Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
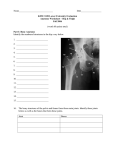
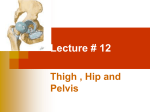
Unit III - Understanding Athletics - Related Injuries to the Lower Quarter Chapter 10 Hip, Pelvis & Thigh Injuries Objectives Describe the basic anatomy of the hip Explain common hip, pelvis & thigh injuries that occur with athletic participation Identify common signs & symptoms of hip, pelvis & thigh injuries Explain the treatments performed by an ATC for specific hip, pelvis & thigh injuries Hip Joint Facts Contains some of the strongest muscles in the body Subject to tremendous demands Vulnerable to injuries that can sideline a player for long periods of time Important to know how to prevent & treat injuries to these areas Anatomy Classified as a synovial ball-and-socket type of joint Articulation – Between the femur & pelvis Connected with thick strong ligaments – Femur Longest bone in the body Two muscle groups of the femur – quadriceps & hamstrings – Pelvis Acetabulum-hip socket – Head of femur fits into “cup shaped” acetabulum – Very deep – Covered by thick ligamentous structure provide stability Anatomy-Hip Joint Anatomy-Hip Muscles Include most powerful muscles in the body Hip flexion – Hip flexors Hip extension – Hamstrings & gluteus maximus Abduction – Lateral muscles gluteus medius, gluteus minimus & tensor fascia latae Adduction – Groin muscles Run down the medial aspect of the femur Anatomy-Hip Muscles/Anterior Anatomy-Hip Muscles/Posterior Anatomy-Hip Muscles/Lateral Preventing Hip Injuries Hip is a very stable joint – Trainer sees few sprained ligaments or dislocations in this area – Trainer will see many muscular strain-related injuries Proper flexibility training & stretching prior to activity is warranted Proper strength training to muscles around hip & lower torso – i.e. “core” region – Proper strength necessary for normal balance & stability Sports expose thigh to contact – Athletes must wear proper equipment (pads) – Contact-type injuries can occur at the iliac crest (point of the hip) This area has little natural protection – Football players required to wear a hip pad here Treating Hip, Pelvis & Thigh Injuries & Conditions Most injuries to hip, pelvis & thigh are – Strains – Contusions Area is not exempt from other injuries – Fractures – Dislocations Muscle & Tendon Injuries Thigh strains are common athletic injuries – Hip flexor – Hip extensor – Groin muscles Many muscles in the leg cross two joints – Some see this as the cause of strains in the region Strength imbalance occurs – Stronger muscle group puts excessive tension on the opposing muscle group i.e. athlete has a great deal of strength in quads but hamstrings are weak making hams prone to strain Muscle & Tendon Injuries Care PRICE Wrap with a supportive elastic bandage Moderate & severe strains – Need to be referred to a physician Rehabilitation – Focus on regaining Strength ROM Enhancing flexibility – Prior to returning to play Assorted Hip Area Stretches Assorted Hip Area Stretches Bone Injuries Athletic-related fractures of the hip, pelvis & femur – Often occur as a result of an avulsion Tendon pulling away the bone – Disruption of the epiphysis Damage to the growth plate – Stress – Trauma to the femur Pelvic fractures are not common – Do occur – Excessive stress is placed on the bone tissue Avulsions Avulsion fracture – Result of forceful muscle contractions – Literally pull the bone away at the site where tendon attaches – Example Football player continues to run aggressively forward While a defender is holding his leg Hip flexor forcefully contracts Causes a fracture Growth Plate Fractures Epiphyseal fractures – Occur at the growth plates of bones – Especially at the capital femoral epiphysis Where the neck & head of the femur join Most common hip disorder in active children between the ages pf 10-15 Head of femur splits off the neck – Causes pain in groin, hip & knee If trainer suspects this – Athlete referred to a physician – Treatment includes Stopping the slippage Helping to close the growth plate with a surgical procedure Growth Plate Fractures Stress Fractures Femoral stress fractures do occur – Although uncommon – Do occur in running-oriented athletes Causes – Repetitive stress Result of the force of pounding the lower extremity while running – Causes femur to bend slightly repeatedly Stretching one side, compressing the other Small hairline fractures develop from bone tissue being repeatedly stretched Causes a great deal of pain & discomfort Indications – Reduce stress to the fracture site so it can heal Rest Alternative activity (i.e. aquatic therapy) Stress Fractures Bone scan showing positive right femoral neck stress fracture Stress Fractures MRI showing inferior femoral neck stress fracture Femur Fractures Largest bone in the body Extreme stress required to fracture it Signs & Symptoms – Severe pain – Loss of function – Internal bleeding – Swelling – Tearing of muscles, tendons, nerves & arteries – Athlete unable to move the leg – Often causes leg to externally rotate Femur Fractures View from front View from side Femur Fractures Initial treatment – Immobilization – Transportation to the hospital by EMS They will often use a traction splint Gently pulls the femur – Helps reduce leg pain & spasm Hip Dislocations Extreme stress can cause a dislocation Most occur posterior Usually accompany other trauma – Such as a fracture Severe damage can occur in this area – Due to nerve & vascular structures Signs & Symptoms – Athlete in extreme pain – Leg is often internally rotated Hip Dislocation Head of femur should be here Hip Dislocations Initial treatment – Ambulance called immediately – Transported to the hospital ASAP Only a physician should reduce a hip dislocation Significant follow-up treatment required – Before the athlete can return to activity Rehabilitation – Begins with establishing normal ROM & strength – Gait training will be necessary Learning how to walk normally This is a long process Other Common Injuries Thigh contusion – Common injury in contact sports Legg-Calve’-Perthes Disease – Another injury trainers must always keep in mind – Especially with younger athletes Hip & Thigh Muscle Contusions Deep thigh contusion are common – Predominately to the quads – Especially in collision sports – Can cause disability Severe contusions can cause – Tissue tearing – Extensive bleeding If not managed appropriately serious thigh contusions – Cause a condition known as myositis ossificans Formation of bone tissue within the muscle Disability & loss of function is a typical consequence Hip & Thigh Muscle Contusions Deep contusion in the hamstrings Myositis Ossificans Radiograph of tibia and fibula showing periosteal new bone formation from a subperiosteal hematoma and, separately from it, an area of ossification within the muscle due to myositis ossificans. It would look very similar in the quadriceps of the thigh. Hip & Thigh Muscle Contusions When treating a thigh contusion (quads) – Proceed with the PRICE technique With knee in a flexed position during ice application – Trainer may put athlete in a hinged knee immobilizer With it locked into flexion Limits the total loss of flexibility due to the injury Moderate to severe contusion – Place athlete on crutches – Minimize stress to the area – Refer to team physician Hip & Thigh Muscle Contusions Early rehabilitation – Must restore mobility Effective methods – Active rest – Use of ice – Gentle stretching routines – Ultrasound Used to – Resolve the blood that collects internally – Break up the bony tissue deposits Upon return to activity – Trainer places a protective pad over the contusion Repeated contusions to the area can create myositis ossificans Legg-Calve’-Perthes Disease Disruption of blood flow to the head of the femur Causes the tissue at the head of the femur to die Often seen in children & teens who are still growing Signs & Symptoms – Groin or knee pain – Walking with a limp If trainer suspects this – Refer athlete to physician immediately Legg-Calve’-Perthes Disease Radiograph MRI The head of these femurs shows a flat white area on radiograph and a dark area on the MRI. This represents dead bone or bone that no longer has any blood supply.