Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiovascular disease wikipedia , lookup
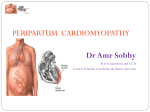
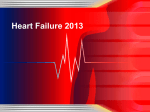
504 Differences in Cardiovascular Responses to Isoproterenol in Relation to Age and Exercise Training in Healthy Men John R. Stratton, MD; Manuel D. Cerqueira, MD; Robert S. Schwartz, MD; Wayne C. Levy, MD; Richard C. Veith, MD; Steven E. Kahn, MB, ChB; and Itamar B. Abrass, MD Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Background. Cardiac aging is characterized by a reduced heart rate response to (-agonist stimulation with isoproterenol, but whether the ejection fraction and other cardiovascular responses are reduced in humans is largely unknown. In addition, whether reduced (-agonist responses can be improved with exercise training has not been determined in humans. Methods and Resuls. Cardiovascular responses to graded isoproterenol infusions (3.5, 7, 14, and 35 ng/kg/min for 14 minutes each) were assessed in 15 older (age, 60-82 years) and 17 young (age, 24-32 years) rigorously screened healthy men. Thirteen older and 11 young subjects completed 6 months of endurance training and were retested. At baseline, the older group had reduced responses to isoproterenol for heart rate (+65% older versus +92% young, p<0.001), systolic blood pressure (+9%Y versus +24%, p<0.001), diastolic blood pressure (-12% versus -24%, p<0.05), ejection fraction (+12 versus +20 ejection fraction units, p<O.OOl), and cardiac output (+70%o versus + 100%, p<0.001). The mean plasma isoproterenol concentrations achieved during the infusions were marginally higher (p=0.07) in the older group (128±58, 227±64, 354±114, and 700±125 pg/ml) than in the young (79±20, 178±49, 273±79, and 571±139 pg/ml). Intensive training increased maximal oxygen consumption by 21% in the older group (28.9±4.6 to 35.1±3.8 ml/kg/min, p<O.OOl) and by 17% in the young (44.5±5.1 to 52.1±63 ml/kg/min,p<0.001), but training did not augment any of the cardiovascular responses to isoproterenol in either group. The mean plasma isoproterenol concentrations at the four infusion doses were unchanged after training in both groups. Conclusions. We conclude that there is an age-associated decline in heart rate, blood pressure, ejection fraction, and cardiac output responses to (-adrenergic stimulation with isoproterenol in healthy men. Altered (3-adrenergic responses probably contribute to the reduced cardiac responses to maximal exercise that also occur with aging. Furthermore, intensive exercise training does not increase cardiac responses to (-adrenergic stimulation with isoproterenol in either young or older men. The reduced (3-adrenergic response appears to be a primary age-associated change that is not caused by disease or inactivity. (Circulation 1992;86:504-512) KEY WoRDs * aging * responses, (3-adrenergic * ejection fraction * cardiac output * exercise T he age-associated decline in cardiovascular performance is more apparent during stress than at rest. The hallmarks of cardiovascular aging are a reduced maximal heart rate, ejection fraction, and, in most studies, cardiac output with exercise stress.1-6 ,B-Adrenergic pathways are a primary means of mediating the increased cardiovascular performance in response to stress,7-9 and abnormalities of ,B-adrenergic modulation of cardiovascular function may partially explain the cardiovascular changes of aging.10'11 From the Divisions of Cardiology, Gerontology, and Geriatric Medicine, Departments of Medicine and Psychiatry and Behavioral Sciences, Seattle VA Medical Center and University of Washington. Supported by the Medical Research Service of the Department of Veteran Affairs and by National Institutes of Health grant AG06581. Address for correspondence: John R. Stratton, MD, Cardiology (111-C), Seattle VA Medical Center, 1660 South Columbian Way, Seattle, WA 98108. Received January 8, 1992; revision accepted May 6, 1992. In animal models, catecholamine-stimulated heart rate, myocardial contractility, and vasodilatation all decline with age.1"'12 There are fewer data in humans, and many prior studies have been confounded by the failure to rigorously exclude underlying occult cardiovascular disease, which might alter 13-adrenergic responses. Available studies in humans have documented reduced blood pressure or venodilation responses to epinephrine or isoproterenol13'4 and smaller heart rate responses to isoproterenol"3 '5-17 in older than in younger subjects. It is unclear whether other cardiovascular responses, including ejection fraction and cardiac output, are also reduced with aging in humans. A reduction in ,B-adrenergic responses with aging may be an important mechanism for age-associated decreases in cardiovascular performance during exercise stress. In normal young or older subjects, dynamic exercise training maintains or improves exercise cardiac function, yet resting and submaximal levels of catecholamines are unchanged or reduced, whereas vagal tone may become more dominant.18-2' The maintenance or Stratton et al Aging, Exercise Training, and B-Adrenergic Responses Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 improvement in exercise cardiac function with reduced catecholamine concentrations suggests that the cardiac response to 13-adrenergic stimulation may be increased with training. However, the extent to which the cardiovascular improvements of training may be a result of improved ,3-adrenergic responses versus other mechanisms, such as training-induced hypertrophy, is unclear. Sensitivity to /3-adrenergic stimulation is clearly affected by exercise training in some systems; for example, training increases ,l-adrenergic-induced lipolysis.22,23 Results in animal models have been conflicting, with some training studies suggesting increased cardiovascular catecholamine responses24-27 and others showing no change or a decrease.28-3' There are only limited and conflicting data regarding training effects on cardiovascular responses to l3-adrenergic