Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Prenatal development wikipedia , lookup
Umbilical cord wikipedia , lookup
Anatomical terminology wikipedia , lookup
Anatomical terms of location wikipedia , lookup
Large intestine wikipedia , lookup
Acute liver failure wikipedia , lookup
Drosophila embryogenesis wikipedia , lookup
Human embryogenesis wikipedia , lookup
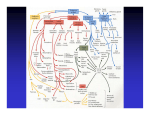
Digestive System • Primitive gut (PG) develops I0 from endoderm – PG ⇒ digestive system • Dorsal part of the yolk sac is incorporated into embryo as the PG due to formation of head, tail & lateral folds during 4th week – Endoderm gives rise to most of epithelium of the digestive tract & parenchyma of its associated glands • Liver & pancreas – Ectoderm of stomodeum (primitive mouth)⇒ epithelium at the superior end of digestive tract – Ectoderm of proctodeum (anal pit)⇒ epithelium at the inferior end of the digestive tract Digestive tract • Connective tissue & muscles in the wall of the digestive tract are derived from splanchnic mesenchyme that surrounds the endodermal primitive gut (PG) • PG is divided into four parts – Pharynx – Foregut – Midgut – hindgut Pharynx • Supported by pharyngeal/branchial arches – Series of paired sacculations in lateral walls ⇒ Pharyngeal pouches • By the end of the 4th week five pairs have formed Pharyngeal Pouches • First pharyngeal pouch – Enlarges & develops into a tubotympanic recess • This will become the auditory tube & tympanic cavity (middle ear) • Second pharyngeal pouch – Remains small & is largely obliterated as palatine tonsil develops • Endodermal cells form surface epithelium of tonsil & lining of its crypts • Mesenchyme around this pouch differentiates into lymphoid tissue Pharyngeal Pouches (cont.) • Third pharyngeal pouch – Dorsal endoderm ⇒ inferior parathyroid glands – Ventral endoderm unite to form thymus – Both glands lose connection with pharynx & migrate in a caudal & medial direction • Fourth pharyngeal pouch – Dorsal endoderm ⇒ superior parathyroid glands • Fifth pharyngeal pouch (part of fouth) – Ultimobranchial body which incorporates into thyroid gland • These cells give rise to parafollicular/C cells & secrete calcitonin Foregut • Lies caudal to pharyx & extends as far back as the liver outgrowth • At about 4 weeks a small diverticulum appears in ventral wall at caudal border – Tracheobonchiole/respiratory diverticulum • Gradually separates from foregut dividing foregut – Dorsal esophagus – Ventral respiratory primordium Foregut • Esophagus – Tube extending from pharynx to stomach • Initially short but elongates rapidly keeping pace with differentiating neck & descending heart & lungs Foregut • Stomach – Fusiform dilatation in 4th week of development – During the following weeks appearance & position changes (descends) • Increases in length • Dorsal border grows faster than ventral wall + 90o CW rotation along its long axis – Posterior faces left, Anterior faces right – Convex greater curvature (GC) ⇒ lies on left – Concave lesser curvature (LC) ⇒ lies on right – Epithelium differentiates into gastric glands & surrounding mesenchyme • Three incomplete layers of the muscular coat Foregut • Duodenum – Develops early in 4th week from caudal part of foregut & cephalic part of midgut • Junction of two parts directly distal to origin of liver bud – Takes form of C shape loop & rotates to right as stomach rotates • Duodenal rotation along with rapid growth of head of the pancreas causes swing to left side of abdomen – During 2nd month the lumen is obliterated by cell proliferation but recanalized shortly after Foregut • Liver & gallbladder – Liver primordium appears in middle of 3rd week as hepatic diverticulum (HD) or liver bud at distal end of foregut • Hepatic diverticulum rapidly enlarges due to cell proliferation dividing into a large & small part – Large cranial part ⇒ liver primordium – Small caudal part ⇒ gallbladder primordium – Hepatic cells continue to divide, the connection between the HD & duodenum narrows ⇒ bile duct Liver (cont.) • Epithelial hepatic cell cords intermingle with vitelline & umbilical veins ⇒ Hepatic sinusoids • Liver grows rapidly & fills most of abdominal cavity – Initially right & left lobe are = size • Right lobe becomes larger & subdivides into caudate & quadrant lobes – At 9th week 10% of fetal body weight – At full term 5% of fetal body weight Gallbladder & Pancreas • Gallbladder primordium – Distal end expands ⇒ gallbladder – Proximal part stays narrow ⇒ cystic duct • Pancreas formed by two buds originating from endodermal lining of duodenum – Buds arise on opposite sides at end of 4th week • Dorsal pancreas ⇒ forms most of the gland – Pushes out from dorsal wall