate sinus (Fig 17b). Other variants include medial and lateral displacement, lateral bending, L-shaped configuration, and sagittal transverse clefts [14]. Page 18 of 74 Fig. 15: Attachment of the middle turbinate. The insertion of the middle turbinate can be divided into 3 parts. The first or vertical part attaches to the cribriform plate. The second or oblique part attaches to the basal lamella or lamina papyracea. The third or horizontal part attaches to the perpendicular plate of the palatine bone. These attachments help to stabilize the middle turbinate. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 19 of 74 Fig. 16: Concha bullosa. Concha bullosa of the middle turbinate in 2 different patients. Concha bullosa in patient 1 showing pneumatization of the middle turbinate (a, b). Concha bullosa may be the site of inflammatory disease ranging from simple mucosal thickening to mucocele (c, d). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 20 of 74 Fig. 17: Paradoxical middle turbinate (a) and turbinate sinus (b). Paradoxical middle turbinate is formed by the inverse curling of middle turbinate and direct lateral convexity of the bone toward the lateral sinus wall. Turbinate sinus (red arrows, b) is formed by the concavity of the curled segment. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP 4. Superior turbinate The superior turbinate is derived from the fourth lamella. Concha bullosa may coexist and cause headache (Fig 18) [15]. Page 21 of 74 Fig. 18: Concha bullosa of the superior turbinate. Concha bullosa may occur in the superior turbinate, a structure derived from the fourth lamella. This variant may cause headache. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP 5. Supreme turbinate The supreme turbinate is usually rudimentary. B. Bone anatomy and variants derived from other important structures 1. Ethmoid roof Page 22 of 74 The ethmoid roof protects the anterior cranial fossa during surgery. It consists of fovea, crista galli, lateral lamella, and cribriform plate (Fig 19). Foveal angle, measured between the fovea and the lamina papyracea, is an index for determining the risk of operation (Fig 20a, b). A low-sloping fovea predisposes to a risk of anterior cranial penetration. Asymmetry of the ethmoid roof also increases the risk of penetration into the anterior cranial fossa (Fig 20c). The lateral lamella is one of the critical structures for surgery. The depth of the olfactory pit was classified by Kero as follows (Fig 21) [16]: Type 1: 1-3 mm Type 2: 4-7 mm Type 3: 8-16 mm The cribriform plate and lateral lamella are thin structures that are easily broken. Dehiscence or congenital defect may also occur, associated with spontaneous cerebrospinal fluid rhinorrhea (Fig 22) [17]. Fig. 19: Ethmoid roof. The ethmoid roof consists of fovea, crista galli, lateral lamella, and cribriform plate. Cribriform plate is a thin structure that may be dehiscent or defective. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 23 of 74 Fig. 20: Foveal angle (a, b) and asymmetry of the ethmoid roof (c). Foveal angle is the angle between the fovea and lamina papyracea. A low sloping fovea predisposes to anterior cranial penetration during surgery. Differences in height between the right and left fovea are also significant for surgery. The ethmoid roof is lower and high sloping on the right side (arrow) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 24 of 74 Fig. 21: Kero's classification: Type 1 (a), Type 2 (b), and Type3 (c). Kero's classification is based on the depth of the olfactory pit. In the type 3 in particular, the ethmoid roof is significantly higher than the anterior cranial fossa, increasing the surgical risk. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 25 of 74 Fig. 22: Spontaneous cerebral fluid leakage from the left cribriform plate. Cribriform plate calcification is obscure on the left side (a). STIR sequences show fluid continuous to the subarachnoid space (red arrow, b). