Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Turner syndrome wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Artificial heart valve wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
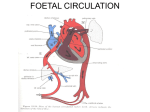
Catheter Based Treatment of Adult Congenital Heart Disease Zoltan G. Turi, M.D. Robert Wood Johnson Medical School August 21, 2004 [email protected] TERMS OF USE This site has been developed solely for use by members and authorized guests of the Society for Cardiovascular Angiography and Interventions (SCAI), henceforth referred to as "the users." The users are authorized to view, copy, download and print materials from this website subject to the following terms, conditions and exceptions: 1. The materials are to be used solely for noncommercial educational purposes directed toward students ("fellows") in interventional cardiology training programs accredited by the Accreditation Council for Graduate Medical Education (ACGME) or physicians preparing to take the examination for the ABIM Certification in Interventional Cardiology. Any other use is expressly prohibited. 2. The materials are not to be reproduced or included in any way in any textbooks, journals, other enduring materials, presentations (other than described in item #1 above) without the prior written permission of the authors. 3. The materials are not to be modified. They are to be used for instructional or self-study purposes in the format provided with the source clearly identified. 4. The materials are to be used free of charge. Neither the users nor SCAI shall charge a fee for use of these materials. 5. The materials remain the sole intellectual property of the individual contributors, who retain copyright to those materials and have granted SCAI a license to post them on this website for the purposes described in item #1. 6. Copyright information or other proprietary notices on the materials or elsewhere on this website may not be removed, changed, or altered in any way. 7. The site design, layout and individual elements are not to be reproduced, copied or redistributed except as indicated above in item #1 above. The information on this site should not be used as a substitute for medical evaluation, advice, and/or treatment by a qualified healthcare provider. The materials are not intended for public or patient education, but rather for education of fellows in training programs as described in item #1 above. Information in text files, slides, graphs or articles on this website do not replace consultations with qualified healthcare professionals to meet medical needs. If you are not a health care provider, you should not use this site. We encourage you instead to consult a healthcare professional. The authors, contributors and editorial staff have made every effort to contact holders of copyright to obtain permission to reproduce copyright material. However, if any permissions have been inadvertently overlooked, SCAI will be pleased to make the necessary and reasonable arrangements. If you wish to use the presentation for any purpose other than that outline above, please contact SCAI at [email protected]. Scope of the Problem ● ● ● > 500,000 patients with adult congenital heart disease in the US 0.8 % of live births, not including bicuspid aortic valves (1-2%), MVP (3-7%) Burgeoning technologies – Limit discussion to approved devices, techniques – Limit discussion to relatively common structural abnormalities – not complex post repair states Diseases in Adult Congenital Heart Disease Intervention ● ● All are lesions that typically allow survival to adulthood without intervention Stenoses – Pulmonic ● ● – – ● Valvar Branch Congenital aortic – juvenile bicuspid A.S. Coarctation Fenestrations Patent Foramen Ovale * – Atrial Septal Defect – Patent Ductus Arteriosus* – Ventricular Septal Defects * Account for 93% of systemic circulation in utero – Cardiac Cath in Congenital Heart Disease ● Paradox - Need to know anatomy to do cath ● Cardiac output and shunt calculations essential ● Need to appreciate pitfalls of oxygen consumption measurement ● PVR and SVR importance ● Need to understand basics of shunting ● Need to appreciate basics of mixed venous oxygen saturation Oxygen mixing ● ● ● Right atrial oxygen saturation is highest in: 1. Coronary sinus 2. Inferior vena cava 3. Superior vena cava 4. Left superior vena cava Normal maximum “step-ups” between sites – SVC-PA 7% – SVC-RA 11% – RV-PA 5% Mixed venous = (3*SVC+IVC)/4 Fick principle • As applied to any vascular bed, the difference in oxygen content across that bed divided into the oxygen consumed. • In the setting of a shunt, compare flows across individual beds Fast train = little change in concentration Slow train = maximal extraction and greatest delta But it all depends on oxygen consumption !!! J. Grossman Quick and dirty: Large difference in PA and Systemic saturations: Low cardiac output – train moves slowly – greater extraction Low oxygen carrying capacity – need to extract maximum oxygen because of low hemoglobin Oxygen consumption and Cardiac Output ● O2 onsumption rarely measured directly – – ● Typically assumed to be 125 ml/min/m2 Accurate ± 10 - 30% – Decreased in low output state, somnolence, hypothyroidism, etc. – Increased in high output state, undersedation, hyperthyroidism, etc. Cardiac output (as typically measured) = O2 consumption/ (FA - PA) O2 content * 10 - assumes that pulmonary and systemic flows are equal, PV=FA, and mixed venous (MV) = PA sat Shunts ● Shunt ratio – AO - MV = Pulmonary blood flow PV - PA Systemic blood flow Typically assumed FA = Ao saturation and no right to left; if right to left with ASD or VSD, Ao lower than PV. In ductus with right to left, FA will be lower than Ao. – Ao = 95%; PA = 80%; SVC = 62%; IVC = 70% MV = (3*62 + 70)/4 = 64 Shunt = (95-64)/(95-80) = 31/15 ~ 2:1 Resistance ● Ohm’s Law Voltage drop = flow * resistance Resistance = ● Voltage Flow As applied in vascular physiology: Resistance = Pressure drop across a vascular bed Flow across vascular bed ● As applied to pulmonary hemodynamics: ● PVR = Mean PA – Mean PAW pressure Pulmonary blood flow As applied to pulmonary hemodynamics: SVR = Mean PA – Mean PAW pressure Systemic blood flow Resistance = Wood units. Multiply by 80 for dynes-sec-cm-5 Pulmonary Hypertension ● Variable definitions but typically: – ● ● ● ● mPA < 20 = nl, 20 – 30 = mild, >30 = mod, > 45 = severe Nl PVR = 1- 3 Wood or 80 -240 dynes-sec-cm-5 Nl SVR = approximately 10 x nl PVR PVR/SVR > 0.5 to 0..75 suggests high risk or inoperable patient Vasodilator challenge with nitric oxide, adenosine, oxygen, dihydropyridines, prostacycline, etc. to assess reversibility Pulmonic Stenosis ● ● Adults develop RVH and eventual RV failure Typically occurs in combination with other congenital lesions – ● Tetralogy of Fallot Symptoms – – – – – Fatigue Dyspnea Right heart failure Syncope Exertional angina Pulmonic Valvuloplasty ● Indications: – – ● ● ● Patients with exertional angina, dyspnea, syncope, or pre-syncope where the cause is likely to be PS (e.g. young adults) Asymptomatic patients with normal CO, and gradient > 50 mm Hg Class I; 30 – 50 mm Hg Class II Goal is gradient < 30 mm Hg; Excellent 20 to 30 year results 90 % success Typically use 1 -2 balloons; oversize 20 - 40% Kothari S Pulmonic Valvuloplasty • Suicide ventricle – Typically chronic severe PS – Infundibular hypertrophy – Treat with beta blockade • Surgery for dysplastic valves (Noonan’s syndrome) • Resultant mild or moderate PI well tolerated – RV handles volume overload well Pulmonary Branch Stenosis • May be complication of maternal rubella, William’s, Noonan’s, arteritis, external compression • Associated congenital abnormalities • Typically at origins of main PA branches – May occur at site of prior surgery e.g. Blalock-Taussig • Untreated: lung hypoperfusion/ dyspnea, cyanosis, RV hypertension and failure • Balloon alone – poor results – PA segments too elastic → recoil • Stenting generally successful – risks: – Rupture – Issue of patient growth in children – Pulmonary hyperperfusion – edema, hemoptysis Indian Pediatrics Congenital Aortic Stenosis • Unicuspid valve – rare – requires surgery • Bicuspid – 1 – 2 %; variable course; AR; L dominant; familial clusters. – Associated with coarcts, Williams Syndrome, PDA, cystic medial necrosis, Turner’s Syndrome (30% bicuspid) – May have ejection click – Echo : doming Yale Congenital Aortic Stenosis LV dP/dt 300 200 Ao dP/dt 100 0 Congenital Aortic Stenosis-Treatment ● Antibiotic prophylaxis ● PBAV generally successful ● – Young adults (and neonates) – Indication = gradient > 50 mm Hg regardless of symptoms – Balloon is procedure of choice for congenital AS Complications of PBAV – 5% severe AR – most common with unicuspid valve – Death, blood loss, perforation – 1-2% – Success rates, restenosis, complications similar to surgery – Will eventually need AVR, but when root is bigger Coarctation