stimulation in young humans32-38 and no information in older humans. Information in older subjects is of particular interest because of the reduction in ,3-adrenergic cardiovascular responsiveness that occurs with aging. Several of the changes noted with aging are related to disuse and normalize with increased activity.39 This study had two purposes. The first was to determine whether rigorously screened sedentary healthy older men indeed do have reduced heart rate, blood pressure, ejection fraction, and cardiac output responses to ff-adrenergic stimulation with isoproterenol compared with healthy young men. The second purpose was to determine whether intensive endurance exercise training increases cardiovascular responses to isoproterenol in either young or older men. To minimize the possibility of underlying occult cardiac disease, which is common in elderly men," we used rigorous cardiac screening techniques. Our results document reduced cardiovascular responses to isoproterenol in healthy older men but no improvement in isoproterenol responses after a 6-month intensive endurance exercise training program in either young or older men. Methods Subjects Two age groups (18-32 years and 60-85 years old) of healthy men were studied. Subjects were excluded if they had any history of angina, myocardial infarction, stroke, hypertension, chronic pulmonary disease, diabetes, current medication use (prescription or over the counter), current smoking, exercise-limiting orthopedic impairment, or participation in a regular exercise program in the previous year. Entry laboratory requirements included a normal hematocrit, fasting blood glucose, total cholesterol, creatinine, resting ECG, M-mode and two-dimensional echocardiograms, and a Bruce protocol maximal exercise test, which included immediate postexercise and redistribution tomographic thallium imaging in all older subjects. No young subjects were excluded on the basis of exercise testing, but 22 of 37 potential older subjects were excluded (four with fixed thallium defects, seven with reversible thallium defects, five with ST segment depression with normal thallium, five with frequent premature beats, and one with claudication). Seventeen young (age, 24-32 years) and 15 older men (age, 60-82 years) entered the study and were evaluated before exercise training. Eleven of the young and 505 13 of the older subjects were also evaluated after exercise training. Six of the young subjects were not restudied for various reasons (withdrawal from training in four, refusal in one, technical problems in one). One of the older subjects underwent baseline testing but did not enter the training program, and one older subject's postexercise training data were not included because of the development of a significant intercurrent illness. The posttraining results, however, are not significantly different if this subject is included. All studies were conducted at least 36 hours after the last episode of exercise training to avoid the acute effects of exercise. This study was approved by the Human Subjects Committee of the University of Washington, and all subjects gave informed consent. Training Program and Maximal Oxygen Consumption The 6-month training program was supervised and monitored and consisted of walking, jogging, and bicycling for 45 minutes per session four or five times per week in a supervised setting. Training began at 50-60% of heart rate reserve, increased to 80-85% by the third or fourth month, and continued at that level for the remaining time. Maximal oxygen consumption was measured with a maximal Bruce treadmill protocol exercise test. The mean expiratory respiratory exchange ratio was 1.23±0.09 on the tests before training and 1.24±0.05 (p=NS) on the tests after training, indicating good effort. Study Protocol Intravenous catheters were inserted into a right hand vein and a right antecubital vein of each subject, after which they rested supine for 30 minutes before collection of baseline data. All studies were performed with the subject supine, and pretraining and posttraining studies were performed at the same time of day (10 AM to 12 noon). After the collection of baseline data, serial infusions of isoproterenol hydrochloride at 3.5, 7, 14, and 35 ng/kg/min were given for 14 minutes, each with a Harvard infusion pump (Harvard Apparatus, South Natick, Mass.). The infusion solution was prepared by diluting a sufficient amount of isoproterenol in 0.5N saline to achieve a total injectate volume of 20 ml at each infusion level. Goldstein et a140 have documented steady-state levels of isoproterenol at this duration of infusion. No complications occurred, and all subjects received all four doses on all studies. Data Collection and Processing At rest and during the final 2 minutes of each infusion dose, cardiac blood pool images, heart rate, and left arm automated sphygmomanometer blood pressure (Paramed Model 9350, Palo Alto, Calif.) were recorded. For radionuclide angiography, blood was obtained at the time of intravenous catheter placement and labeled with 20-30 mCi of 99"Tc as previously described.4' Images were acquired in the left anterior oblique projection, which offered the best septal definition, with a high-sensitivity parallel hole collimator and a General Electric 300 small-field-of-view camera interfaced to a Microdelta imaging terminal. Radionuclide images were acquired in 20-msec frames by forward and backward reconstruction with +20% arrhythmia rejection; a single beat was dropped after each rejected beat.42 Ejection fraction, end-diastolic volume, and end-systolic Circulation Vol 86, No 2 August 1992 506 volume were calculated by previously described methods.43 Cardiac output was obtained by multiplying the stroke volume times the mean heart rate during the acquisition. The correlation between left ventricular volume measurements by our radionuclide angiographic method of left ventricular volume determination and invasive contrast angiography in 19 subjects was r=0.90 