Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
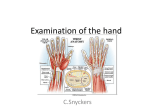
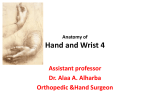
Anatomy of the Hand and Wrist Arthritides of the Hand and Wrist Bone and Soft-Tissue Tumors of the Hand and Forearm Traumatic Brachial Plexus Injuries Dupuytren Contracture Flexor and Extensor Tendon Injuries Frostbite Infections of the Hand Nerve Compression Syndromes Replantations in the Upper Extremities Soft-Tissue Coverage Vascular Disorders Wrist Arhtoscopy A. B. C. D. E. The Nail bed The Skin/Fascia Compartments of the Forearm and Hand Palmar Spaces of the Hand The Digits F. G. H. I. J. The Hand The Wrist The Forearm Vascular Anatomy of the Hand, Wrist, and Forearm Nerves of the Hand, Wrist, and Forearm Figure 1: Illustrations of the cross-sectional anatomy of the compartments of the forearm (A) and hand (B). (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; (B) and Charles A. Goldfarb, MD. Table 1 Contributions of Interosseous and Lumbrical Muscles to the Extensor Apparatus Muscles Dorsal interosseous Lumbrical Location and Action 4 dorsal interossei Bipennate; arise from both metacarpals of intermetacarpal space Each dorsal interosseous has 2 muscle bellies: Superficial •passes under sagittal hood to become medial tendon •insertion: lateral tubercle of proximal phalanx •action: abductor of digit Deep •passes over sagittal hood to become lateral tendon •insertion: transverse fibers of extensor apparatus •action: flexor of MCP joint Originate from FDP tendon Passes volar to the deep transverse intermetacarpal ligament Located on the radial side of each digit Insertion: radial lateral band (of extensor apparatus) via oblique fibers Action: extend PIP and DIP joints Only muscle able to “relax” its antagonist (origin on FDP) Innervation: 1st and 2nd lumbricals (unipennate): median nerve 2nd and 3rd lumbricals (bipennate): ulnar nerve MCP = metacarpophalangeal, PIP = proximal interphalangeal, DIP = distal interphalangeal (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC, and Charles A. Goldfarb, MD.) Figure 2: Anatomic zones for the characterization of flexor tendon injuries. (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Figure 3: Commonly accepted flexor pulley nomenclature (A1-A5 and C1-C3). Note ulnar bursa (UB) and radial bursa (RB). (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Table 2 The Interosseous Muscles Muscle Insertion Action Characteristics Superficial muscle belly Lateral tubercle of proximal phalanx Abduct digit Bipennate Deep muscle belly Transverse fibers of extensor apparatus Flex MCP joint Bipennate Volar Extensor apparatus; no insertion into the proximal phalanx Flex MCP joint; adduct index, ring, and little Unipennate fingers Dorsal MCP = metacarpophalangeal Table 3 The Lumbrical Muscles Muscle Origin Insertion Innervation Action Characteristics First lumbrical FDP tendon Radial lateral band Median nerve Extend PIP and DIP joints Unipennate Second lumbrical FDP tendon Radial lateral band Median nerve Extend PIP and DIP joints Unipennate Third lumbrical FDP tendon Radial lateral band Ulnar nerve Extend PIP and DIP joints Bipennate Fourth lumbrical FDP tendon Radial lateral band Ulnar nerve Extend PIP and DIP joints Bipennate FDP = flexor digitorum profundus, PIP = proximal interphalangeal, DIP = distal interphalangeal Table 4 The Thenar Muscles Muscle Abductor pollicis brevis Origin Insertion Innervation Median nerve, 95% Transverse carpal Radial base of P1, MCP Ulnar nerve, 2.5% ligament, FCR sheath, joint capsule, radial Both, 2.5% trapezium, scaphoid sesamoid Flexor pollicis brevis Transverse carpal ligament Thumb MCP joint capsule and radial sesamoid Opponens pollicis Transverse carpal ligment, trapezium, thumb CMC capsule Volar-radial distal thumb metacarpal Adductor pollicis Long finger metacarpal Ulnar sesamoid of thumb, ulnar base of P1, dorsal apparatus Superficial head: median nerve Deep head: ulnar nerve Action Abduction and flexion of the thumb metacarpal Ulnar angulation at the MCP joint Thumb IP joint extension Flexion of thumb metacarpal and P1 Thumb pronation Thumb IP joint extension Median nerve, 