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP 2. Lamina papyracea The lamina papyracea is a thin structure in which dehiscence may be seen, most often at the insertion of the basal lamella (Fig 23)[18]. Associated bulging of the orbital contents poses a risk for surgery. Fig. 23: Dehiscence of the lamina papyracea with medial herniation of orbital fat. Bony dehiscence occurs most often at the insertion of the basal lamella. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 26 of 74 3. Ethmoid foramen Injury to the anterior ethmoidal artery during endoscopic procedures may cause intracranial or orbital hematoma, and preoperative assessment of this artery is essential to avoid complications. The ethmoid artery runs through the ethmoid foramen. The ethmoid foramen may be located using the medial notch of the orbit and anterior ethmoidal sulcus as a landmark on the CT images (Fig 24)[19]. Injury to the posterior ethmoid artery, located 10-12 mm behind anterior ethmoid foramen, is less common. Page 27 of 74 Fig. 24: Anterior and posterior ethmoid foramina. The medial notch of the orbit is a useful landmark for identifying the ethmoid foramen. The posterior ethmoid artery is located 10-12 mm behind anterior ethmoid foramen. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP III. Air cell anatomy and variants The ethmoid sinuses arise from the endochondral bone. This origin results in remarkably thin bony contours with irregular and morphologically unique borders [6]. Pneumatization is variable, limited only by the presence of hard bone. A. Anterior ethmoid air cells 1. Intramural cells a) Sinus lateralis (the lateral sinus of Grunwald, suprabullar recess, and retrobullar recess) The sinus lateralis, also called the suprabullar or retrobullar recesses, is located superior and posterior to the ethmoid bulla (Fig 25). The sinus lateralis can extend dorsally, far posterior and inferior between the ethmoid bulla and the basal lamella of the middle turbinate, opening into a space known as the hiatus semilunaris superior. The ethmoid bulla usually opens into a well-pneumatized sinus lateralis. If the ethmoid bulla does not extend to the skull base, the sinus lateralis may continue anteriorly into the frontal recess (Fig 25c)[20]. The suprabullar and retrobullar recesses can also be approached medially and inferiorly through the hiatus semilunaris superior. Page 28 of 74 Fig. 25: Sinus lateralis (the lateral sinus of Grunwald, suprabullar recess, and retrobullar recess). The sinus lateralis(retrobullar recess, red dotted line, b-d) is the space between the ethmoid bulla (EB) and the third basal lamella (yellow dotted line). When ethmoid bulla dose not extend to the roof, the sinus lateralis continues to frontal recess (suprabullar recess, blue dotted line, c). The ethmoid bulla opens posteriorly into lateral recess (** in b). (Agger nasi cell [AN],suprabullar cell [*]) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP b) Suprabullar cells and frontal bullar cells The suprabullar and frontal bullar cells are located above the ethmoid bulla (Figs 26, 27). The suprabullar cells do not protrude into the frontal sinus, in contrast to the frontal bullar cells, which extend to the frontal sinus. The frontal recess may be narrow between the agger nasi and suprabullar or frontal bullar cells. The suprabullar and frontal cells are equivalent to the suprabullar recess, which appears as a cleft above the ethmoid bulla Page 29 of 74 during endoscopy. The prevalence of suprabullar and frontal cells is approximately 8% and 10%, respectively [21]. Fig. 26: Suprabullar and frontal bullar cells. Suprabullar cells (Fig a, b *) do not extend to the frontal sinus in contrast to frontal bullar cells (Fig c, d **). The frontal recess may be narrow between the agger nasi cells (AN) and suprabullar or frontal bullar cells (b). (Ethmoid bulla [EB]) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 30 of 74 Fig. 27: Inflammation of the frontal bullar cells. Frontal bullar cells are opacified (*). The frontal sinus is clear because the frontal recess is not involved. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP c) Pneumatization of the crista galli Pneumatization of the crista galli may communicate with the frontal recess (Fig 28). Obstruction of ostium causes chronic sinusitis or mucocele formation within the crista galli [22]. Recognition of this variant is important to avoid extension into anterior cranial fossa during surgery. Page 31 of 74 Fig. 28: Pneumatization of the crista galli. Anterior ethmoid cells extending to the crista galli. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP 2. Extramural cells a) Haller cells#infraorbital cells# Page 32 of 74 Haller cells, first identified by Haller in 1765, extend to the medial roof of the maxillary sinus, inserted between the lamina papyracea and the uncinate process below the ethmoid bulla (Fig 29). Haller cells may contribute to the narrowing of the infundibulum[23]. Fig. 29: Haller cells. Haller cells (red arrow) are located at the medial floor of the maxillary sinus below the ethmoid bulla (EB). When small, they may be similar appearance to the infraorbital canal (c, d). Due to their location next to the infundibulum, Haller cells may obstruct sinus drainage. (Uncinate process [*] posterior ethmoid cell [PC] Infraorbital canal [yellow arrow]) References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 33 of 74 b) Frontal cells Frontal cells are anterior ethmoid cells located above the agger nasi cells that may obstruct the frontal recess. Bent and Kuhn classify frontal cells into 4 different types (Fig 30)[21, 24]. Type 1: Single cell, not extending into the frontal sinus (24.2%) Type 2: Two or more cells, sometimes extending to the inferior frontal sinus (4.2%) Type 3: Single cell, extending into the frontal sinus (3.1%) Type 4: Isolated cells located in the frontal sinus (0.0%) Fig. 30: Frontal cells: Type 1 (a, b), Type 2 (c, d), and Type 3 (e, f). Frontal cells (*) are located above the agger nasi cells (AN). Frontal cells form the anterior wall of the drainage pathway from the frontal sinus (yellow dotted line), and encroach on the frontal recess or frontal sinus. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP c) Supraorbital ethmoid cell Page 34 of 74 The supraorbital ethmoid cell extends behind the frontal sinus through the orbital plate of the frontal bone (Fig 31). It simulates a septated frontal sinus (Fig 32). The supraorbital ethmoid cell can compromise frontal sinus drainage. During endoscopic surgery, it may be mistaken for the frontal sinus. Fig. 31: Supraorbital ethmoid cells. The supraorbital ethmoid cell (*) extend to the orbital plate of the frontal bone. The anterior ethmoid foramen (red arrows) is easily identified by pneumatization of the supraorbital ethmoid cell. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 35 of 74 Fig. 32: Mucocele of the supraorbital ethmoid cell. Left ethmoid mucocele (*) is bulging into orbital fossa. On the axial slices of the CT (b, c), supraorbital cell (*) are easily mistaken for frontal sinus (**). In this case frontal sinus and frontal recess (yellow dotted line and red arrow) are intact. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP d) Interfrontal sinus septal cell The interfrontal sinus septal cell is located in the interfrontal septa (Fig 33). This variant may cause inflammation and mucocele [14]. Page 36 of 74 Fig. 33: Interfrontal sinus septal cell. The interfrontal sinus septal cell (*) is located between the frontal sinuses. This cell drains into frontal recess (red dotted line). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP B. Posterior ethmoid air cells 1. Intramural cells a) Posterior, postreme ethmoid cells Posterior and postreme ethmoid cells drain into the superior meatus and may extend above the maxillary sinus (Fig 34). The fourth basal lamella divides the posterior ethmoid group of cells into posterior and postreme ethmoid cells. Page 37 of 74 Fig. 34: Posterior ethmoid cell (PC) and postreme ethmoid cell (PSC) The superior nasal turbinate (fourth basal lamella; yellow arrows in a, b) separates the posterior and postreme ethmoid cells. Posterior ethmoid cell can invade into the roof of the maxillary sinus behind the Haller cell (c, d). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP 2. Extramural cells a) Onodi cells (sphenoethmoidal cells) Onodi cells, also known as sphenoethmoidal cells, are postreme ethmoid cells which extend above the sphenoid sinus (Fig 35). Onodi cells are intimately related to the optic nerve and internal carotid artery. Onodi cells could be mistaken for the sphenoid sinus during endoscopic surgery. Mucocele or fungal sinusitis of Onodi cells may cause visual disturbance (Fig 36). Page 38 of 74 Fig. 35: Onodi cells. Onodi cells (OC), or sphenoethmoidal cells, represent invasion of the postreme ethmoid cells above the sphenoid sinus. These cells can contact the optic nerve (a, b) and internal carotid artery(c). Pneumatization may extend to the anterior clinoid process (*). References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Page 39 of 74 Fig. 36: Aspergillosis of the Onodi cell. Aspergillosis of the Onodi cell in a 60-yearold man with right visual disturbance. Right Onodi cell (*) invades the anterior clinoid process, with local inflammation (yellow arrows) involving the right optic nerve. As part of the ethmoid sinus, this structure should not be confused with the sphenoid sinus (**). Aspergillus was identified in the specimen postsurgery. References: Department of Radiology, University of Tsukuba - Tsukuba, Ibaraki/JP Images for this section: Page 40 of 74 Fig. 2: Lateral aspect of nasal cavity. This schematic diagram (a) shows 5 ethmoturbinals which develop into 1) the uncinate process, 2) ethmoid bulla, 3) middle turbinate, 4) superior turbinate, and 5) supreme turbinate (b). Fig. 3: Coronal section of the nasal sinus, 12 weeks gestation. Ascending portion of the middle meatus (*) develops into frontal recess and frontal sinus. The descending portion Page 41 of 74 (**) develops into infundibulum and maxillary sinus. (Uncinate process [UP], ethmoid bulla [EB], middle turbinate [MT]) Fig. 4: Ascending and descending portions of the middle turbinate, lateral aspect of nasal cavity, and coronal section. Ethmoturbinal is divided into lamina basilaris (red dotted line) and lamina recurvata (blue line). The lamina basilaris forms part of the lateral wall attachment. The lamina recurvata is more medial with a curled configuration. The lamina basilaris separates the draining pathway. The genu is the angle between the ascending and descending portions (yellow line). The other portion of ethmoturbinals show similar development. Page 42 of 74 Fig. 5: Ethmoid anatomy: The 5 basal-lamellae concept. The basal lamellae (blue arrows) separate the draining pathways (red arrows). The frontal and maxillary sinuses drain into the middle meatus via the frontal recess and hiatus semilunaris between the first (agger nasi cells and uncinate process) and second (ethmoid bulla) basal lamellae. The hiatus semilunaris superior opens between the second and third lamellae (middle turbinate). The third basal lamella separates the anterior and posterior ethmoid cells. The fourth basal lamella (superior turbinate) divides the posterior and postreme meatus. Page 43 of 74 Fig. 6: Migration of ethmoid cells. Agger nasi cells (AN) and ethmoid bulla (EB) are derived from pneumatization of the first and second basal lamellae. Agger nasi cells are the most anterior air cells and can invade uncinate process. The frontal cells, located above the agger nasi cells, form the anterior wall of the frontal recess. Additional anterior ethmoid cells are located around the ethmoid bulla (suprabullar recess, suprabullar cells, frontal bullar cells, and retrobullar recess) or orbital wall (supraorbital ethmoid cells, and Haller cells). Anterior ethmoid cells can extend to interfrontal sinus septa and crista galli. Posteriorly, they may extend to the turbinate (concha bullosa) or above the sphenoid sinus (Onodi cells). (Air cells around agger nasi cells [blue], ethmoid bulla [red], posterior air cells [yellow]) Page 44 of 74 Fig. 7: Medially bent uncinate process. The