with a mean difference of 1.6 ml and an SEM of 31.4 ml.43 Moreover, the interobserver reproducibility of this method for left ventricular volume determination is excellent (r=0.99; mean difference, 3.8%). Plasma isoproterenol concentrations were measured by high-performance liquid chromatography with electrochemical detection after alumina extraction.44 The sensitivity of the assay for isoproterenol is 10 pg/ml with a coefficient of variation of 3.4%. Resting plasma norepinephrine and epinephrine concentrations before and after training were measured with a single-isotope radioenzymatic assay.45,46 10050- 0* -,S n Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 vO HR SBP EF DBP CO FIGURE 1. Bar graph showing mean percentage change for several of the measurements in the young and older groups induced by the 35-nglkglmin isoproterenol dose before training. The response to isoproterenol was reduced for all variables in the older group (all p<O.05). HR heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; EF, ejection fraction; CO, cardiac output. isoproterenol infusion rate, the older group had a smaller increase in heart rate than the young (+65% older versus +92% young, p<0.001) (Figures 1 and 2, Table 1). At resting baseline, systolic and diastolic blood pressures were somewhat higher in the older group. During isoproterenol infusions, however, systolic blood pressure increased less in the older group (+9% versus +24% at the highest dose, p<0.001); systolic blood pressure at the highest dose was 151 mm Hg in the older group and 159 mm Hg in the young. In addition, diastolic blood pressure decreased significantly less during the infusions in the older group (-12% versus -24%, Results Isoproterenol Responses at Baseline Before Training At rest during the baseline condition, the older and young groups had similar heart rates. During the highest -X Y Pre -X Y Post 1 O Pre o OLD 1O Statistical Analysis Results are expressed as the mean±SD. The results in all young and older subjects before training were compared by ANOVA for repeated measures. The effects of training in each of the groups were also assessed by ANOVA for repeated measures. The reported probability values are those for the interaction terms (old versus young times dose or pretraining versus posttraining times dose). A value of p<0.05 was considered significant. A L* 150- Post -x Y Pre B X Y Post G 0 Pre vOOPost 120 p=0.0003 YoungiOld*Dose 110 Systolic pressure 100 90 80 70 60: au Rest C 3.5 x.ypre A rwc - 14 7 PostYPvrpre X. X ruKras - - 35 -U" p=O.0001 Young/Old*D~ 85- Rest Ejection fraction x 10000 - 9000 - 3.5 7 YPP-x YPr t 10000 80007000 -= 6000 ; 50OOO 1- 75. -=.--------- - 65 - 14 35 Pre -O OPost Young/OldiDose ,p=0.0001 Cardiac output ------- 4000 3000 1,I, J; Rest 3.5 7 14 35 ReSt 3.5 7 14 35 FIGURE 2. Graphs showing mean pretraining (pre) and posttraining (post) heart rate (beats per minute panel A), systolic blood pressure (mm Hg, panel B), ejection fraction (%o, panel C), and cardiac output (ml/min, panel D) responses to the serial isoproterenol doses (Rest, 3.5, 7, 11, and 35 nglkg/min) for the 11 young and 13 older subjects who underwent exercise training. The probability (p) values are for the young/old *dose term obtained from ANOVA for repeated measures. The older group had significantly reduced responses to isoproterenol on all of these measures. Stratton et al Aging, Exercise Training, and 13-Adrenergic Responses 507 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 TABLE 1. Mean Pretraining Responses to Isoproterenol in Young (n= 17) and Older (n=15) Men Rest 3.5 ng/kg/min 7 ng/kg/min 14 ng/kg/min 35 ng/kg/min Heart rate* (bpm) Young 61±7 69±11 74±11 86±14 117±15 Older 65±10 72±10 76± 11 89±12 107±12 Systolic BP* (mm Hg) Young 127±9 131±11 141±13 149±15 158±21 Older 138±11 144±20 146±17 152±18 151±18 Diastolic BP* (mm Hg) Young 76+5 70±5 65+6 65±9 58±10 Older 85±9 86±9 79±7 77±7 75±9 Mean BP (mm Hg) Young 93±4 90±5 91±6 93±7 92±9 Older 103±9 106±11 102±10 102±10 100±11 Ejection fraction* (%) Young 61±7 71±5 73±6 79±7 81±8 Older 59±5 65+7 66±5 69±5 71±6 Peak ejection rate* (EDV/sec) Young -3.3±0.5 -4.1±0.5 -4.8±0.7 -5.6±0.8 -7.5±+1.3 Older -3.0±0.6 -3.7±0.5 -4.3±0.4 -4.7±0.5 -5.8±1.1 EDV (ml) Young 132±39 129±45 126±42 117±39 105±30 Older 98±23 96±19 95±21 91±18 84±26 ESV (ml)* Young 52±21 39±18 35±16 26±13 22±12 Older 41±13 34±11 32+10 29±8 25±11 Stroke volume (ml) Young 80±21 90±28 91±28 91±30 84±20 Older 57±13 62±12 63±14 62±11 59±17 Cardiac output (l/min)* 4.9±+1.3 Young 6.2±1.9 6.7±1.9 7.7±2.5 9.8+2.5 Older 3.7±0.8 4.5±1.1 4.7±1.1 5.5±1.2 6.3±1.7 bpm, Beats per minute; BP, blood pressure; EDV, end-diastolic volume; ESV, end-systolic volume. Values are mean±SD. *p<0.05 by ANOVA for repeated measures (old vs. young x isoproterenol dose). p<0.05). The mean arterial blood pressure response was not significantly different between the two groups (-3% versus -1% at the highest dose). The mean resting ejection fraction was similar in the two groups. However, the ejection fraction response to isoproterenol was significantly smaller in the older group than the young (+ 12 ejection fraction units older versus +20 ejection fraction units young at the highest dose, p<0.001). The peak ejection rate response was also reduced in the older group (+93% older versus +127% young, p<0.001). In addition, the older men had a smaller increase from rest to the highest dose in the ratio of systolic blood pressure to end systolic TABLE 2. Mean Pretraining Isoproterenol Levels in Young (n=17) and Older (n=15) Men 14 7 3.5 35 ng/kg/min ng/kg/min ng/kg/min ng/kg/min Isoproterenol 79±20 Young Older 128±58 Values are mean±SD. 178±49 227±64 273±79 354±114 571±139 700±125 volume (+88% older versus +280% young, p<0.05). The end-diastolic volume response to isoproterenol was not significantly different between the two groups (- 14% older versus -20% young, p=NS), whereas the end-systolic volume response was significantly smaller in the older group (-39% older versus -58% young, p<O.OOl). The stroke volume response to isoproterenol was not significantly different between groups, but the cardiac output response was reduced in the older men (+ 70% older versus + 100% young, p< 0.001). The mean plasma isoproterenol concentrations achieved during the infusions were marginally higher in the older group (p=0.07) (Table 2). The older group had higher mean resting concentrations of norepinephrine (343+124 versus 244+78 pg/ml, p<0.05) and epinephrine (134 + 27 versus 95 + 57 pg/ml, p < 0.05). Endurance Training Results Endurance training increased maximal oxygen consumption by 21% in the older men (28.9+±4.6 versus 35.1+3.8 ml/kg/min,p<0.001) and by 17% in the young men (44.5+5.1 versus 52.1+6.3 ml/kg/min, p<0.001). Neither the absolute increases in maximal oxygen con- 508 Circulation Vol 86, No 2 August 1992 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 TABLE 3. Mean Pretraining and Posttraining Responses in the Young (n = 11) 3.5 ng/kg/min 7 ng/kg/min Rest Heart rate* (bpm) 74+9 62±7 70±9 Pre 56±4 59+7 66±7 Post Systolic BP (mm Hg) 131±10 140±9 129±8 Pre 144±12 126±7 135±10 Post Diastolic BP (mm Hg) 75±5 67±4 65±6 Pre 73±7 65±7 62±9 Post Mean BP (mm Hg) 89±4 90±4 93±4 Pre 91±6 88±6 89±5 Post Ejection fraction (%) 71±6 73±6 60±6 Pre 74±5 72±6 63+5 Post EDV (ml) 132±50 138±53 138±46 Pre 152±49 161±52 166±54 Post ESV (ml) 39±18 44±20 58±23 Pre 43±18 64±22 50±22 Post Stroke volume (ml) 81±26 95±33 95±33 Pre 111±32 103±34 113±30 Post Cardiac output (I/min) 6.9±2.3 4.9±1.6 6.5±2.1 Pre 7.3±2.0 6.7±1.9 5.7±1.8 Post 14 ng/kg/min 35 ng/kg/min 87+11 75+10 118+15 100±11 148±15 146±12 161±21 162±21 63±10 59±12 60±12 55±9 91±7 88±7 94±10 91±8 78±7 76±8 80±9 81±9 122±48 142±49 113+34 126±40 30±13 39±21 27±13 28±18 94±36 105±29 88±23 100±24 10.3±2.6 9.9±2.3 bpm, Beats per minute; BP, blood pressure; EDV, end-diastolic volume; ESV, end-systolic volume. Values are mean±SD. *p<0.05 by ANOVA for repeated measures (pretraining vs. posttraining times x isoproterenol dose). sumption nor the percent increase from baseline was significantly different between the two groups. In the young men after training, absolute heart rate responses to isoproterenol infusions were decreased (p<0.05) (Table 3). Systolic, diastolic, and mean blood pressure responses to isoproterenol were not altered by training in the young men. In addition, the ejection fraction, peak ejection rate, end-diastolic volume, endsystolic volume, stroke volume, and cardiac output responses to isoproterenol were not altered by training. In the older men, absolute heart rate responses to isoproterenol infusions were also decreased with training (p<0.05) (Table 4). None of the other responses to isoproterenol were altered by training in the older men (systolic or diastolic blood pressure, ejection fraction, peak ejection rate, end-diastolic volume, end-systolic volume, stroke volume, or cardiac output). The mean plasma isoproterenol concentrations at the various infusion doses (Table 5) and the mean resting norepinephrine and epinephrine concentrations were unchanged after training in both groups. The older group had no change in resting plasma norepinephrine concentration (362±+126 pg/ml before versus 313±96 pg/ml after) or in plasma epinephrine concentration (135±26 pg/ml before versus 135±39 pg/ml after) as a result of training. Similarly, the young group had no significant change in resting plasma norepinephrine 8.0±2.9 7.8±2.0 concentration (261±+79 pg/ml before versus 304±81 pg/ml after) or in plasma epinephrine concentration (77+±39 pg/ml before versus 88±+23 pg/ml after) as a result of training. Discussion There are two major findings of this study. First, cardiovascular responses to isoproterenol, including heart rate, ejection fraction, cardiac output, and systolic and diastolic pressures were reduced in healthy older men compared with younger men. Second, exercise training did not augment isoproterenol responses in these healthy men. Aging and /3-Adrenergic Responses The autonomic nervous system mediates, at least in part, most cardiovascular responses including preload, contractility, heart rate, afterload, and cardiac output.7-9'47 With aging, cardiovascular responses to stress are, in general, reduced in both animals and humans.11'2'47'48 Several factors may contribute to the deficiencies of aging, including occult disease (particularly coronary artery disease), deconditioning, and intrinsic age-associated structural and functional changes. In addition to these factors, however, there is evidence in animal models of an ageassociated reduction in 8-adrenergic-mediated changes in heart rate, vascular tone, and myocardial contractili- Stratton et al Aging, Exercise Training, and P-Adrenergic Responses 509 TABLE 4. Mean Pretraining and Posttraining Responses in the Older Group (n= 13) Rest 3.5 ng/kg/min 7 ng/kg/min 14 ng/kg/min 35 ng/kg/min Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Heart rate* (bpm) 107+12 89±13 73±10 77±11 Pre 66+10 88+14 71±11 62±9 65+9 Post 57+8 Systolic BP (mm Hg) 153+18 152+18 Pre 138+11 147±18 147+18 155±21 147±16 150±16 Post 136±9 140±11 Diastolic BP (mm Hg) 75±9 79±7 77±7 Pre 85±9 85±8 65±6 73±9 72±11 Post 84±8 76±8 Mean BP (mm Hg) 101±11 102±10 Pre 103±9 106±11 101±10 95±9 98±89 98±11 Post 101±8 98±7 Ejection fraction (%) 71±6 Pre 66±6 67±5 69±5 59±5 71±7 69±7 70±5 Post 61±6 68±5 EDV (ml) 85±26 Pre 97±24 96±20 94±22 90±18 106±30 Post 126±39 115±25 113±25 113±25 ESV (ml) 33±11 31±9 40±13 28±8 25±11 Pre 51±22 38±13 36±13 34±10 30±11 Post Stroke volume (ml) 63±12 62±12 57±13 63±15 60±17 Pre 78±16 75±23 Post 75±19 77±16 79±17 Cardiac output (1/min) 3.7±0.8 4.6±1.0 4.8±1.1 5.5±1.3 6.4±1.8 Pre 4.3±1.1 4.8±1.2 5.0±1.0 5.6±1.3 Post 6.4±1.4 bpm, Beats per minute; BP, blood pressure; EDV, end-diastolic volume; ESV, end-systolic volume. Values are mean±SD. *p<0.05 by ANOVA for repeated measures (pretraining vs. posttraining x isoproterenol dose). ty.10llA47-53 The reduced contractile and vasodilating responses to ,B-adrenergic