Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
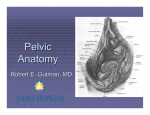
1|P ag e Quick review from the previous lecture…. we said that the true pelvis doesn’t have a roof, rather its continuous with the false (greater) pelvis through which we call it the pelvic inlet or brim. The anterior wall of the pelvic wall we said that it’s made of pubic symphysis and 2 (V) shaped pubic bones. Posteriorly, it’s made of sacrum, coccyx and the piriformis muscle(passing through the greater notch. The lateral wall is formed mainly by the obturator internus muscle with it’s covering fascia. Now let’s start with the inferior pelvic wall ( the floor )…. The floor is formed by which we call it the diaphragm → but its opposite to the thoracic diaphragm, how ? this one is concave superiorly, so like a bowl. now most of the walls are formed by bones and muscles, except the floor, it’s mainly muscular. this diaphragm divides the true pelvic cavity into main pelvic cavity and perineum (later). 2|P ag e Inferior view Now the main muscle components of the diaphragm… 1- The coccygeus muscle: It’s called also the ischiococcygeus, why? because it’s arising from the ischial spine to the coccyx & Lat. Lower sacrum. It’s a small triangular muscle It lies on the inner surface of the sacrospinus ligament, which separate the greater sciatic foramen above from the lesser below. Innervation: branches of S4 & S5. Actions: support pelvic viscera and slightly flexes coccyx. 2- Levator ani muscle: The main muscle, wide muscular sheet. It’s divided into 3 parts. Origin : Pubic bone (ant.)→Tendinous arch of obturator fascia(dividing the obturator muscle into superior and inf. parts →Ischial spine(post.). * the thickened part of the obturator fascia to give an origin to the levator ani we call it tendinous arch of obturator fascia.(green line). Insertion: The muscle will spread medially, until it Reaches the midline, there it will fuse With the muscle of the opposite side. 3|P ag e →if you look to the inferior view: a gap is present anteriorly between the 2 levator ani , and this gap will provide a passage (hiatus) of the urethra and vagina → called urogenital hiatus. →Now in the middle part and posterior part when the muscles fuse they will form a very strong fibrous ligament but is interrupted by the anal orifice. →So the fibrous ligament will be divided into anterior part which we call it the perineal body and the tendinous attachment behind the anus which is continuous with the coccyx we will call it the anococcygeal body or ligament. →Notice that we have a thickening in the origin and one(divided into 2) in the insertion. Now divisions of the levator ani muscle: Anterior division: Short muscular slips From pubic bone blend with fascia around strc. In the midline. Surrounds the vagina in the female and prostate in males. Subdivided into: A- Pubovaginalis (sphincter vaginae, beacause it acts as a sphincter) or puboprostaticus (levator prostatae, beacause it elevates the prostate in addition to anus). Notice the names indicate origin and insertion. 4|P ag e B- puboperinealis muscle: some fibers goes to the perineal body C- Puboanalis: to the anus. Few fibers. the previous two are not important - Intermediate division: from the pubic bone. Divided into 2 parts a) puborectalis: thick narrow part forms a sling around the ano-rectal junction → it will pull this junction forward → angulation btw the rectum and anal canal → we refer to it as the anorectal angle 80o. IMP. WHY ? → Maintains fecal continence, destruction to this muscle causes fecal incontinence. the sling is thick in vertical dimension but in a transverse dimension it’s narrow. b) Pubococcygeus: →thinner & wider from the pubic bone & ant.part of tendinous arch to → the anococcygeal body. -posterior division: (the iliococcygeus). From post. tendinous arch & ischial spine →to anococcygeal & coccyx. More aponeurotic than muscular → rare muscle fibers.(dense regular C.T .→ support and resist downward pressure during inspiration 5|P ag e In general the levator ani has 3 main functions : 1- Support and resist downward pressure caused by inspiration when the thoracic diaphragm contracts. In females, helps in child bearing. 2- Formation of anorectal angle by the puborectalis part. 3- Sphincteric functions around anus, vagina, urethra. Innervations of levator ani muscle: Mainly by pudendal nerve ( by inferior anal(rectal) nerve). Fibers from S4 called nerve to levator ani. As we said the levator ani will divide the true pelvic cavity into 2 parts: Upper main pelvic cavity Lower cavity ( the perineum) → the main nerve is the pudendal nerve (the nerve of shame) 6|P ag e Summary 7|P ag e Pelvic fascia It covers the pelvic cavity and wall. Composed of two parts : Parietal & visceral. - The parietal fascia : will cover the muscles forming also the deep fascia of the muscles themselves and it will take the name of the muscle it covers. The green layer in the figure. How many muscles we have ? posteriorly piriformis → so we should have a piriformis fascia lat. → obt. Internus → so we should have obturator fascia → in the middle of this muscle it will thicken forming the tendinous arch. Notice the perineum under the levator ani , notice the sup. & inf. Fascia of the levator ani → they are continuous with each other where ? through the anterior gap ( the urogenital hiatus) . 