Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Echocardiography wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
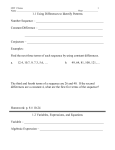
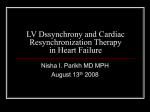
Journal of the American College of Cardiology © 2005 by the American College of Cardiology Foundation Published by Elsevier Inc. Vol. 46, No. 12, 2005 ISSN 0735-1097/05/$30.00 doi:10.1016/j.jacc.2005.05.095 FOCUS ISSUE: CARDIAC RESYNCHRONIZATION THERAPY CLINICAL RESEARCH Resynchronization and M-Mode Echo Septal to Posterior Wall Motion Delay Fails to Predict Reverse Remodeling or Clinical Improvement in Patients Undergoing Cardiac Resynchronization Therapy Gregory M. Marcus, MD,* Emily Rose, MD,† Esperanza M. Viloria, BS,* Jill Schafer, MS,‡ Teresa De Marco, MD, FACC,* Leslie A. Saxon, MD, FACC,§ Elyse Foster, MD, FACC,* for the VENTAK CHF/CONTAK-CD Biventricular Pacing Study Investigators San Francisco and Los Angeles, California; Boston, Massachusetts; and St. Paul, Minnesota The aim of this study was to test the hypothesis that a longer septal-to-posterior wall motion delay (SPWMD) would predict greater reverse remodeling and an improved clinical response in heart failure patients randomized to cardiac resynchronization therapy (CRT) in the CONTAK-CD trial. BACKGROUND The SPWMD predicted clinical benefit with CRT in two previous studies from the same center. METHODS In this retrospective analysis of the CONTAK-CD trial, SPWMD was measured from the baseline echocardiogram of 79 heart failure patients (ejection fraction 22 ⫾ 7%, QRS duration 159 ⫾ 27 ms, 72% ischemic, 84% male) randomized to CRT and compared with six-month changes in echocardiographic and clinical parameters. Patients with a left ventricular end-systolic volume index (LVESVI) reduction of at least 15% were considered responders. RESULTS The feasibility and reproducibility of performing the SPWMD measurements were poor. Larger values for SPWMD did not correlate with six-month changes in left ventricular end-diastolic volume index (p ⫽ 0.26), LVESVI (p ⫽ 0.41), or left ventricular ejection fraction (p ⫽ 0.36). Responders did not have a significantly different SPWMD than non-responders (p ⫽ 0.26). The SPWMD did not correlate with measures of clinical improvement. At a threshold of SPWMD ⬎130 ms, the test characteristics to predict reverse remodeling or a clinical response were inadequate. CONCLUSIONS The previous findings that SPWMD predicts reverse remodeling or clinical improvement with CRT were not reproducible in patients randomized in the CONTAK-CD trial. (J Am Coll Cardiol 2005;46:2208 –14) © 2005 by the American College of Cardiology Foundation OBJECTIVES Intraventricular conduction delay, primarily in the form of left bundle-branch block, is present in approximately 25% of heart failure patients (1). The resultant delayed and dyssynchronous left ventricular (LV) contraction worsens ventricular function and results in increased myocardial oxygen demand, ventricular remodeling, and increased mortality (2– 4). By simultaneously stimulating the right ventricle and the free wall of the LV, cardiac resynchronization therapy (CRT) has been shown to decrease LV volumes and dimensions, From *Department of Medicine, Division of Cardiology, University of California, San Francisco, San Francisco, California; †Department of Medicine, Brigham and Women’s Hospital, Boston, Massachusetts; ‡Guidant Corporation, St. Paul, Minnesota; and §Department of Medicine, Division of Cardiology, University of Southern California, Los Angeles, California. Drs. DeMarco and Foster received grants from Guidant Corporation. Dr. Saxon consults for and receives grants from Guidant Corporation, Medtronic, and St. Jude Corporations. Ms. Schafer is an employee of Guidant Corporation. The first two authors contributed equally to this paper. Manuscript received March 1, 2005; revised manuscript received May 8, 2005, accepted May 15, 2005. increase ejection fraction, and improve functional status in some, but not all patients