stimulation are not a generalized phenomenon but rather are specific for 13-agonists, as the responses to other agents (calcium or nitrates) are maintained.52-54 Because isoproterenol is not significantly taken up by storage sites, the reduced responses cannot be explained by differential uptake or release of the mediator from storage sites. In humans, there are fewer data, but studies have noted smaller changes in systolic and diastolic pressures during epinephrine or isoproterenol infusions with aging,13'55 reduced isoproterenol-induced venodilation,14 and a reduced heart response to isoproterenol.15'175657 Whether the contractile response to /3-adrenergic stimTABLE 5. Pretraining and Posttraining Isoproterenol Levels in the Young (n=11) and Older Group (n= 13) 14 35 7 3.5 ng/kg/min Young Pre 71±+-17 71+43 Post Older Pre 132+62 Post 130±60 Values are mean±SD. ng/kg/min ng/kg/min ng/kg/min 170±44 136±66 268+91 233+57 522±112 223±68 211±78 354±114 316±63 689±124 673±139 511 ± 132 ulation is reduced with aging in humans is uncertain. One recent study, in which occult coronary artery disease was not excluded, found a reduced echocardiographically measured shortening fraction response to isoproterenol.56 We found a reduced ejection fraction and peak ejection rate response in older men. The reduced ejection cannot be explained by a greater systolic pressure response, because the systolic pressure actually rose more in the young than the older group; at the highest infusion dose, when the ejection fraction was 10 units higher in the young than in the older group, the systolic pressure was similar (158+21 mm Hg young versus 151+± 18 mm Hg older). In addition, the ratio of systolic pressure to end-systolic volume, which partially normalizes for differences in afterload, rose by 280% in the young compared with 88% in the older group. Although none of the measures of contractility used in this study are free of significant limitations, taken together the results suggest a reduced inotropic response of healthy older hearts to ,B-adrenergic stimulation. Our subjects were thoroughly screened to exclude any overt or occult disease, and a high proportion of older subjects were eliminated because of abnormal screening exercise tolerance tests. Therefore, underlying but undiagnosed disease is an unlikely explanation for our results. The reduced responses of the older group were 510 Circulation Vol 86, No 2 August 1992 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 also probably not a result of differences in circulating isoproterenol concentrations, as marginally higher concentrations were present in the older group, possibly because of a smaller volume of distribution or alterations in clearance. Thus, the present study might have slightly underestimated the age-associated decline in isoproterenol responses. Another possible explanation for the reduced isoproterenol response at baseline in the older group might be deconditioning.47 However, deconditioning does not appear to account for the diminished responses in the older group, because there was no change with training. Therefore, the most likely reason for the observed differences is an age-associated diminution in /3-adrenergic responses similar to that noted in animal models. The available data suggest that the age-associated decrease in catecholamine responses may be multifactorial and related to changes in both receptor and postreceptor function.58,59 With aging there are reductions in p-receptor agonist binding affinity in humans,59-62 cardiac adenylate cyclase activity in animals, and lymphocyte adenylate cyclase in humans,63-65 but no change in the numbers or antagonist affinity of p-receptors in humans.61,6266 The receptor alterations may account, at least in part, for the decreased p-agonist responses with aging. The reduced responses to isoproterenol in the older group parallel the changes seen with exercise stress, in which heart rate and ejection fraction responses are decreased with aging.4,10,67 Our findings are consistent with the interpretation that the reduced responses at peak exercise are caused, at least in part, by reduced p8-adrenergic responses. Conway et a168 noted that the age-related differences in cardiac output during exercise were lessened during 8-blockade, also suggesting that the differences seen with age result from a decrease in ,8-adrenergic responses. Exercise Training and p-Adrenergic Responses Plasma catecholamine concentrations are reduced at submaximal work rates after training,18-20 but exercise cardiac output is maintained or increased,21'69 which could be explained by an increased sensitivity to adrenergic stimulation, among other mechanisms. Training does clearly increase p-adrenergic responses to epinephrine-induced lipolysis.23'70 Whether training increases cardiovascular sensitivity to catecholamines, however, remains unclear. Two animal studies showed increased contractility of isolated papillary muscles to isoproterenol,24'25 whereas a third study noted no change in norepinephrine sensitivity.28 In dogs, training resulted in greater isoproterenol-induced changes in stroke volume, stroke work, and maximal velocity of contraction and systemic vascular resistance but not ejection fraction.26'27 In rats, one group found decreased vascular sensitivity to norepinephrine after training,29 whereas a second study found no change in hindlimb vascular resistance to epinephrine.30 Although maximal heart rate response to isoproterenol was reduced in trained rats71 and pigs,31 other studies have found increased or unchanged adrenergic heart rate sensitivity.72 Previous data in humans regarding the effects of exercise training on ,B-adrenergic responses are limited and conflicting. Heart rate increases with isoproterenol epinephrine have been similar in trained and untrained young subjects.33-35,37,73 Cross-sectional studies have reported an increase3274 and a reduced73 blood pressure response to norepinephrine or epinephrine and no difference in