83% Ulnar nerve, 10% Both, 7% Flexion and pronation of thumb metacarpal Ulnar nerve Adduction of thumb metacarpal Thumb IP joint extension FCR = flexor carpi radialis, MCP = metacarpophalangeal, IP = interphalangeal, CMC = carpometacarpophalangeal Table 5 The Hypothenar Muscles Muscle Origin Insertion Abductor digiti minimi Distal pisiform, FCU insertion Ulnar base P1, 90% Extensor apparatus, 10% Flexor digiti minimi Opponens digiti minimi Innervation Action Ulnar nerve Strong abductor of little finger Mild MCP joint flexion of little finger Little finger IP joint extension Transverse carpal ligament, hook of hamate Little finger P1 palmar Ulnar nerve base Little finger flexion at MCP joint Transverse carpal ligament, hook of hamate Distal three quarters of the ulnar aspect of Ulnar nerve the little finger metacarpal Supination of the little finger metacarpal Deepens palm to complement thumb opposition FCU = flexor carpi ulnaris, MCP = metacarpophalangeal, IP = interphalangeal (Continued) (Continued) Figure 4: Dissections of a right wrist. A, Dorsal view of a right wrist with the ECRL and ECRB reflected distally. The dorsal extrinsic wrist ligaments are identified. The DRC originates at the dorsal lip of the distal radius, adjacent to the dorsal radial tubercle (the Lister tubercle, designated by #). It traverses the radiocarpal joint obliquely to insert into the lunate and triquetrum. The DIC arises from the triquetrum and inserts into the capitate, the distal scaphoid, and the trapezoid. ERCL = extensor carpi radialis longus, ECRB = extensor carpi radialis brevis, DRC = dorsal radiocarpal ligament, DIC = dorsal intercarpal ligament. B, Dorsal view of a right wrist after resection of the extrinsic ligaments. The dorsal aspect of the TFCC, the dorsal radioulnar ligament, is visualized. The SLIL and LTIL stabilize the proximal carpal row. The capitate and hamate are identified in the distal carpal row. SLIL = scapholunate interosseous ligament, LTIL = lunotriquetral interosseous ligament, Cap = capitate, H = hamate. C, Dorsal view of the DRUJ. The distal ulna articulates with the distal radius at the DRUJ where the distal radial articular surface (sigmoid notch) has a greater radius of curvature than that of the unlar head. The DRUJ is constrained by the dorsal and volar (not shown) distal radioulnar ligaments. The distal radioulnar ligaments are components of the TFCC. The Lister tubercle (designated by #) is identified for reference. UH = ulnar head, US = ulnar styloid, dRUL = dorsal distal radioulnar ligament. D, End-on view of the articular surface of the right distal radius and the ulnocarpal joint with the carpus reflected palmarly and ulnarly. The SF and LF of the distal radius are separated by the scapholunate ridge. The volar extrinsic ligaments originate from the distal radius and include the RC, RSC, and RL ligaments. Components of the TFCC include the central meniscal homologue (TFCC), the dorsal and volar radioulnar ligaments (not shown), the UL, the UT, and the floor of the ECU sheath (not shown). SF = scaphoid facet, LF = lunate facet, RC = radial collateral ligament, RSC = radioscaphocapitate ligament, RL = radiolunate ligament, UL = ulnolunate ligament, UT = ulnotriquetral ligament. (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Table 6 Origins and Insertions of the Extrinsic Wrist Ligaments Ligament Origin Insertion Radial collateral Radius (0 mm from RS) Scaphoid waist and distal palmar trapezium Radioscaphocapitate Radius (4 mm from RS) Scaphoid waist and midpalmar capitate Radiolunatotriquetral Radius (10 mm from RS) Lunate +/- triquetrum Radioscapholunate Mesocapsule with termination of AIN and Ligament of Testut and Kuenz AIA Short radiolunate Volar-ulnar margin of radius Lunate Ulnotriquetral Volar radioulnar ligament Triquetrum Ulnolunate Volar radioulnar ligament Lunate Ulnocapitate Volar margin of the ulnar head Capitate Dorsal radiocarpal Dorsal radius at the Lister tubercle Lunate and triquetrum Dorsal intercarpal Triquetrum Scaphoid and trapezoid and capitate Volar Extrinsic, Radiocarpal Volar Extrinsic, Ulnocarpal Dorsal Extrinsic RS = radial styloid tip, AIN = anterior interosseous nerve, AIA = anterior interosseous artery Figure 5: Cross-sectional anatomy of the proximal third (A), middle third (B), and distal third (C) of the forearm. (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Table 7 Musculature of the Dorsal Forearm and Wrist Muscle Mobile Wad of Three Brachioradialis Origin Insertion Innervation Upper supracondylar ridge Radial styloid Base of the index finger metacarpal Radial nerve Extensor carpi radialis longus Lower supracondylar ridge Extensor carpi radialis brevis Lateral epicondyle, elbow capsule annular ligament Superficial Extensor Muscles Anconeus Post-lateral epicondyle Most medial common Extensor carpi ulnaris extensor superior ulnar border EDM Common extensor origin EDC Deep Extensor Muscles Common extensor origin Supinator Lateral epicondyle, annular ligament, lateral ulnar collateral ligament APL Radius EPB EPL EIP Interosseous membrane +/radius Ulna Ulna + interosseous membrane Radial nerve Base of the long finger metacarpal SBRN, 25% PIN, 45% Radial nerve, 30% Lateral-dorsal ulna Radial nerve Base of the small finger metacarpal PIN Small finger extensor apparatus Digital extensor apparatus Anterior proximal radius Thumb metacarpal base, trapezium thenar muscle (varies) Thumb proximal phalanx, extensor hood (varies) Thumb distal phalanx Index finger extensor apparatus PIN PIN PIN PIN PIN PIN PIN SBRN = superficial branch of the radial nerve, PIN = posterior interosseous nerve, EDM = extensor digiti minimi, EDC = extensor digitorum communis, APL = abductor pollicis longus, EPB = extensor pollicis brevis, EPL = extensor pollicis longus, EIP = extensor indicis proprius Table 8 Musculature of the Volar/Flexor Forearm and Wrist Muscle Origin Insertion Superficial Layer (all cross the elbow joint) Superficial head: distal 1 cm of supracondylar ridge plus medial epicondyle Pronator teres Midlateral radius Deep head: Medial coronoid distal to sublime tubercle† Base of the index and long finger metacarpals Palmar aponeurosis Innervation* Median nerve Flexor carpi radialis Medial epicondyle PL‡ Medial epicondyle Median nerve Medial epicondyle, sublime Base of P2 (fingers§) Median nerve tubercle, anterior radius Humeral head: medial Pisiform, pisohamate ligament, epicondyle Ulnar nerve pisometacarpal ligament Ulnar head: Posteromedial ulna FDS FCU Median nerve Deep Layer (none crosses the elbow joint) FDP FPL Pronator quadratus Anterior plus medial ulna, interosseous membrane Anterior radius, interosseous membrane Distal ulna Base of P3 (fingers) AIN, ulnar nerve Base of thumb P2 AIN Volar radius AIN * The median nerve may course distally between the FDS and the FDP; commonly within the FDS epimysium, and occasionally within the FDS substance. †The deep (ulnar) head of pronator teres separates the ulnar artery (deep) from the median nerve (superficial). It is absent in approximately 6% of wrists. ‡The palmaris longus is absent unilaterally in ~15% of wrists and bilaterally in 7%. §There is variable presence of the FDS to the small finger. PL = palmaris longus, FDS = flexor digitorum superficialis, FCU = flexor carpi ulnaris, FDP = flexor digitorum palmaris, AIN = anterior interosseous nerve, FPL = flexor pollicis longus Figure 6: Illustrations of the primary arterial anatomy of the upper extremity. A, Volar forearm, wrist, and hand. B, Dorsal forearm, wrist, and hand. (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Figure 7: Illustration of the brachial plexus (right). (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Figure 8: Illustration of the anatomic course and branches of the radial nerve in the right upper extremity. BR = brachioradialis, ECRL = extensor carpi radialis longus, ECRB = extensor carpi radialis brevis, ECU = extensor carpi ulnaris, EDC = extensor digitorum communis, EDM = extensor digitorum communis, APL = abductor pollicis longus, EPL = extensor pollicis longus, EPB = extensor pollicis brevis, EIP = extensor indicis proprius, PIN = posterior interosseous nerve. (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Figure 9: Illustration of the anatomic course and branches of the ulnar nerve in the