slightly above hepatic diverticulum • Ventral pancreas ⇒ head & uncinate process – Develops near entry of bile duct – Main pancreatic duct • Formed by distal part of dorsal duct + entire ventral duct Midgut • In a 4-5 week old embryo midgut is suspended from dorsal abdominal wall by a short mesentery & communicates with the yolk sac via vitelline duct • Will give rise to: – Part of duodenum & rest of the small intestine • Distal to where the bile duct enters – Ceacum – Appendix – Ascending colon – Proximal 2/3 of transverse colon Midgut (cont.) • All structures of midgut supplied by superior mesenteric artery • Development is characterized by a rapid growth in the length of the gut ⇒ formation of primary intestinal loop – Cranial limb • Part of duodenum, jejunum, part of ileum – Caudal limb • Balance of ileum to proximal 2/3 of transverse colon – Vitelline duct • At junction of cranial & caudal limb • If it persists in adult ⇒ Meckel’s diverticulum Midgut (cont.) • As the intestinal loop elongates rapidly & liver enlarges, the abdominal cavity is temporally too small causing intestinal loop to project into the umbilical cord ⇒ physiological umbilical hernia (starting around the 6th week) – By about the end of the 3rd month the herniated loops begin to return to the abdominal cavity Hindgut • Gives rise to: – – – – – distal 1/3 of transverse colon the descending colon the sigmoid colon the rectum upper part of anal canal • All hindgut derivatives are supplied by the inferior mesenteric artery • The terminal portion = cloaca – Cloacal membrane • lined with endodermal cells internally • Lined with ectodermal cells externally Congenital Malformations • • • • • • • • Branchial Anomalies Esophageal Atresia Esophageal stenosis Short esophagus Intestinal stenosis & atresia Omphalocoele Umbilical hernia Meckel’s Diverticulum Branchial Anomalies • Most of the abnormalities of the branchial region are represented by remnants of the branchial structures that normally disappear – Branchial fistula • An abnormal opening on the side of the neck – Usually the result of persistance of parts of 2nd branchial groove & 2nd branchial pouch – Agenesis of thyroid & parathyroid • • • • DiGeorge Syndrome Failure of 3rd & 4th pharyngeal pouches to differentiate May be due to teratogen action No known genetic cause Esophageal Atresia • Usually occurs with tracheo-esophageal fistula (TEF) • Several types – Lower esophagus communicates with back of trachea & upper esophagus ends in a blind pouch ( most common) – Discontinuous esophagus with no tracheoesophageal fistula (rare) • Possibly genetic • Possible maternal vitamin A deficiency Congenital Esophageal Stenosis • Rarer than esophageal atresia with TEF • Little known etiology • Symptoms – Regurgitation of food – Failure to gain weight – Dilation of esophagus above level of obstruction may press against the trachea & bronchi ⇒ produce wheezing sounds Congenital Malformations (cont.) • Short esophagus – Causes partial thoracic stomach • Small portion of stomach above diaphragm • Gastroesophageal incompetence is a common cause of vomiting (often projectile) during infancy • Intestinal stenosis & atresia – Occurs commonly in duodenum & ileum – May be due to interruption of blood supply to a loop of fetal intestine • Results in necrosis, which later becomes fibrous cord connecting proximal & distal ends Congenital Malformations (cont.) • Omphalocoele – Results from failure of intestine to return to abdomen during 10th week – Hernia may contain a single loop of intestine or most of the intestine • Herniated mass is covered by a thin transparent membrane composed of peritoneum & amnion – Associated with chromosome abnormalities & other severe defects • Umbilical hernia – Differs from omphalocoele • herniated mass is covered by skin & subcutaneous tissue Congenital Malformations (cont.) • Gastroschisis – Herniation of abdominal contents through the body wall directly into the amniotic cavity • Defect occurs lateral to umbilicus, usually on the right, through a region weakened by regression of the right umbilical vein which normally disappears – Viscera are not covered by peritoneum or amnion • Bowel may be damaged by exposure to amniotic fluid – 1 in 10,000 births (frequency is ⇑) • May be related to cocaine use Congenital Malformations (cont.) • Meckel’s Diverticulum – Ileal diverticulum is common – Higher frequency among males – Represents remnant of the vitelline duct – Appears as finger-like pouch arising from ileum – 3-6 cm long & may remain connected to umbilicus by a fibrous cord or fistula – Wall of diverticulum contains all tissue layers of the ileum • May include gastric & pancreatic tissue • Gastric secretion often produces ulceration