with severe LV systolic dysfunction, interventricular conduction delay, and symptomatic heart failure (5,6). In previous studies, a greater degree of electrical and mechanical dyssynchrony at baseline have been associated with greater likelihood of improvement in LV structure and function with CRT (7,8). Current inclusion criteria for CRT devices use only the QRS duration to assess dyssynchrony. Given the costs and risks associated with CRT, identifying reliable non-invasive measures of ventricular dyssynchrony that predict therapeutic benefit are needed to optimize patient selection. In a non-randomized study of 20 CRT patients with predominantly non-ischemic cardiomyopathy, it was demonstrated that septal-to-posterior wall motion delay (SPWMD) measured by M-mode echocardiography was a useful predictor of reverse remodeling (9). More recently, a study of 60 CRT patients from the same center demonstrated that the SPWMD was useful to predict heart failure progression. JACC Vol. 46, No. 12, 2005 December 20, 2005:2208–14 Abbreviations and Acronyms CRT ⫽ cardiac resynchronization therapy LV ⫽ left ventricle/ventricular LVEDVI ⫽ left ventricular end-diastolic volume index LVEF ⫽ left ventricular ejection fraction LVESVI ⫽ left ventricular end-systolic volume index NYHA ⫽ New York Heart Association SPWMD ⫽ septal-to-posterior wall motion delay In both studies, a longer SPWMD was associated with greater improvement with CRT, and a SPWMD ⱖ130 ms was found to be a useful cutoff point to predict success. Based on these results, SPWMD has been suggested as a screening method for patient selection for CRT. However, the feasibility and utility of this parameter have not been tested in a largely ischemic population in whom endocardial excursion of either the septal or posterior wall may be markedly diminished and therefore not clearly identifiable. This study was designed to test the hypothesis that SPWMD would predict greater reverse remodeling and an improved clinical response in heart failure patients randomized to CRT in the CONTAK-CD trial. METHODS Subjects. The VENTAK CHF/CONTAK-CD study enrolled 581 patients from 47 investigational centers throughout the U.S. from February 1998 through December 2000. The study was approved by the institutional review board at each participating institution, and patients gave written informed consent. Inclusion criteria were an indication at the time of enrollment for an implantable cardioverter defibrillator, symptomatic heart failure despite optimal drug therapy, left ventricular ejection fraction (LVEF) ⱕ35%, a QRS duration ⱖ120 ms; age ⱖ18 years, and normal sinus node function. The exclusion criteria and study design have been described in a previous publication (5). Originally, all patients received a CRT device and were randomized to CRT turned on or to CRT turned off (phase 1, n ⫽ 248). Because of regulatory concern, the study was modified from a crossover to a six-month parallel design in phase 2 (n ⫽ 333). Of the 581 patients enrolled between the two phases, 501 were successfully implanted with the investigational system (5). Only phase 2 patients randomized to CRT turned on with paired baseline and six-month echo data are included in this analysis. Echocardiographic analysis. Two-dimensional Doppler echocardiograms were performed at multiple investigational sites according to a standardized protocol at baseline, three months, and six months after randomization. For the purposes of this study, the baseline and six-month echocardiograms were analyzed. A two-dimensionally guided (Mmode) echocardiogram at a level just below the tips of the mitral leaflets, basal to the tips of the papillary muscles, was used for measurement of the SPWMD as described subsequently. Left ventricular end-diastolic volumes and LV end- Marcus et al. SPWMD Fails to Predict CRT Outcomes 2209 systolic volumes were obtained by tracing the endocardium at the end-diastole (maximum cavity dimension) and endsystole (frame before mitral valve opening or the