of the Aorta ● Hypertension – – ● Claudication – – – ● ● ● ● Renal hypoperfusion Renal failure ABI’s No PVD Brachial-femoral lag Syncope > 50% have bicuspid aortic valves VSD, PDA, sub-Ao membrane, parachute mitral, supra-mitral ring associated Occasional similar syndrome 2 trauma o Diagnosis ● Hypertension with or without murmur – Murmur may disappear because of collaterals – Murmur may be continuous because of collaterals – Murmur of associated AS with or without ejection click ● Headaches, chest pain, intracranial hemorrhage ● Claudication only occasionally ● Left arm pressure may be lower if subclavian involved ● Suprasternal notch pulsation ● EKG - LVH Radiographic Findings UW Considerations for Intervention in Coarctation ● Hypertension – Significant afterload on LV → wall stress → LVH ● ● – – – ● ● ● Ameliorated by development of collaterals Exacerbates L → R shunt with associated VSD, PDA avoid ACE inhibitors → renal failure Successful ↓ upper body BP may cause hypoperfusion Baroreceptors/renin-angiotensin system may not reset Planned pregnancy Recurrent coarctation post repair – balloon preferable; no concensus on native coarcts Gradient > 20 mm Hg Coarctation Angioplasty ● ● ● Balloon – – 80-90% success (<10 mm Hg gradient) – do not oversize rupture Complications – Rupture – False aneurysm – Aneurysm in 5% – Higher rate of recurrence than surgery – Paraplegia Antibiotic prophylaxis indefinitely Yale Stenting for Coarctation ● ● Controlled tear Perhaps superior results – Dissection and aneurysm formation less likely Yale Atrial Septal Defect 30% of all congenital heart abnormalities in adults Presenting symptoms – atrial arrhythmias, stroke/TIA, fatigue, exercise Frequently asymptomatic first 3 decades – 70% symptomatic by age 50 Ostium Primum Yale Congenital Heart Disease 70% ASD diagnosis ● 2:1 female – – ● ● ● Yale EKG – iRB3 in 90% CX Ray – pulm vasculature, RA,LA Physical – – – ● MVP MS = Lutembacher Pulmonic flow murmur; diastolic rumble Wide split S2 RV lift Echo – – RV size and function Shunting UMN Percutaneous Closure ● ● Indicated for: Secundum ASD (or Fontan) – > 1.5:1 shunt (at a minimum must have left to right shunt) or ● – ● Shunt ↓with ↑PVR RVVO Contraindications – – – > 38-40 mm A-V valve proximity ± Absence of rim (< 5 mm) Children’s Memorial Chicago Post ASD closure • Medication – Antibiotic prophylaxis x 6 months (none required for untreated ASD’s) – Aspirin and ? clopidogrel x 6 months or anticoagulation • Complications – – – – – – Device embolization Atrial arrhythmias Clot formation on device Pericardial effusion, TIA, sudden death Residual flow through shunt Mechanical interference with adjacent structures ASD – Percutaneous Closure versus Surgery ● ● ● ● Surgery highly effective, low morbidity and mortality in young patients Major and minor adverse events rates with surgery in 5 – 20% range Major and minor adverse event rates with percutaneous approach in 2 – 5% range To prevent device erosion, guidelines for sizing to unstretched orifice size – lowest size that eliminates flow; avoid overriding aorta Patent ductus ● ● Exercise intolerance Angina – ● ● ● Coronary steal in diastole Endocarditis 1/3rd die by age of 40 of PHT, CHF if no Rx. Small PDAs with benign course Yale Congenital Heart Disease ● ● Machinery/continuous murmur CX-Ray prominent pulmonary arteries; biventricular enlargement. PDA ● Indication – – Left to right shunt Endocarditis prevention ● Beak shaped – coils – ● – ● 1 loop PA – rest Ao > 6 mm occluder Not severe PHT with cyanosis Success > 90% PFO Anatomy Photo from Textbook & Atlas of the Cardiovascular System, Thomas, et al. Lurking Clot Theory Cul de sac Valsalva induced paradoxical flow results in embolic event. • 36 year old ♀ 3 wks dyspnea/syncope • Left leg pain • DVT • Occluded left popliteal • PA systolic 80 mm Hg • Multiple pe’s Kessel-Schaefer Circulation 2001 Incidence of PFO in Patients with and without ischemic stroke 50 40 Incidence of PFO (%) 40 P < 0.001 30 20 10 10 0 CVA No CVA n = 60 n = 100 Lechat et al. NEJM 1988:318;1148 Patients with CVA 60 50 Incidence of PFO (%) 54 40 40 30 20 21 10 0 Identifiable cause Risk factor only No identifiable cause n = 19 n = 15 n = 26 Lechat et al. NEJM 1988:318;1148 Recurrent Ischemic Events in Patients with Cryptogenic Stroke and PFO 20 19 Number of CVA/TIA 15 10 5 0 0 Antiplatelet/ Anticoagulant Surgical Closure Cujec et al. Canadian J. Cardiology 1999:15;57 N = 581 Mas NEJM 2001 Rx Aspirin 300 mg