uncinate process is bent medially, contacting the middle turbinate and occluding the infundibulum (red arrow). Mucus drains through the accessory foramen (yellow arrow). In this case, mucosal thickening is caused by dental caries (blue arrow). Page 45 of 74 Fig. 8: Elongated or enlarged uncinate processes. This patient presented with left maxillary sinusitis. An elongated or enlarged uncinate process (red arrow in b) was found after cleaning of the nasal cavity. Fig. 9: Pneumatized uncinate process. Pneumatized uncinate process (red arrow) is believed to represent extension of agger nasi cells. In this case, the agger nasi cell extends to the uncinate process (yellow arrow, c). Page 46 of 74 Fig. 10: Four different attachments of the uncinate process. When the uncinate process attaches to ethmoid bulla or lamina papyracea (red arrows, a and b), the frontal recess opens directly into middle meatus. When the attachment is at the skull base or middle turbinate (red arrows, c and d), the frontal recess opens into the ethmoid infundibulum. Yellow dotted line shows drainage pathway. (Lamina terminalis (*)) Page 47 of 74 Fig. 11: Uncinate process attachment to the middle turbinate (red arrows). Anterior to posterior coronal CT images of the same patient as Fig 10d. In this condition, frontal recess opens into the ethmoid infundibulum.(yellow dots). Page 48 of 74 Fig. 12: Agger nasi cells. Agger nasi cells (green arrows) are the most anterior of the ethmoid cells. The agger nasi cells drain to the middle nasal meatus (orange arrows).The agger nasi cells are located posteromedial to the lacrimal sac and are the anatomical landmark for this sac during surgery. Page 49 of 74 Fig. 13: Ethmoid bulla. The ethmoid bulla (EB) is located in the anterior air cells and is usually the largest cell. EB is formed by pneumatization of the second basal lamella. (Agger nasi cell [AN], uncinate process [UP], sinus lateralis [SL], frontal recess [FR]) Page 50 of 74 Fig. 14: Torus lateralis. The torus lateralis (green arrows) represents an ethmoid bulla without pnenumatization. (Agger nasi cell [AN]) Fig. 15: Attachment of the middle turbinate. The insertion of the middle turbinate can be divided into 3 parts. The first or vertical part attaches to the cribriform plate. The second or oblique part attaches to the basal lamella or lamina papyracea. The third or horizontal part attaches to the perpendicular plate of the palatine bone. These attachments help to stabilize the middle turbinate. Page 51 of 74 Fig. 16: Concha bullosa. Concha bullosa of the middle turbinate in 2 different patients. Concha bullosa in patient 1 showing pneumatization of the middle turbinate (a, b). Concha bullosa may be the site of inflammatory disease ranging from simple mucosal thickening to mucocele (c, d). Page 52 of 74 Fig. 17: Paradoxical middle turbinate (a) and turbinate sinus (b). Paradoxical middle turbinate is formed by the inverse curling of middle turbinate and direct lateral convexity of the bone toward the lateral sinus wall. Turbinate sinus (red arrows, b) is formed by the concavity of the curled segment. Page 53 of 74 Fig. 18: Concha bullosa of the superior turbinate. Concha bullosa may occur in the superior turbinate, a structure derived from the fourth lamella. This variant may cause headache. Page 54 of 74 Fig. 19: Ethmoid roof. The ethmoid roof consists of fovea, crista galli, lateral lamella, and cribriform plate. Cribriform plate is a thin structure that may be dehiscent or defective. Page 55 of 74 Fig. 20: Foveal angle (a, b) and asymmetry of the ethmoid roof (c). Foveal angle is the angle between the fovea and lamina papyracea. A low sloping fovea predisposes to anterior cranial penetration during surgery. Differences in height between the right and left fovea are also significant for surgery. The ethmoid roof is lower and high sloping on the right side (arrow) Page 56 of 74 Fig. 21: Kero's classification: Type 1 (a), Type 2 (b), and Type3 (c). Kero's classification is based on the depth of the olfactory pit. In the type 3 in particular, the