minimum cavity area) in the two-chamber and four-chamber views and derived according to Simpson’s rule (biplane method of discs) (10). The left ventricular end-systolic volume index (LVESVI) and left ventricular end-diastolic volume index (LVEDVI) are normalized for body surface area. The LVEF was calculated as the total stroke volume divided by the end-diastolic volume. Echocardiograms were excluded when less than 80% of the endocardium could be visualized. Responders were defined as those who had greater than a 15% decrease in LVESVI (9,11). Clinical improvement measures included six-month change in peak exercise O2 consumption, 6-min walk distance, quality of life score as assessed by the Minnesota Living with Heart Failure Questionnaire, and New York Heart Association (NYHA) functional class. The SPWMD represents the delay between the motion of the septum and the posterior wall of the LV. We adopted the method described by Pitzalis et al. (9) and measured the SPWMD on the M-mode echocardiogram obtained at baseline before randomization: the maximum displacement of the septal wall and the maximum displacement of the posterior wall were both measured from the onset of the QRS; the QRS to septal wall deflection value was then subtracted from the QRS to posterior wall deflection value to calculate the SPWMD (Fig. 1). Three measurements were made for each parameter and then averaged. These measurements were performed for each subject by two independent observers for 60% of the subjects for the primary and first observer and 47% of the subjects for the primary and second observer. In adopting this method, we recognize that the level of M-mode echocardiogram differs from the original description (9): Pitzalis obtained the M-mode at the level of the papillary muscles. In contrast, the measurements for the present study were made at a more basal level, representing the standard location for measuring LV dimensions. The ability to accurately measure SPWMD on the M-mode tracing was highly dependent on the extent of excursion of the septal and posterior walls. Therefore, a scale of difficulty was created. A value of one was given if both the septal wall and the posterior wall deflection were easily visualized. A value of two was given if either the septal or posterior wall displacement was difficult to visualize. A value of three was given if both the septal and posterior wall were difficult to visualize or if either one had no identifiable deflection. Operators blinded to the success of resynchronization therapy for the individual patients performed the echocardiographic analysis of intraventricular dyssynchrony. Interobserver reliability was measured with two independent observers compared with the primary observer. Statistical analysis. Linear comparisons between SPWMD and LVESVI, LVEDVI, and LVEF were made by calculating the Pearson product-moment correlation coefficient. 2210 Marcus et al. SPWMD Fails to Predict CRT Outcomes JACC Vol. 46, No. 12, 2005 December 20, 2005:2208–14 Figure 1. Septal wall motion delay (SWMD) was measured in M-mode by measuring from the start of the QRS to the peak of the septal wall deflection. Posterior wall motion delay (PWMD) was measured similarly by measuring from the start of the QRS to the peak of the posterior wall deflection. The difference between the septal wall deflection and the posterior wall deflection is the septal-to-posterior wall motion delay (SPWMD). Differences in categorical and continuous variables between responders and non-responders were assessed by the chisquare test or Student t test, as appropriate. In addition, six-month change in peak exercise O2 consumption, 6-min walk distance, quality of life score, and NYHA functional class were correlated with all dyssynchrony parameters. To reveal whether patients with longer baseline SPWMD measurements experienced a significantly greater improvement in LVESVI, LVEDVI, and LVEF with CRT than other patients, linear regressions with respect to these variables and their effect