8|P ag e - the visceral layer: Covers and supports visceral organs like prostate, uterus &bladder. It will become the adventitia of these organs In certain locations it will thicken and extend from the visceral layers to the parietal fascia → now it will become a ligament why we need these ligaments ? to suspend the organs in their places. we have 4 important ligaments : 1- pubovesical (in females) &puboprostatic ligament ( in males) extends from pubic fascia down towards the neck of bladder or prostate. 2- different ligaments in females : important in supporting the uterus and vagina in their middle position in the pelvic cavity btw the bladder ant. And the rectum post. . a) pubocervical ligament : from the pubic bone → obturator fascia → cervix & it’s lateral to the pubovesical . 9|P ag e b) Another one which arises from the posterior pelvic cavity, the sacrocervical ligament, c) The third one comes from the lateral abdominal wall which is, The transverse cervical (cardinal L.) (principal L.). if you cut the cardinal ligament you will see an artery and vein inside It, which is the uterine artery. Clinical note: this is important because when you need to ligate this artery and vein during hysterectomy . however we know that the ureter passes under this artery and ligament so you have to avoid it. And this is known as “the water and the bridge”. ( water: ureter, bridge: cardinal L) Quick review: Pelvic space: Greater ( false) pelvis is not part of the pelvic cavity rather it’s a part of the abdominal cavity. True pelvis: divided by the pelvic diaphragm into upper main pelvic cavity and lower the perineum. The pelvic brim seperates between the true and the false pelves. And the borders of the brim are : Posteriorly: the promontory of the sacrum with it’s wings . Anteriorly: upper edge of the pubic symphesis Laterally: the iliopectineal line ( part is iliac and is called the arcuate line and the pubic part is called the pectineal line). 10 | P a g e cont…. The pelvic wall: The pelvic girdle : the bony pelvis only → 2 hip bones, sacrum & coccyx. They are joined by 4 joints they are: Anteriorly: pubic symphesis → secondary cartilaginous Posteriorly: the 2 sacroiliac joints → compound joint (anteriorly synovial And posteriorly fibrous Syndesmoses with little movement). * Most of the joints in the pelvis they must have a little movement. Posteroinferior: btw the sacrum and the coccyx → sec. cartilaginous, but why its fixed in its place although there should be a movement? Because a dense “sleeve” of ligaments””زي كم القميص around this joint. But it may be disrupted. The muscles: 4 muscles: 1- The piriformis: located post. , innervated by nerve to piriformis ( it comes from the L5,S1 and S2 , it was a H.W), function : lat. rotation 2- Obturator internus: on the lat. Wall 3- Coccygeus 4- Levator ani form the diaphragm inferiorly. The fascia: Parietal fascia: covering the 4 muscles. Visceral fascia: 4 ligaments Male&female : pubovesical or puboprostatic Female: additional 3 ligaments. Mentioned previously. It’s 3am → you have to appreciate this , yla appreciate Now we move to gender variations 11 | P a g e Gender variations Why is this? because of the physiological functions of child bearing and pregnancy. Male Female Thickness of hip bone False pelvis True pelvis Pelvic Inlet (P. brim) Pelvic outlet Pubic angle Much thicker More prominent landmarks why Deep Narrow, deeper, & tapered(laterally And anterioposteriorly) funnel shaped in male Wider and shallower Wider, shorter & cylindrical shape in Female >facilitate birth Heart-shaped (android pelvis) Oval to round shape in female (Gynecoid pelvis) More oval ( ant./post.) Sharp <70 o (indicated by index & middle fingers). round Wide >80 o (indicated by index and thumb). Notes: why male bone is thicker ? because of strong musculature pulling the insertions→ so the bone is getting thicker.other examples : bicipital groove is getting deeper as the biceps continue pulling…. Pubic tubercle and so on...and males especially have stronger muscles by the action of androgens also . Why we have shallower false pelvis in females? Because it’s oriented more horizontal of iliac bone Why its more tapered in males ? the sacrum more anteriorly and the ischial tuberosities become more inverted. In females the tuberosities are more everted and the sacrum is flatter. What makes the male outlet more oval? The ischial tuberosities, because they are more inverted toward inside. The pubic arch is formed by the 2 inferior pubic rami. Forming the subpubic angle. Why pubic angle in females are wider ? because the ischial