cardiac output to isoproterenol in trained compared with untrained subjects.36 In another cross-sectional study, both the vasodilator and systolic pressor responses to epinephrine were greater in endurance-trained subjects; in a longitudinal component to this study, however, endurance training failed to alter the systolic or diastolic pressure responses to epinephrine.37 In longitudinal training studies in humans, no apparent change was noted in inotropic or chronotropic sensitivity to epinephrine.33,37 However, the results of these two studies are hampered by the small numbers (n =6 and n = 10) and by the relatively crude contractility measures by echo and systolic time intervals. A recently reported longitudinal study in 16 young subjects (mean age, 27 years) noted an improvement in echo-measured fractional shortening.38 The reasons for the discrepancy between findings of the study by Spina and colleagues38 and the findings in our young group are unclear but may relate to measurement techniques (echo versus nuclear), patient populations (men and women versus all men), or, less likely, training intensity (+20% versus + 17% maximal oxygen consumption). The current study found no evidence of increased heart rate, blood pressure, ejection fraction, or cardiac output responses to isoproterenol. The lower heart rate at all levels of infusion was probably a result of increased vagal tone. Thus, we conclude that regular exercise does not increase /8-adrenergic responses in healthy young or older men. or Limitations The observed hemodynamic changes represent both the primary effects of the infusion and secondary reflex responses. The relative contributions cannot be determined. Baroreflex sensitivity is decreased with age,75 but differences in baroreflex sensitivity, if anything, might tend to minimize the age differences observed. Vagal inhibition of ventricular function probably occurs in humans.76 An increase in vagal tone as a result of training (as suggested by the reduced heart rate) might mask any training-induced improvement in isoproterenol responses. Although we consider this unlikely, we cannot exclude this possibility because we did not pretreat with atropine. In addition, our study cannot differentiate and 82-adrenergic receptor responses. Conclusions regarding the lack of a training effect in ,B-adrenergic responses must be tempered by the relatively small number of subjects. When all subjects were combined (n = 24), however, there was still no evidence of an enhanced cardiovascular response to isoproterenol after training for any of the measured variables. The ejection fraction is a relatively crude measure of contractility. More precise measures require invasive methods, which were not deemed justifiable in this healthy sample. The reduced ejection fraction during isoproterenol in the older group cannot be explained by differences in heart rate. Increasing the heart rate alone causes no significant change in the ejection fraction.77 In this study, we did not measure maximal ,-adrenergic /3k- responses but only submaximal safety concerns. responses because of Stratton et al Aging, Exercise Training, and j-Adrenergic Responses In conclusion, the heart rate, blood pressure, ejection fraction, and cardiac output responses to graded doses of isoproterenol are reduced in healthy older men. Endurance exercise training does not enhance f-adrenergic responses in either older or young men. Reduced ,f-adrenergic responses probably contribute to the decreased cardiovascular responses to maximal exercise that occur with aging. Acknowledgments The authors thank Kevin Murphy, Jean Hadlock, John Martin, Candy Sands, Geri Orta, Dale Matsuoka, and Anna Coleman for their technical help. We thank Robert A. Bruce, MD, for his help and encouragement in planning and conducting the study and for reviewing the manuscript. We thank Jim Kousbaugh for his help in preparation of the manuscript. References Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 1. Raven PB, Mitchell JH: Effect of aging on the cardiovascular response to dynamic and static exercise, in Weisfeldt M (ed): The Aging Heart. New York, Raven Press, 1980, chap 10, pp 269-296 2. Hossack KF, Bruce RA: Maximal cardiac function in sedentary normal men and women: Comparison of age-related changes. JAppl Physiol 1982;53:799-804 3. Julius S, Amery A, Whetlock LS, Conway J: Influence of age on the hemodynamic response to exercise. Circulation 1967;36: 222-229 4. Port S, Cobb FR, Coleman RE, Jones RH: Effect of age on the response of the left ventricular ejection fraction to exercise. N Engl J Med 1980;303:1133-1137 5. Rodeheffer RJ, Gerstenblith G, Becker LC, Fleg JL, Weisfeldt ML, Lakatta EG: Exercise cardiac output is maintained with advancing age in healthy human subjects: Cardiac dilatation and increased stroke volume compensate for a diminished heart rate. Circulation 1984;69:203-213 6. Higginbotham MB, Morris KG, Williams RS, Coleman RE, Cobb FR: Physiologic basis for the age-related decline in aerobic work capacity. Am J Cardiol 1986;57:1374-1379 7. Neil E: Catecholamines and the cardiovascular system, in Blaschko H, Sayers G, Smith AD (eds): Handbook of Physiology, Section 7. Washington, DC, American Physiology Society, 1975, pp 473-489 8. Levy MN, Martin PJ: Neural control of the heart, in Berne RM (ed): Handbook of Physiology, Section 2. Washington, DC, American Physiology Society, 1979, pp 581-620 9. Christensen NJ, Galbo H: Sympathetic nervous activity during exercise. Annu Rev Physiol 1983;45:139-147 10. Gerstenblith G, Renlund DG, Lakatta EG: Cardiovascular response to exercise in younger and older men. Fed Proc 1987;46: 1834-1839 11. Weisfeldt ML, Lakatta EG, Gerstenblith G: Aging and the heart, in Braunwald E (ed): Heart Disease: A Textbook of Cardiovascular Medicine, ed 4. Philadelphia, WB Saunders Co, 1992, chap 52, pp 1656-1669 12. Lakatta EG: Determinants of cardiovascular performance: Modification due to aging. J Chronic Dis 1983;36:15-30 13. van Brummelen P, Buhler