ethmoid roof is significantly higher than the anterior cranial fossa, increasing the surgical risk. Page 57 of 74 Fig. 22: Spontaneous cerebral fluid leakage from the left cribriform plate. Cribriform plate calcification is obscure on the left side (a). STIR sequences show fluid continuous to the subarachnoid space (red arrow, b). Fig. 23: Dehiscence of the lamina papyracea with medial herniation of orbital fat. Bony dehiscence occurs most often at the insertion of the basal lamella. Page 58 of 74 Fig. 24: Anterior and posterior ethmoid foramina. The medial notch of the orbit is a useful landmark for identifying the ethmoid foramen. The posterior ethmoid artery is located 10-12 mm behind anterior ethmoid foramen. Page 59 of 74 Fig. 25: Sinus lateralis (the lateral sinus of Grunwald, suprabullar recess, and retrobullar recess). The sinus lateralis(retrobullar recess, red dotted line, b-d) is the space between the ethmoid bulla (EB) and the third basal lamella (yellow dotted line). When ethmoid bulla dose not extend to the roof, the sinus lateralis continues to frontal recess (suprabullar recess, blue dotted line, c). The ethmoid bulla opens posteriorly into lateral recess (** in b). (Agger nasi cell [AN],suprabullar cell [*]) Page 60 of 74 Fig. 26: Suprabullar and frontal bullar cells. Suprabullar cells (Fig a, b *) do not extend to the frontal sinus in contrast to frontal bullar cells (Fig c, d **). The frontal recess may be narrow between the agger nasi cells (AN) and suprabullar or frontal bullar cells (b). (Ethmoid bulla [EB]) Page 61 of 74 Fig. 27: Inflammation of the frontal bullar cells. Frontal bullar cells are opacified (*). The frontal sinus is clear because the frontal recess is not involved. Page 62 of 74 Fig. 28: Pneumatization of the crista galli. Anterior ethmoid cells extending to the crista galli. Page 63 of 74 Fig. 29: Haller cells. Haller cells (red arrow) are located at the medial floor of the maxillary sinus below the ethmoid bulla (EB). When small, they may be similar appearance to the infraorbital canal (c, d). Due to their location next to the infundibulum, Haller cells may obstruct sinus drainage. (Uncinate process [*] posterior ethmoid cell [PC] Infraorbital canal [yellow arrow]) Page 64 of 74 Fig. 30: Frontal cells: Type 1 (a, b), Type 2 (c, d), and Type 3 (e, f). Frontal cells (*) are located above the agger nasi cells (AN). Frontal cells form the anterior wall of the drainage pathway from the frontal sinus (yellow dotted line), and encroach on the frontal recess or frontal sinus. Page 65 of 74 Fig. 31: Supraorbital ethmoid cells. The supraorbital ethmoid cell (*) extend to the orbital plate of the frontal bone. The anterior ethmoid foramen (red arrows) is easily identified by pneumatization of the supraorbital ethmoid cell. Page 66 of 74 Fig. 32: Mucocele of the supraorbital ethmoid cell. Left ethmoid mucocele (*) is bulging into orbital fossa. On the axial slices of the CT (b, c), supraorbital cell (*) are easily mistaken for frontal sinus (**). In this case frontal sinus and frontal recess (yellow dotted line and red arrow) are intact. Page 67 of 74 Fig. 33: Interfrontal sinus septal cell. The interfrontal sinus septal cell (*) is located between the frontal sinuses. This cell drains into frontal recess (red dotted line). Page 68 of 74 Fig. 34: Posterior ethmoid cell (PC) and postreme ethmoid cell (PSC) The superior nasal turbinate (fourth basal lamella; yellow arrows in a, b) separates the posterior and postreme ethmoid cells. Posterior ethmoid cell can invade into the roof of the maxillary sinus behind the Haller cell (c, d). Page 69 of 74 Fig. 35: Onodi cells. Onodi cells (OC), or sphenoethmoidal cells, represent invasion of the postreme ethmoid cells above the sphenoid sinus. These cells can contact the optic nerve (a, b) and internal carotid artery(c). Pneumatization may extend to the anterior clinoid process (*). Page 70 of 74 Fig. 36: Aspergillosis of the Onodi cell. Aspergillosis of the Onodi cell in a 60-year-old man with right visual disturbance. Right Onodi cell (*) invades