right upper extremity. FCU = flexor carpi ulnaris, FDP = flexor digitorum profundus, FPB = flexor pollicis brevis, ADM = abductor digiti minimi, AdP = adductor pollicis, FDM = flexor digiti minimi, ODM = opponens digiti minimi. (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) Figure 10: Illustration of the anatomic course and branches of the median nerve in the right upper extremity. PT = pronator teres, FDS = flexor digitorum superficialis, FCR = flexor carpi radialis, FDP = flexor digitorum profundus, AIN = anterior interosseous nerve, PQ = pronator quadratus, FPB = flexor pollicis brevis, APB = abductor pollicis brevis, OP = opponens pollicis. (Copyright Fraser J. Leversedge, MD; Martin Boyer, MD, MSc, FRCSC; and Charles A. Goldfarb, MD.) A. B. C. D. E. Primary Osteoarthritis Erosive Osteoarthritis Pulmonary Hypertrophic Osteoarthropathy Posttraumatic Arthritis Rheumatoid Arthritis F. G. H. I. Systemic Lupus Erythematosus Psoriatic Arthritis Gout Calcium Pyrophosphate Deposition Disease (Pseudogout) Figure 1: Drawing showing positioning of the hand on the radiographic cassette for the hyperpronated view Table 1 Radiographic Staging* and Treatment of Thumb CMC Arthritis Stage 1 2 3 4 CMC Articular CMC Articular CMC Joint (Type Contour Space of Changes) Normal Normal Abnormal Abnormal Widened Mild subluxation CMC Scaphotrapezial Surgical Treatment† Osteophytes Joint None CMC synovectomy and débridement (arthroscopic) With joint laxity, ligament reconstruction (FCR tendon) None Arthroscopic débridement and tendon interposition Partial trapeziectomy with tendon interposition Complete trapeziectomy with ligament reconstruction and tendon interposition Trapeziometacarpal arthrodesis > 2 mm None Partial trapeziectomy with tendon interposition. Complete trapeziectomy with LRTI Trapeziometacarpal arthrodesis > 2 mm Pantrapezial arthrosis Arthroplasty Complete trapeziectomy with LRTI None Narrowing Mild subchondral < 2 mm sclerosis Narrowing Sclerotic or cystic changes in subchondral bone Narrowing Sclerotic or cystic changes in subchondral bone LRTI = ligament reconstruction and tendon interposition *As described by Eaton and Littler. †All stages are initially treated nonsurgically. Figure 2: AP radiograph of a stage II SLAC wrist. The capitate has migrated proximally, and joint space narrowing is seen between the radial styloid and the scaphoid as well as between the proximal pole of the scaphoid and the scaphoid fossa of the distal radius. Figure 3: AP radiograph of a SNAC wrist. Joint space narrowing is seen between the distal pole of the scaphoid and the radial styloid as well as between the distal pole of the scaphoid and the trapezium and trapezoid. Minimal joint space narrowing is seen between the proximal pole of the scaphoid and the scaphoid fossa of the distal radius. Table 2 Radiographic Staging of SLAC Wrist Stage Radiographic Signs Treatment I Arthrosis localized to the radial side of the Radial styloidectomy plus scapholunate reduction and scaphoid and the radial styloid. Sharpening stabilization of the radial styloid Elimination of radioscaphoid joint by: 1. Proximal row carpectomy; disadvantages: reduction of wrist motion and grip strength; should be avoided if there are capitate head degenerative changes 2. 2. Four corner (lunate, capitate, hamate, triquetrum) fusion (SLAC procedure). Retains 60% of wrist motion and 80% of grip strength 3. 3. Other: Radioscapholunate fusion, total wrist arthrodesis, total wrist arthroplasty II Arthrosis of the entire radioscaphoid joint. (The radiolunate joint is usually spared.) III Arthrodesis progressing to the capitolunate 1. SLAC procedure, PRC joint due to proximal migration of the 2. Total wrist arthrodesis (ideal position is 10° of extension and capitate slight ulnar deviation) PRC = proximal row carpectomy Table 3 Radiographic Staging of SNAC Wrist Stage I II III Radiographic Signs Treatment Arthrosis between the distal scaphoid and radial styloid. Radial styloidectomy plus fixation of scaphoid nonunion with bone graft SLAC procedure Scaphocapitate arthrosis in addition to stage Proximal row carpectomy I (proximal scaphoid and corresponding