FR, Kiowski W, Amann FW: Agerelated decrease in cardiac and peripheral vascular responsiveness to isoprenaline: Studies in normal subjects. Clin Sci 1981;60: 571-577 14. Hiremath AN, Pershe RA, Hoffman BB, Blaschke TF: Comparison of age-related changes in prostaglandin El and betaadrenergic responsiveness of vascular smooth muscle in adult males. J Gerontol 1989;44:M13-M17 15. Fitzgerald D, Doyle V, Kelly JG, O'Malley K: Cardiac sensitivity to isoprenaline, lymphocyte beta-adrenoceptors and age. Clin Sci 1984;66:697-699 16. Klein C, Hiatt WR, Gerber JG, Nies AS: Age does not alter human vascular and nonvascular beta 2-adrenergic responses to isoproterenol. Clin Pharmacol Ther 1988;44:573-578 17. Vestal RE, Wood AJJ, Shand DG: Reduced ,-adrenoreceptor sensitivity in the elderly. Clin Pharmacol Ther 1979;26:181-186 18. Winder WW, Hickson RC, Hagberg JM, Ehsani AA, McLane JA: Training-induced changes in hormonal and metabolic responses to submaximal exercise. JAppl Physiol 1979;46:766-771 511 19. Cousineau D, Ferguson RJ, deChamplain J, Gauthie RP, Cote P, Bourassa M: Catecholamines in coronary sinus during exercise in man before and after training. JAppl Physiol 1977;43:801-806 20. Hartley LH, Mason JW, Hogan RP, Jones LG, Kotchen TA, Mougey EH, Wherrg FE, Pennington LL, Ricketts PT: Multiple hormonal responses to prolonged exercise in relation to physical training. J Appl Physiol 1972;33:607-610 21. Ehsani AA, Ogawa T, Miller TR, Spina RJ, Jilka SM: Exercise training improves left ventricular systolic function in older men. Circulation 1991;83:96-103 22. Crampes F, Beauville M, Riviere D, Garrigues M, Lafontan M: Lack of desensitization of catecholamine-induced lipolysis in fat cells from trained and sedentary women after physical exercise. J Clin Endocrinol Metab 1988;67:1011-1017 23. Martin WH, Coyle EF, Joyner M, Santensanio D, Ehsani AA, Holloszy JO: The effects of stopping exercise training on epinephrine induced lipolysis. JAppl Physiol 1984;56:845-848 24. Mole PA: Increased contractile potential of papillary muscles from exercise-trained rat hearts. Am J Physiol 1978;234(Heart Circ Physiol):H421-H425 25. Wyatt HL, Chuck L, Rabinowitz B, Tyberg JV, Parmley WW: Enhanced cardiac response to catecholamines in physically trained cats. Am J Physiol 1978;234(Heart Circ Physiol):H608-H613 26. Ramo P, Kettunen R, Hirvonen L: Hemodynamic effects of endurance training on canine left ventricle. Am J Physiol 1987;252(Heart Circ Physiol):H7-H13 27. Ramo P, Kettunen R, Timisjarvi J, Takala T, Hirvonen L: Anabolic steroids alter the haemodynamic effects of endurance training on the canine left ventricle. Pfiugers Arch 1987;410:272-278 28. Williams JF, Potter RD: Effect of exercise conditioning on the intrinsic contractile state of cat myocardium. Circ Res 1976;39: 425-428 29. Wiegman DL, Harris PD, Joshua IG, Miller FN: Decreased vascular sensitivity to norepinephrine following exercise training. JAppl Physiol 1981;51:282-287 30. Richter EA, Christensen NJ, Ploug T, Galbo H: Endurance training augments the stimulatory effect of epinephrine on oxygen consumption in perfused skeletal muscle. Acta Physiol Scand 1984; 120:613-615 31. Hammond HK, White FC, Brunton LL, Longhurst JC: Association of decreased myocardial 3-receptors and chronotropic response to isoproterenol and exercise in pigs following chronic dynamic exercise. Circ Res 1987;60:720-726 32. LeBlanc J, Boulay M, Dulac S, Jobin M, Labrie A, RousseauMigneron S: Metabolic and cardiovascular responses to norepinephrine in trained and nontrained human subjects. JAppl Physiol 1977;42:166-173 33. Martin WH, Coyle EF, Ehsani AA: Cardiovascular sensitivity to epinephrine in the trained and untrained states. Am J Cardiol 1984;54:1326-1330 34. Williams RS, Eden RS, Moll ME, Lester RM, Wallace AG: Autonomic mechanisms of training bradycardia: ,-adrenergic receptors in humans. JAppl Physiol 1981;51:1232-1237 35. Duncan JJ, Farr JE, Upton SJ, Hagan RD, Oglesby ME, Blair SN: The effects of aerobic exercise on plasma catecholamines and blood pressure in patients with mild essential hypertension. JAMA 1985;254:2609-2613 36. Lehmann M, Dickhuth HH, Schmid P, Porzig H, Keul J: Plasma catecholamines, beta-adrenergic receptors, and isoproterenol sensitivity in endurance trained and non-endurance trained volunteers. Eur JAppl Physiol 1984;52:362-369 37. Svedenhag J, Martinson A, Ekblom B, Hjemdahl P: Altered cardiovascular responsiveness to adrenaline in endurance trained subjects. Acta Physiol Scand 1986;126:539-550 38. Spina RJ, Ogawa T, Coggan AR, Holloszy JO, Ehsani AA: Exercise training improves left ventricular contractile response to beta adrenergic agonist. J Appl Physiol 1992;72:307-311 39. Bortz WM: Disuse and aging. JAMA 1982;248:1203-1208 40. Goldstein DS, Zimlichman R, Stoll R, Keiser HR: Plasma catecholamine and hemodynamic responses during isoproterenol infusions in humans. Pharmacol Ther 1986;40:233-238 41. Cerqueira MD, Harp GD, Ritchie JL, Stratton JR, Walker RD: Rarity of preclinical alcoholic cardiomyopathy in chronic alcoholics less than 40 years of age. Am J Cardiol 1991;67:183-187 42. Wallis JW, Wu-Connolly L, Rocchini AP, Juni JE: Dynamic arrhythmia filtration for gated blood pool imaging: Validation against list mode technique. J Nucl Med 1986;27:1347-1352 43. Levy WC, Cerqueira MD, Matsuoka DT, Harp GD, Sheehan FH, Stratton JR: Four radionuclide methods of left ventricular volume 512 44. 45. 46. 47. 48. 49. 50. Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. Circulation Vol 86, No 2 August 1992 determination: Comparison of manual and a new automated technique. J Nucl Med 1992;33:763-770 Goldstein DS, Feuerstein G, Izzo JL, Kopin IJ, Keiser HR: Validity and reliability of liquid chromatography with electrochemical detection for measuring plasma levels of norepinephrine and epinephrine in man. Life Sci 1981;28:467-475 Evans MI, Halter JB, Porte D: Comparison of double- and singleisotope enzymatic derivative methods for measuring catecholamines in human plasma. Clin Chem 1978;24:567-570 Stratton JR, Halter JB, Hallstrom AP, Caldwell JH, Ritchie JL: Comparative plasma catecholamine and hemodynamic responses to handgrip, cold pressor and supine bicycle exercise testing in normal subjects. JAm Coll Cardiol 1983;2:93-104 Filburn CR, Lakatta EG: Age-related alterations in ,B-adrenergic modulation of cardiac cell function, in Johnson JJ (ed): Aging and Cell Function. New York, Plenum Publishing, 1984, chap 4, pp 211-246 Lakatta EG, Yin FC: Myocardial aging: Functional alterations and related cellular mechanisms. Am J Physiol 1982;242:H927-H941 Lakatta EG, Gerstenblith G, Angell CS, Shock NW, Weisfeldt ML: Diminished inotropic response of aged myocardium to catecholamines. Circ Res 1975;36:262-269 Dobson JG Jr, Fenton RA, Romano FD: Increased myocardial adenosine production and reduction of 8-adrenergic contractile response in aged hearts. Circ Res 1990;66:1381-1390 Yin FC: Aging and aortic impedance in beagle dogs. Mech Ageing Dev 1988;42:49-62 Guarnieri T, Filburn CR, Zitnik G, Roth GS, Lakatta EG: Contractile and biochemical correlates of beta adrenergic stimulation of the aged heart. Am J Physiol 1980;239:H501-H508 Deisher TA, Mankani S, Hoffman BB: Role of cyclic AMPdependent protein kinase in the diminished beta adrenergic responsiveness of vascular smooth muscle with increasing age. J Pharmacol Exp Ther 1989;249:812-819 Fleisch JH, Maling HM, Brodie BB: Beta receptor activity in aorta: Variations with aging and species. Circ Res 1970;26:151-162 Wilkie FL, Halter JB, Prinz PN, Benedetti C, Eisdorfer C, Atwood B, Yamasaki D: Age-related changes in venous catecholamines basally and during epinephrine infusion in man. J Gerontol 1985; 40:133-140 Chou HT, Yokota Y, Fukuzaki H: Left ventricular reserve of the hypertrophied heart in patients with systemic hypertension and hypertrophic cardiomyopathy: Relation to age and left ventricular relative wall thickness. Jpn Circ J 1990;54:373-382 Johansson SR, Hjalmarson A: Age and sex differences in cardiovascular reactivity to adrenergic agonists, mental stress and isometric exercise in normal subjects. Scand J Clin Lab Invest 1988; 48:183-191 Fan TH, Banerjee SP: Age-related reduction of beta-adrenoceptor sensitivity in rat heart occurs by multiple mechanisms. Gerontology 1985;31:373-380 Scarpace PJ: Decreased receptor activation with age: Can it be explained by desensitization? JAm Geriatr Soc 1988;36:1067-1071 Montamat SC, Davies AO: Physiological response to isoproterenol and coupling of beta-adrenergic receptors in young and elderly human subjects. J Gerontol 1989;44:100-1o5 61. Feldman RD, Limbird LE, Nadeau J, Robertson D, Wood AJ: Alterations in leukocyte beta-receptor affinity with aging: A potential explanation for altered beta-adrenergic sensitivity in the elderly. N Engl J Med 1984;310:815-819 62. Winther K, Naesh 0: Aging and platelet beta-adrenoceptor function. Eur J Pharmacol 1987;136:219-223 63. Scarpace PJ, Armbrecht HJ: Adenylate cyclase in senescence: Catecholamine and parathyroid hormone pathways. Rev Clin Basic Pharm 1987;6:105-118 64. Abrass IB, Scarpace PJ: Catalytic unit of adenylate cyclase: Reduced activity in aged human lymphocytes. J Clin Endocrinol Metab 1982;55:1026-1028 65. Scarpace PJ: Forskolin activation of adenylate cyclase in rat myocardium with age: Effects of guanine nucleotide analogs. Mech Ageing Dev 1990;52:169-178 66. Abrass I, Scarpace PJ: Human lymphocyte beta-adrenergic receptors are unaltered with age. J Gerontol 1981;36:298-301 67. Levy WC, Cerqueira M, Abrass I, Schwartz R, Stratton JR: Stroke volume is maintained in advanced age by cardiac dilatation despite decreased contractility with supine bicycle exercise. (abstract) J Nucl Med 1990;(suppl 31):838 68. Conway J, Wheeler R, Sannerstedt R: Sympathetic nervous activity during exercise in relation to age. Cardiovasc Res 1971;5: 577-581 69. Jennings G, Nelson L, Nestel P, Esler M, Korner P, Burton D, Bazelmans J: The effects of changes in physical activity on major cardiovascular risk factors, hemodynamics, sympathetic function, and glucose utilization in man: A controlled study of four levels of activity. Circulation 1986;73:30-40 70. Crampes F, Riviere D, Beauville M, Marceron M, Garrigues M: Lipolytic response of adipocytes to epinephrine in sedentary and exercise trained subjects: Sex related differences. EurJApplPhysiol 1989;59:249-255 71. Bolter CP, Atkinson KJ: Maximum heart rate responses to exercise and isoproterenol in the trained rat. Am J Physiol 1988;254: R834-R839 72. Schaible TF, Scheuer J: Cardiac adaptations to chronic exercise. Prog Cardiovasc Dis 1985;27:297-324 73. Pavlik G, Frenkl R: Sensitivity to catecholamines and histamine in the trained and in the untrained organism and sensitivity changes during digestion. Eur JAppl Physiol 1975;34:199-204 74. Mann SJ, Krakoff LR, Felton K, Yeager K: Cardiovascular responses to infused epinephrine: Effect of state of physical conditioning. J Cardiovasc Pharmacol 1984;6:339-343 75. Gribbin B, Pickering TG, Sleight P, Peto R: Effect of age and high blood pressure on baroreflex sensitivity in man. Circ Res 1971;29: 424-431 76. Stratton JR, Pfeifer MA, Halter JB: The hemodynamic effects of sympathetic stimulation combined with parasympathetic blockade in man. Circulation 1987;75:922-929 77. Johannessen KA, Cerqueira M, Veith RC, Stratton JR: Influence of sympathetic stimulation and parasympathetic withdrawal on Doppler echocardiographic left ventricular diastolic filling velocities in young normal subjects. Am J Cardiol 1991;67:520-526 Differences in cardiovascular responses to isoproterenol in relation to age and exercise training in healthy men. J R Stratton, M D Cerqueira, R S Schwartz, W C Levy, R C Veith, S E Kahn and I B Abrass Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Circulation. 1992;86:504-512 doi: 10.1161/01.CIR.86.2.504 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1992 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/86/2/504 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/