on treatment group were performed. To be consistent with previous studies, a SPWMD value ⱖ130 ms was used to determine the sensitivities, specificities, and positive and negative predictive values for six-month improvement in echocardiographic and clinical parameters (8,9). In determining associations between patients with and without a SPWMD ⱖ130 ms and clinical outcomes, continuous measures were calculated from a Student t test and values for categorical measures were calculated by a chi-square test. Within-subjects standard deviation was calculated using the analysis of variance between the two independent observers and compared with the primary observer, and repeatability of measurements was calculated by multiplying the withinsubjects standard deviation by 2.77 to account for 2 SD from the mean and two independent measurements of the same value (12–14). RESULTS Of the 333 subjects randomized to CRT in the CONTAK-CD trial, six-month echocardiograms were available for 79 (24%) (Table 1). Compared with subjects for whom six-month echocardiograms were not available, those with both baseline and six-month echocardiograms had no significant differences in regard to gender, etiology of heart failure, QRS duration, and ejection fraction (Table 1). Subjects for whom six-month echocardiograms were not available were less likely to be taking a beta-blocker and were less likely to have a lateral lead location. Feasibility of the SPWMD measurements. A definitive systolic deflection of both the septal and posterior walls was evident in less than half of all subjects (45%). According to the difficulty scale, the number of patients in each category was: 1 (n ⫽ 39), 2 (n ⫽ 27), and 3 (n ⫽ 13). The level of difficulty scale did not influence relationships between dyssynchrony parameters and CRT benefit in any category. Reproducibility of SPWMD measurements. There was poor inter-observer precision of SPWMD (observer 1 with the primary observer ⫽ 141 ms, n ⫽ 37; observer 2 with the primary observer ⫽ 194 ms, n ⫽ 47). For example, the within-subjects standard deviation for SPWMD between observer 1 and the primary observer was 51 ms, yielding a repeatability of 141 ms. These suggest that 95% of pairs of measurements of the same echocardiographic parameter by different observers should fall between 141 ms. Correlations between baseline SPWMD and six-month evidence of reverse remodeling. The reduction in LVESVI and LVEDVI and the improvement in ejection fraction were determined by comparing the baseline and six-month echocardiograms. Baseline SPWMD did not correlate with six-month changes in LVESVI (⫺0.10, p ⫽ 0.41), LVEDVI (⫺0.14, p ⫽ 0.26), or ejection fraction (0.11, p ⫽ 0.36). Correlations remained non-significant when examining the same echocardiographic parameters in patients with and without ischemic etiologies of heart failure. The baseline SPWMD did not significantly differ between responders (mean 77 ⫾ 141 ms, range ⫺340 ms to 312 ms) and non-responders (mean 59 ⫾ 160, range ⫺326 ms to 525 ms, p ⫽ 0.63). The lack of any relationship between baseline SPWMD and responders persisted when examining patients with ischemic etiologies of heart failure alone or non-ischemic etiologies of heart failure alone. Pa- Marcus et al. SPWMD Fails to Predict CRT Outcomes JACC Vol. 46, No. 12, 2005 December 20, 2005:2208–14 Table 1. Baseline Characteristics: Patients With and Without Paired Six-Month Echocardiograms Characteristic Age at implant (yrs) n Mean ⫾ SD Range Gender, n (%) Male Female NYHA funtional class, n (%) II III IV Concomitant medications, n (%) ACE or ARB Beta-blocker Digoxin Diuretic Qualifying LVEF (%) n Mean ⫾ SD Range PR interval (ms) n Mean ⫾ SD Range Qualifying QRS duration (ms) n Mean ⫾ SD Range Resting heart rate, beats/min n Mean ⫾ SD Range Systolic blood pressure (mm Hg) n Mean ⫾ SD Range Diastolic blood pressure (mm Hg) n Mean ⫾ SD Range Primary tachyarrhythmia, n (%) Monomorphic VT Polymorphic VT Nonsustained VT Ventricular fibrillation Other arrhythmias, n (%) Paroxysmal atrial fibrillation Atrial flutter Conduction disorder, n (%) LBBB RBBB Non-specific Etiology of heart failure, n (%) Ischemic Non-ischemic Paired Echo No Paired Echo p (n ⴝ 79) (n ⴝ 69) Value 79 66.8 ⫾ 1.2 26.1–82.5 169 65.6 ⫾ 10.1 28.9–82.6 66 (83.5) 13 (16.5) 144 (85.2) 25 (14.8) 0.73 28 (35.4) 46 (58.2) 5 (6.3) 52 (30.8) 102 (60.4) 15 (8.9) 0.66 68 (86.1) 49 (62.0) 56 (70.9) 69 (87.3) 144 (85.2) 70 (41.4) 116 (68.6) 148 (87.6) 0.86 ⬍0.01 0.72 0.96 79 21.9 ⫾ 6.6 9.0–35.0 169 21.1 ⫾ 6.6 5.0–35.0 0.40 79 201 ⫾ 41 90–332 145 207 ⫾ 43 88–336 0.30 79 159 ⫾ 27 121–237 147 161 ⫾ 27 120–240 0.49 79 72 ⫾ 13 49–108 169 74 ⫾ 12 43–106 0.15 79 117 ⫾ 18 83–170 168 119 ⫾ 22 79–197 0.40 79 66 ⫾ 10 31–88 168 68 ⫾ 12 36–100 0.13 44 (55.7) 8 (10.1) 19 (24.1) 8 (10.1) 104 (61.5) 8 (4.7) 39 (23.1) 18 (10.7) 0.43 13 (16.5) 4 (5.1) 30 (17.8) 6 (3.6) 0.80 0.57 47 (59.5) 8 (10.1) 24 (30.4) 86 (50.9) 27 (16.0) 56 (33.1) 0.34 57 (72.2) 22 (27.8) 110 (65.1) 59 (34.9) 0.27 0.41 2211 Table 1 Continued Characteristic Left anterior oblique view lead position, n (%) Anterior Lateral Posterior Anterior-posterior view lead position, n (%) Apical Basal Mid Paired Echo No Paired Echo p (n ⴝ 79) (n ⴝ 69) Value 16 (21.1) 54 (71.1) 6 (7.9) 50 (35.0) 73 (51.0) 20 (14.0) 0.02 9 (11.8) 7 (9.2) 60 (78.9) 18 (12.6) 14 (9.8) 111 (77.6) 0.97 ACE ⫽ angiotensin-converting enzyme; ARB ⫽ angiotensin receptor blocker; LBBB ⫽ left bundle-branch block; LVEF ⫽ left ventricular ejection fraction; NYHA ⫽ New York Heart Association; RBBB ⫽ right bundle-branch block; VT ⫽ ventricular tachycardia. tients with a SPWMD ⱖ130 ms did not have significantly improved six-month changes in LVESVI, LVEDVI, or ejection fraction compared with those with SPWMD ⬍130 ms; again, this finding was independent of heart failure etiology. In addition, the test characteristics for a SPWMD ⱖ130 ms to predict a responder were poor (Table 2). Correlation between baseline SPWMD and measures of clinical improvement. Baseline SPWMD parameters did not significantly correlate with six-month change in oxygen consumption (⫺0.04, p ⫽ 0.75), six-month change in 6-min walk (⫺0.06, p ⫽ 0.59), six-month change in quality of life (0.11, p ⫽ 0.32), or six-month change in NYHA functional class (0.06, p ⫽ 0.54). Patients with a SPWMD ⱖ130 ms were no more likely to have six-month improvement in any of the clinical parameters (Table 3). The test characteristics for a SPWMD ⱖ130 ms to predict an improvement in at least one NYHA functional class were poor (Table 2). In the linear regression analyses, no significant interactions between SPWMD and CRT with respect to improvements in LVESVI, LVEDVI, and LVEF were found. DISCUSSION With respect to reverse remodeling, systolic function, and improvements in clinical outcomes, SPWMD as determined by M-mode echocardiography did not predict a response to CRT in this group of patients. We do not believe that our findings bear any reflection on the validity of the concept that true baseline LV dyssynchrony itself might predict benefit with CRT. Instead, contrary to previous publications, we believe our data demonstrate that M-mode SPWMD does not provide a reliable or accurate reflection of actual LV dyssynchrony. Primarily, the limited feasibility of obtaining the necessary M-mode measurements in order to calculate the SPWMD suggests that this method of screening for CRT selection would likely not be applicable in clinical practice. In this cohort, nearly one-half (45%) of patients had neither a definitive septal nor posterior wall deflection visualized on M-mode echocardiography. Twenty-seven (34%) had only 2212 Marcus et al. SPWMD Fails to Predict CRT Outcomes JACC Vol. 46, No. 12, 2005 December 20, 2005:2208–14 Table 2. Sensitivity, Specificity, and Positive and Negative Predictive Values of SPWMD ⱖ130 ms for Reverse Remodeling and Clinical Improvement Six-Month Change Sensitivity Specificity Positive Predictive Value Negative Predictive Value LVESVI reduction of at least 15% Increase of at least one NYHA