Total wrist arthrodesis radial articular surface spared) Total wrist arthroplasty SLAC procedure Periscaphoid arthrosis (proximal lunate and Total wrist arthrodesis captiate may be preserved) Total wrist arthroplasty Table 4 Ulnar Variance and Load Sharing Across Wrist Ulnar Variance Load Sharing + 2 mm 60% radius, 40% ulna + 1 mm 70% radius, 30% ulna Neutral 80% radius, 20% ulna − 1 mm 90% radius, 10% ulna − 2 mm 95% radius, 5% ulna Table 5 Table 6 Treatment of RA Affecting the Extensor Tendons Treatment of RA Affecting the Flexor Tendons Condition Treatment Condition/Symptoms Treatment Radial deviation and supination of the carpus only ECRL to ECU transfer Nerve compression symptoms Synovectomy with carpal tunnel release Triggering Distal radioulnar joint arthrosis Distal ulna resection (Darrach procedure, hemiresection, or Sauvé-Kapandji procedure) Synovectomy with resection of FDS slip FPL rupture FDS transfer or tendon graft with spur excision FPL rupture with advanced disease Thumb IP joint arthrodesis FDS ruptures in digits Observation FDP ruptures in digits Synovectomy and DIP joint arthrodesis Caput ulna syndrome EIP to EDQ transfer or EDQ to EDC piggyback transfer Multiple tendon ruptures FDS transfer or palmaris graft ECRL = extensor carpi radialis longus, ECU = extensor carpi ulnaris, EIP = extensor indicis proprius, EDQ = extensor digitorum quinti, FDS = flexor digitorum sublimis. FPL = flexor pollicis longus, FDS = flexor digitorum sublimis, FDP = flexor digitorum profundis. Figure 4: The pathoetiology of rheumatoid carpal deform-ity: scaphoid flexion, scapholunate widening, lunate translocation, and secondary radioscaphoid arthrosis combined with ulnar drift of the digital MCP joints. (Courtesy of the Indiana Hand Center, © Gary Schnitz, 2007.) Table 7 Table 8 Treatment of RA Affecting the Wrist Treatment of RA Affecting the MCP Joint Severity of Disease/Patient Characteristics Treatment Midcarpal joint well preserved Partial arthrodesis (radiolunate or scaphoradiolunate) Advanced disease Total wrist arthrodesis Sedentary patient with good bone stock Total wrist arthroplasty Severity of Disease Treatment Early stages Medical Ulnar drift with preservation of articular surface Soft-tissue realignment procedures (extensor relocation, intrinsic release, collateral ligament reefing) Severe joint involvement, fixed deformities, or arthritis— cartilage loss MCP joint arthroplasty Thumb MCP joint involvement Arthrodesis Thumb MCP joint involvement with IP joint involvement Arthroplasty Figure 5: Swan-neck deformity. A, Terminal tendon rupture may be associated with synovitis of the DIP joint, leading to DIP joint flexion and subsequent PIP joint hyperextension (a). Rupture of the flexor digitorum superficialis tendon may occur due to infiltrative synovitis which may lead to decreased volar support of the PIP joint and subsequent hyperextension deformity (b). B, Lateral-band subluxation dorsal to the axis of rotation of the PIP joint (c), contraction of the triangular ligament (d), and attenuation of the transverse retinacular ligament (e) are depicted. (Reproduced from Boyer MI, Gelberman RH: Operative correction of swan-neck and boutonniere deformities in the rheumatoid hand. J Am Acad Orthop Surg 1999;7:95.) Figure 6: Boutonniere deformity. Primary synovitis of the PIP joint (a) may lead to attenuation of the overlying central slip (b) and dorsal capsule and increased flexion at the PIP joint. Lateral-band subluxation volar to the axis of rotation of the PIP joint (c) may lead in time to hyperextension. Contraction of the oblique retinacular ligament (d), which originates from the flexor sheath and inserts into the dorsal base of the distal phalanx, may lead to extension contracture of the DIP joint. (Reproduced from Boyer MI, Gelberman RH: Operative correction of swan-neck and boutonniere deformities in the rheumatoid hand. J Am Acad Orthop Surg 1999;7:98.) Table 9 Treatment of Boutonniere Deformity Type of Deformity Treatment Passively correctable Splinting Moderate Extensor reconstruction (central slip imbrication, Fowler distal tenotomy) Stiff contracture PIP joint arthrodesis