tuberosities are everted outside > so the rami will move with it . So the ischial tuberosity determines the outlet and pubic angle as we see. 12 | P a g e look at this x-ray and the features we talked ablout: the inlet , the angle .. to determine the horizontal orientation of the iliac wings → you draw a vertical line from the ASIS downward you will see it passes medial to the greater trochanter of the femur in males while in females it passes lateral to the greater trochanter of femur which indicates that the iliac crest is more horizontal and wider. Other variations: The sacrum: in females its more flat While in males its curved more ant. Forming the tapering of the pelvis. The obturator foramen: in males it’s round in females → more oval or triangular because the ischium is moving more lateral and wider . 13 | P a g e pelvic fractures They don’t include the fractures of acetabulum → classified fractures of the lower limbs. Pelvic fractures include the ring shaped bones of the pelvis. In the ring shaped bones like mandible or pelvis, when you have a fracture in one side you always look for a fracture on the other side how ? if the fracture is anterior you look posterior. Classifications of fractures : 2 types: 1. Stable fractures: most of the time doesn’t need surgical intervention and they are one point fractures, just need medical stabilizing 2. Unstable: you need surgical intervention , and they are two points fractures or more→ emergency sometimes tile classification Based on the stability of the sacroiliac joint: classified to A,B &C Type A: if you have a fracture and the SI joint is intact . (stable) Type B: if you have a partial distortion in the SI of the ant. Part of the joint (the synovial part) type C: complete distortion and separation of SI joint. (unstable) 14 | P a g e Stable pelvic fracture: 1. Fractures of the coccyx: the ligaments are weakened → distortion of the joint, very rare. Patient will come with coccydynia(localized pain & infl. Sometimes) Typical history: falling down on buttocks. 2. transverse sacral fractures: very rare to happen due to its thick bone, however when happen it doesn’t need treatment because the ligaments are there supporting the bone→ no displacement just you tell the patient to sit on a smooth surface. 3. Duverney fracture: (iliac wings) A direct blow on the lateral side of the hip (crest) This was described by james duverney in 1751 Why it’s stable ? no displacement, why ? due to presence of muscles which are the iliacus and the gluteal muscles. Most of the time is stable unless you have a complication → injury to a blood vessel → so you have to surgically interfere to stop the bleeding. 4. Ipsilateral fracture: of pubic & ischial rami. On the same side of the ring. Stable → no surgical intervention, only symptomatic Rx. Unless there is additional complication ( like soft tissue injury or hemorrhage) look slide 30 for more pics. 15 | P a g e The unstable fractures: includes ( B&c ) 1- Open book fracture: in three points Partially unstable Includes the anterior compartment of the SI joints and the pubic symphysis We will have disrupted pubic symphysis (pubic symphysis diastasis) When you have pubic diastasis the 2 pubic bones will separate → they will tear the anterior sacroiliac ligament. So the synovial part will be separated so type B → partially unstable. Rx: surgical intervention to close the book and is stabilized with plate and screws. 2- Straddle fracture: (same as ipsilateral but both sides) ( خيَّة ِ إِصا َبة َفرْ َش, )الفسخ Double break of ant. Pelvic ring in both sides Usually in car accidents. This fracture is comminuted (small pieces) And since there is the bladder behind → usualy associated with injury to the urogenital viscera → so you have to deal with the soft tissue first then reduction of bones. 16 | P a g e 3- Vertical shear fracture: type C (completely unstable) 2 point fracture : anteriorly the pubic rami and posteriorly all the SI joint ( the synovial and the fibrous part) → so we call it hemipelvic fracture The fractured segment will be pulled upward. The complication : Minor : Upward dislocation of sacroiliac joint & ipsilateral fracture of pubic rami Major : a) Fracture of the transverse process of L5. b) Avulsion of ischial spine (destruction) c) Stretching of sacral nerves d) Hemorrhage : the most serious one! Because it may happen from an artery (from the sup. Gluteal artery ). Hemorrhage in pelvic fractures: 100% there is a bleeding in these fractures. The mortality rate in PF 5-15% (high) ½ due to hemorrhagic shock Source of bleeding: - Fractured bone - Pelvic veins 90% - Pelvic arteries: 10% Most serious & leading cause of death in PF (especially in vertical shear Fracture in which the sup. Gluteal artery( largest branch of internal iliac) is the most common involved. **emergency care otherwise death within 24 hrs 17 | P a g e The end !Slide 53 next lecture "لن تكون متدينا إال بالعلم ...فاهلل ال يعبد بالجهل" –مصطفى محمود 18 | P a g e