functional class 24% 24% 66% 66% 29% 29% 61% 61% LVESVI ⫽ left-ventricular end-systolic volume index; NYHA ⫽ New York Heart Association; SPWMD ⫽ septal-to-posterior wall motion delay. one of the two walls exhibiting a definite systolic excursion. The remaining 13 patients (16%) of the cohort with M-mode echocardiograms showed both definitive septal and posterior wall deflections. However, as demonstrated in Figure 2, the SPWMD measurement remained difficult even when both septal and posterior wall deflections are well visualized. The difficulty was further confounded by the thinning and akinesis of infarcted segments frequently present in many of these predominantly ischemic patients. Given the practical limitations of obtaining these measurements, the poor inter-observer reproducibility in our study was not surprising. How then can the discrepancies between previous studies and our current study be explained? Pitzalis et al. demonstrated that SPWMD predicted echocardiographic parameters of reverse remodeling in 20 patients (20% with ischemic cardiomyopathy) undergoing CRT (9); the same group more recently showed that SPWMD predicted clinical benefit in 60 patients (22% with ischemic cardiomyopathy) undergoing CRT (8). It is not clear if any of the patients from the first study were included in the second, but, at the most, all of the data supporting the use of SPWMD as a useful predictor stems from 80 patients, 17 (21%) of whom had an ischemic cardiomyopathy. Our cohort included 79 patients, 57 (72%) with an ischemic cardiomyopathy. Therefore, it is possible that the different conclusions between the studies are due to the significantly larger number of patients with ischemic cardiomyopathies in our patient group. Indeed, patients with ischemic cardiomyopathies may be more likely to have focal hypokinesis or akinesis that would sufficiently perturb septal or posterior wall motion so as to make accurate measurements of systolic deflections difficult if not impossible. However, separate analyses of the 22 patients with non-ischemic cardiomyopathy in our study (a number comparable to the original study) (8) also failed to demonstrate any predictive value of SPWMD. As described in the Methods section, the M-mode images in the previous studies were taken in the parasternal short-axis view at the level of the papillary muscle (8,9), whereas our M-mode images were taken in the parasternal long-axis view at the tips of the mitral valve leaflets. Although it is theoretically possible that a measurement taken a few millimeters towards the base would make such a significant difference, we doubt that it would rectify the significant difficulties in identifying a definite systolic excursion in one or both walls. If such a difference were found, this would mean that the measurement at the papillary muscle would have to be quite precise in location, potentially limiting applicability in clinical practice. In our opinion, it is more likely that defining the complex activation sequence of the LV using a single dimensional view is inherently unreliable independent of the precise location of the ultrasound beam. Moreover, because septal infarcts tend Table 3. Difference in Six-Month Change in Clinical Response Measures by SPWMD at Baseline Measure Six-month change n Mean ⫾ SD Range Six-month change n Mean ⫾ SD Range Six-month change n Mean ⫾ SD Range Six-month change Improved No change Worsened SPWMD <130 ms SPWMD >130 ms p Value 42 0.4 ⫾ 3.1 ⫺9.5 to 8.0 21 1.2 ⫾ 2.7 ⫺4.2 to 8.7 0.29 55 42 ⫾ 73 ⫺91 to 229 26 41 ⫾ 102 ⫺177 to 249 0.97 62 ⫺7 ⫾ 21 ⫺67 to 33 27 ⫺10 ⫾ 20 ⫺41 to 34 0.62 25 (39%) 31 (48%) 8 (13%) 8 (29%) 16 (57%) 4 (14%) 0.63 in peak VO2 (ml/kg/min) in 6-min walk (ms) in QOL (points) in NYHA functional class NYHA ⫽ New York Heart Association; QOL ⫽ quality of life; SPWMD ⫽ septal-to-posterior wall motion delay; VO2 ⫽ oxygen consumption. JACC Vol. 46, No. 12, 2005 December 20, 2005:2208–14 Marcus et al. SPWMD Fails to Predict CRT Outcomes 2213 Figure 2. This figure