or arthroplasty Table 10 Treatment of Gout Condition Treatment Acute disease Colchicine or indomethacin Large gouty tophi are surgically excised. Severely involved joints treated with arthrodesis Chronic disease Allopurinol Large gouty tophi Surgical excision Severely involved joints Arthrodesis Benign Soft-Tissue Tumors B. Benign Bone Tumors C. Malignant Soft-Tissue Tumors D. Malignant Bone Tumors A. Figure 1: A, Axial T1-weighted MRI scan of the hand of an elderly man shows a large, multilobulated, soft-tissue mass involving the thenar space, as well as both the flexor and extensor compartments with communication through the interosseous ligaments between the third and fourth metacarpals. The areas of high signal intensity (arrows) are diagnostic for lipoma. B, Diagram of same cross section shown in A with structures labeled. (Reproduced from Johnson TR, Steinbach LS [eds]: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, p 159.) Figure 2: Oblique (left) and AP (right) views (A) and lateral oblique view (B) of the hand of a 22-year-old woman who presented with pain in the hand following a punch to an inanimate object. Lucency in the fifth metacarpal is welldefined and is a classic characteristic of an enchondroma. (Reproduced from Bedi A, Beirmann JS: Hand tumors, in Schwartz HS [ed]: Orthopaedic Knowledge Update: Musculoskeletal Tumors 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, p 31.) A. B. C. D. E. Anatomy of the Brachial Plexus Classification of Injuries Mechanism of Injuries Clinical Examination Electrodiagnostic Evaluation F. G. H. I. J. Imaging Evaluation Determinants of Treatment Treatment Treatment Based on Type of Injuries Rehabilitation Figure 1: Anatomy of the brachial plexus roots and types of injury. The roots are formed by the coalescence of the ventral (motor) and dorsal (sensory) roots as they emerge from the spinal cord. The dorsal root ganglion holds the cell bodies of the sensory nerve fibers conveyed by the dorsal root, whereas the cell bodies for the ventral nerve fibers lie within the spinal cord. Three types of injury can occur: avulsion (top right) injuries pull the rootlets out of the spinal cord; stretch injuries (middle right) attenuate the nerve; and ruptures (bottom right) result in a complete discontinuity of the nerve. (Reproduced with permission from the Mayo Foundation for Medical Education and Research.) Figure 2: Classic form of the brachial plexus. (Reproduced with permission from the Mayo Foundation for Medical Education and Research.) Table 1 Frequency of BPI by Anatomic Level Location of Lesion Frequency (%) Supraclavicular 62 Supraclavicular + distal 9 Retroclavicular 7 Retroclavicular + distal 1 Infraclavicular 20 Infraclavicular + distal 1 Figure 3: Myelography and CT myelography can be instrumental in determining the level of nerve injury. If a pseudomeningocele is present, there is a greater likelihood of a nerve root avulsion. A, A myelogram demonstrates multiple root avulsions. The asterisks indicate pseudomeningoceles. B, CT provides further evaluation of the injury. The arrows point to the nerve roots visible within the thecal sac on the side opposite the pseudomeningocele. (Reproduced with permission from the Mayo Foundation for Medical Education and Research.) Relevant Anatomy and Disease Patterns B. Pathology C. Epidemiology D. Treament E. Complications A. Figure 1: Normal fascial anatomy of the palm and digits, illustrating relationships to the tendon sheath and neurovascular bundles. Figure 2: Patterns of diseased cords. The spiral cord (derived from the pretendinous band, spiral band, Grayson ligament, and lateral digital sheet) displaces the neurovascular bundle toward the midline. The Grayson ligment is seen as an isolated thickened structure. The lateral cord comes off the natatory cord to merge with the lateral digital sheet along the midaxial line. Figure 3: The retrovascular cord arises from the preaxial phalanx and courses dorsal to the neurovascular bundle to insert in the side of the distal phalanx. It is the usual cause of DIP joint contractures. A. B. C. D. Basic Science of Flexor and Extensor Tendons Diagnosis of