the anterior clinoid process, with local inflammation (yellow arrows) involving the right optic nerve. As part of the ethmoid sinus, this structure should not be confused with the sphenoid sinus (**). Aspergillus was identified in the specimen postsurgery. Page 71 of 74 Conclusion Knowledge of anatomical variants of the ethmoid bone is necessary for the diagnosis of paranasal abnormalities and endoscopic treatment planning. An understanding of ethmoid bone embryology facilitates recognition of anatomical structures and normal variants in this area. References 1. Mizukoshi, O. Clinical Otorhinolaryngology and Head and Neck Surgery. Vol. 6A. 1989. 2. Schaefer, JP. The lateral wall of the cavum nasi in man, with special reference to the various developmental stages. J. Morph, 1910. 24: p. 613-707. 3. Zuckerkandl, E. Normale und pathologische Anatomie der Nasenhöhle und ihrer pneumatischen Anhänge. Band 2te Auflage, Wilhelm BraumUller, Wien & Leipzig, 1893. 4. Seydel, O. Über die Nasenhöle der höheren Säugethiere und des Menschen. Morph. Jahrb, 1891. 17: p. 44-99. 5. Killian, G. Zur Anatomie der Nase meschicher Embryonen. Arch. f Laryng, 1895. 2: p. 131-142. 6. Marquez, S, et al. Development of the ethmoid sinus and extramural migration: the anatomical basis of this paranasal sinus. Anat Rec (Hoboken), 2008. 291(11): p. 1535-53. 7. Goncalves, FG. Computed tomography of intra- and extramural ethmoid cells: iconographic essay. Radiol Bras, 2011. 44(5): p. 321-326. 8. Som, PM. Head and Neck imaging. 4 ed. Vol. 1. 2003. 153-165. 9. Huang, BY, et al. Failed endoscopic sinus surgery: spectrum of CT findings in the frontal recess. Radiographics, 2009. 29(1): p. 177-95. 10. Wright, ED, Bolger, WE. The bulla ethmoidalis: lamella or a true cell? J Otolaryngol, 2001. 30(3): p. 162-6. 11. Stilianos, E, Kountakis, TMÖ. Rhinologic and Sleep Apnea Surgical Techniques. 2007: Springer. 12. Lidov, M, Som, PM. Inflammatory disease involving a concha bullosa (enlarged pneumatized middle nasal turbinate): MR and CT appearance. AJNR Am J Neuroradiol, 1990. 11(5): p. 999-1001. Page 72 of 74 13. Danese, M, et al. [Influence of naso-sinusal anatomic variants on recurrent, persistent or chronic sinusitis. X-ray computed tomographic evaluation in 112 patients]. J Radiol, 1997. 78(9): p. 651-7. 14. Som, PM, Lawson, W. Interfrontal sinus septal cell: a cause of obstructing inflammation and mucoceles. AJNR Am J Neuroradiol, 2008. 29(7): p. 1369-71. 15. Homsioglou, E, et al. Pneumatized superior turbinate as a cause of headache. Head Face Med, 2007. 3: p. 3. 16. Keros, P. [On the practical value of differences in the level of the lamina cribrosa of the ethmoid]. Z Laryngol Rhinol Otol, 1962. 41: p. 809-13. 17. Toth, M, et al. Spontaneous cerebrospinal fluid rhinorrhea: a clinical and anatomical study. Laryngoscope. 120(9): p. 1724-9. 18. Moulin, G, et al. Dehiscence of the lamina papyracea of the ethmoid bone: CT findings. AJNR Am J Neuroradiol, 1994. 15(1): p. 151-3. 19. Souza, SA, et al. Anterior ethmoidal artery evaluation on coronal CT scans. Braz J Otorhinolaryngol, 2009. 75(1): p. 101-6. 20. Heinz Stammberger. Essentials of endoscopic sinus surgery. 1993: Mosby. 21. Park, SS, et al. Pneumatization Pattern of the Frontal Recess: Relationship of the Anterior-to-Posterior Length of Frontal Isthmus and/or Frontal Recess with the Volume of Agger Nasi Cell. Clin Exp Otorhinolaryngol. 3(2): p. 76-83. 22. Hajiioannou, J, Owens, D, and Whittet, HB. Evaluation of anatomical variation of the crista galli using computed tomography. Clin Anat. 23(4): p. 370-3. 23. Stackpole, SA, Edelstein DR. The anatomic relevance of the Haller cell in sinusitis. Am J Rhinol, 1997. 11(3): p. 219-23. 24. Bent JP, C-SC, Kuhn FA. The frontal cell as a cause of frontal sinus obstruction. Am J Rhinol., 1994. 8(849-57). Personal Information Thank you for reading our poster. If you have any questions or opinions, please contact me by email. Takashi Hiyama, M.D. Department of Radiology, University of Tsukuba Hospital Page 73 of 74 E-mail: [email protected] Page 74 of 74