illustrates the ambiguous nature of the septal-to-posterior wall motion delay (SPWMD) measurement even when both walls were well visualized. It is uncertain whether the septal wall deflection should be measured at A, the first deflection, at B, the middle of the larger area of deflection, or at point C where the maximum deflection is seen. The initial septal wall deflection is too close to the QRS to represent contraction and may reflect posterior motion resulting from ventricular interaction. The middle of the larger area of septal wall deflection is appropriately timed while the maximum septal wall deflection occurs in diastole. to spare the proximal septum, basal beam angulation may theoretically produce better results in ischemic patients. Nevertheless, in their most recent publication, Pitzalis et al. considered the SPWMD to have a value of 0 ms when septal akinesis was observed, potentially biasing the results of the study (8). Our data, collected in a variety of echocardiography laboratories across the U.S. and involving a majority of ischemic cardiomyopathy patients, are more representative of clinical practice than those acquired in a single center with a majority of non-ischemic cardiomyopathy patients. Tissue Doppler imaging (11,15–17), strain rate imaging (11,17), and methods based on phase analysis (18) all show great promise in the measurement of intraventricular dyssynchrony. One promising method for detecting and measuring dyssynchrony uses an index based on the standard deviation of the time to peak systolic shortening in 12 myocardial segments: Yu et al. (17) have shown that a standard deviation of 33 ms or greater predicts response to CRT with a high degree of sensitivity and specificity . A limitation of this method is that nearly all of the published series have been performed with echocardiographic systems available from a single vendor and the generalizability of these measurements to other systems has not been proven. In contrast, most of the current echocardiographic systems are capable of recording pulsed tissue Doppler velocities, a potentially useful measurement that can be used to obtain timing differences between peak systolic velocities among different segments. Using this technique, one study demonstrated that a septal to lateral wall delay of greater than 60 ms predicted a favorable response to CRT (15). A recog- nized limitation of the pulsed Doppler technique is that only one segment can be recorded in a given cardiac cycle and may be influenced by timing shifts from beat to beat (16). These methods remain investigational, are timeintensive, and are not currently available in the great majority of clinical non-invasive laboratories. On the other hand, although M-mode echocardiography is clinically widely available and technically easy to perform, our findings suggest that it should not be used for patient selection for CRT. Our study demonstrates that this parameter based on M-mode echocardiography, while attractive in its apparent simplicity, is not adequately robust to be applied in clinical practice. A major concern is that patients, especially those with ischemic cardiomyopathy, will not be offered this therapy on the basis of the previously reported studies. Study limitations. The major limitation of this study is that the M-mode images were not targeted to prospectively collect these data. However, all M-mode imaging was performed in accordance with the American Society of Echocardiography recommendations. All centers followed a standardized protocol, and all echocardiograms were analyzed in an experienced core laboratory. CONCLUSIONS Septal-to-posterior wall motion delay based on conventional M-mode echocardiography is not adequate to predict clinical or remodeling response to CRT and therefore should not be used to guide CRT patient selection. Because emerging imaging techniques that provide two- and three- 2214 Marcus et al. SPWMD Fails to Predict CRT Outcomes dimensional measures may more accurately reflect mechanical dyssynchrony, they will likely prove superior in selecting appropriate patients for CRT and will therefore have an expanding role in clinical practice. Reprint requests and correspondence: Dr. Elyse Foster, UCSF Cardiology, M-314, 505 Parnassus Avenue, San Francisco, California 94143-0214. E-mail: [email protected]. JACC Vol. 46, No. 12, 2005 December 20, 2005:2208–14 8. 