Tendon Disruption Primary Repair of Injured Flexor Tendons Primary Management of Extensor Tendon Injuries E. F. G. H. Tendon Repair Complications Tendon Reconstruction Late Complications After Tendon Injury and Repair Conditions Involving Tendinitis Figure 1 : Lateral (A) and dorsal (B) views of a finger depict the components of the digital flexor sheath. The sturdy annular pulleys (A1, A2, A3, A4, and A5) keep the tendons closely applied to the phalanges. The thin, pliable cruciate pulleys (C1, C2, and C3) collapse to allow digital flexion. The palmar aponeurosis pulley (PA) adds to the biomechanical efficiency of the pulley system. (Reproduced from Strickland JW: Flexor tendon injuries: I. Foundation of treatment. J Am Acad Orthop Surg 1995;3:44-54.) Figure 2 : Finger extensor mechanism anatomy. A, Lateral view. B, Dorsal view. DIP = distal interphalangeal joint, MCP = metacarpophalangeal joint, ORL = oblique retinacular ligament, PIP = proximal interphalangeal joint, TRL = transverse retinacular ligament. (Adapted with permission from Coons MS, Green SM: Boutonniere deformity. Hand Clin 1995;11:387-402.) Figure 3: The five zones of flexor tendon injury. Note the three zones of the thumb. (Copyright Fraser J. Leversedge, MD, Martin Boyer, MD, MSc, FRCSC, and Charles A. Goldfarb, MD.) Figure 4: The extensor tendon zones of injury. (Reproduced from Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.) Pathophysiology B. Evaluation C. Management D. Late Effects A. A. B. C. D. E. F. Fingertip Infections Septic Flexor Tenosynovitis Septic Arthritis Osteomyelitis Human Bite Wounds Animal Bite Wounds G. H. I. J. K. Deep-Space Infections Uncommon Infections Conditions Often Mistaken for Infections Immunocompromised Patients Drug Principles A. B. C. D. Peripheral Nerve Anatomy and Physiology Basic Science of Nerve Compression Electrophysiology Common Compression Neuropathies E. F. G. Radial Nerve Compression Syndromes Thoracic Outlet Syndrome Neuropathies of the Shoulder Figure 1 : Clinical photograph of a patient with anterior interosseous nerve compression or paralysis. Note the inability to flex at the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. (Reproduced from Rizzo M, Cooney WP, Carlson HL, Mays W: Hand and wrist reconstruction, in Fischgrund JS [ed]: Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 357-376.) Figure 2 : Intraoperative photograph showing a ganglion in the ulnar tunnel causing isolated compression of the motor branch of the ulnar nerve. (Reproduced from Rizzo M, Cooney WP, Carlson HL, Mays W: Hand and wrist reconstruction, in Fischgrund JS [ed]: Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 357-376.) History B. Indications and Contraindications C. Pediatric Replantations D. Considerations by Level E. Critical Points in Replantation A. Table 1 Kay, Werntz, and Wolff Classification of Ring Avulsion Injuries Injury Type Characteristics Class I Circulation adequate Class II Arterial compromise only Class III Inadequate circulation, with bone, tendon, or nerve injury Class IV Complete degloving or amputation Overview B. Types of Coverage C. Coverage for Common Defect Sites D. Muscle Flap of Lower Extremity E. Soft-Tissue Defects F. Bone Flaps G. Tissue expansion A. Table 1 The Reconstructive Ladder Primary closure Healing by secondary intention Split-thickness skin grafts Full-thickness skin grafts Random pattern local flaps Axial pattern local flaps Island pattern local flaps Distant random pattern flaps Distant axial pattern flaps Free tissue transfer General Information B. Ulnar Artery Thrombosis C. Buerger Disease (Thromboangiitis Obliterans) A. Figure 1: Palmar view of the vascular anatomy of the forearm and hand. Introduction B. Conditions Treated With Arthroscopy C. Patient Setup D. Portals E. Complications A. Table 1 Palmer Classification of Type 1 (Acute) TFCC Tears Class Location Characteristics 1A Central Traumatic tears of articular disk 1B Ulnar Ulnar avulsion 1C Volar distal Distal traumatic disruption of the ulnolunate or ulnotriquetral ligaments 1D Radial Traumatic avulsion from sigmoid notch of radius Figure 1: The standard wrist arthroscopy portals.