9. 10. REFERENCES 1. Eriksson P, Hanson PO, Eriksson H, et al. Bundle-branch block in a general male population: the study of men born 1913. Circulation 1998;98:2494 –500. 2. Grines CL, Bashore TM, Boudoulas H, et al. Functional abnormalities in isolated LBBB: the effect of interventricular asynchrony. Circulation 1989;79:845–53. 3. Little WC, Reeves RC, Arciniegas J, et al. Mechanism of abnormal interventricular septal motion during delayed left ventricular activation. Circulation 1982;65:1486 –91. 4. Baldasseroni S, Opasich C, Gorini M, et al., Italian Network on Congestive Heart Failure Investigators. Left bundle-branch block is associated with increased 1-year sudden and total mortality rate in 5,517 outpatients with congestive heart failure: a report from the Italian network on congestive heart failure. Am Heart J 2002;143: 398 – 405. 5. Higgins SL, Hummel JD, Niazi IK, et al. Cardiac resynchronization therapy for the treatment of heart failure in patients with intraventricular conduction delay and malignant ventricular tachyarrhythmias. J Am Coll Cardiol 2003;42:1454 –9. 6. St. John Sutton MG, Plappert T, Abraham WT, et al. Multicenter InSync Randomized Clinical Evaluation (MIRACLE) Study Group. Effect of cardiac resynchronization therapy on left ventricular size and function in chronic heart failure. Circulation 2003;107:1985–90. 7. Auricchio A, Stellbrink C, Butter C, et al. Pacing Therapies in Congestive Heart Failure II Study Group; Guidant Heart Failure Research Group. Clinical efficacy of cardiac resynchronization therapy 11. 12. 13. 14. 15. 16. 17. 18. using left ventricular pacing in heart failure patients stratified by severity of ventricular conduction delay. J Am Coll Cardiol 2003;42:2109 –16. Pitzalis MV, Iacoviello M, Romito R, et al. Ventricular asynchrony predicts a better outcome in patients with chronic heart failure receiving cardiac resynchronization therapy. J Am Coll Cardiol 2005; 45:65–9. Pitzalis MV, Iacoviello M, Romito R, et al. Cardiac resynchronization therapy tailored by echocardiographic evaluation of ventricular asynchrony. J Am Coll Cardiol 2002;40:1615–22. Schiller NB, Shah PM, Crawford M, et al. Recommendations for quantitation of the left ventricle by 2-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr 1989;2:358 – 67. Yu CM, Fung WH, Lin H, et al. Predictors of left ventricular reverse remodeling after cardiac resynchronization therapy for heart failure secondary to idiopathic dilated or ischemic cardiomyopathy. Am J Cardiol 2002;91:684 – 8. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1:307–10. Bland JM, Altman DG. Measurement error. BMJ 1996;313:744. Bland JM, Altman DG. Measurement error and correlation coefficients. BMJ 1996;313:41–2. Bax JJ, Marwick TH, Molhoek SG, et al. Left ventricular dyssynchrony predicts benefit of cardiac resynchronization therapy in patients with end-stage heart failure before pacemaker implantation. Am J Cardiol 2003;92:1238 – 40. Bax JJ, Ansalone G, Breithardt OA, et al. Echocardiographic evaluation of cardiac resynchronization therapy: ready for routine clinical use? A critical appraisal. J Am Coll Cardiol 2004;44:1–9. Yu CM, Wing-Hong Fung J, Zhang Q, et al. Tissue Doppler imaging is superior to strain rate imaging and postsystolic shortening on the prediction of reverse remodeling in both ischemic and nonischemic heart failure after cardiac resynchronization therapy. Circulation 2004; 110:66 –73. Kerwin WF, Botvinick EH, O’Connell JW, et al. Ventricular contraction abnormalities in dilated cardiomyopathy: effect of biventricular pacing to correct interventricular dyssynchrony. J Am Coll Cardiol 2000;35:1221–7.