Indications • PFO with right to left shunting demonstrable – Bubble study with valsalva on TEE – TCD and • Atrial Septal Aneurysm and • Recurrent cerebrovascular events despite anticoagulation and • No other etiology TIA/stroke Possible Indications Unlikely to be Included ● Scuba divers ● Migraine headaches ● Need for transvenous pacemaker ● Platypnea-orthodeoxia ● Pulmonary hypertension with right to left shunt usually not an indication Ventricular Septal Defects • Perimembranous – Most common – Located under tricuspid and aortic valves – Frequently close in childhood – Device closure experimental – asymmetric to prevent impingement on valves • Muscular – Typically at apex or along muscular upper septum – Most lends itself to percutaneous closure – CardioSeal approved • Supracristal – Between aortic and pulmonic valves P.Lynch Yale VSD – size and shunting ● ● Shunt ratio depends on size of defect and resistance in pulmonary bed Small (restrictive) ,< 0.5 cm → < 1.5 : 1 shunt. 30 – 50% close spontaneously in childhood. ● With large VSD, flow determined by ratio of PVR to SVR. ● High risk endocarditis ● Indications: – symptomatic, Qp:Qs > 1.5:1, PA systolic pressure > 50 mm Hg, ↓’ing LV function, non-Eisenmenger’s physiology Question 1 A 50 year old patient with dyspnea is referred to you because of a "heart murmur". Workup reveals gradient across the pulmonic valve and clinical picture as described. Which one would be the best candidate for balloon pulmonary valvuloplasty? a. A 30 mm Hg gradient across the pulmonic valve. The patient has chronic lung disease. b. An 80 mm Hg gradient across the pulmonic valve. The valve appears dysplastic by echo. c. A 70 mm Hg gradient across the pulmonic valve. The patient has significant findings for right heart failure. d. A 60 mm Hg gradient across the pulmonic valve. The patient has severe bronchospasm and infundibular hypertrophy. Question 2 a. b. c. d. e. A 34 year old woman has a single transient ischemic attack. Extensive neurological workup reveals predisposing factors listed below. Which of the following scenarios would represent indication for percutaneous closure of the PFO? PFO, no atrial septal aneurysm, Protein C deficiency. PFO, atrial septal aneurysm, normal coagulation workup. PFO, no atrial septal aneurysm, normal coagulation workup. PFO, atrial septal aneurysm, migraine headaches. None of the above. for the non-surgical closure of a patent foramen ovale (PFO) in patients with recurrent cryptogenic stroke(1) due to presumed paradoxical embolism through a patent foramen ovale and who have failed conventional drug therapy(2). (1) Cryptogenic stroke - a stroke occurring in the absence of potential phanerogenic cardiac, pulmonary, vascular or neurological sources. (2) Conventional drug therapy - a therapeutic international normalized ratio (INR) on oral anticoagulants Phanerogenic – “denoting a disease the etiology of which is manifest” Question 3 A patient with chronic severe pulmonary hypertension has borderline systemic pressures and persistent systemic desaturation. Noninvasive studies demonstrate right to left shunting across the interatrial septum. You are asked to intervene. You: a. Size the fenestration, determine that there is an ASD and deploy an ASD closure device. b. Defer intervention of any kind. c. In case the fenestration is a PFO, you bring the patient to the cardiac cath lab and examine the effect of oxygen and nitric oxide on hemodynamics. d. Recommend surgical rather than percutaneous closure of an ASD. Question 4 Which one of the following is false? a. Mean survival of untreated coarct patients is age 35 b. A patient with coarctation should typically have a gradient of at least 20 mm Hg before consideration of balloon dilatation c. Antibiotic prophylaxis is not required. d. Acute results of balloon dilatation for native and recurrent coarctation are similar. e. Long term results may include higher rate of aneurysm formation post balloon dilatation of native coarcts compared with surgery. f. Cystic medical necrosis is common and frequently severe in coarctation patients. ● ● ● ● “In adults with (de novo) coarctation, surgical repair can be achieved with zero percent mortality.” – Actually, operative mortality ↑ because of degenerative aortic wall changes, coexist bicuspid aortic valve, CAD, end organ damage from hypertension. – Complications of surgery – paradoxical hypertension, recurrent laryngeal nerve paralysis, phrenic nerve injury, spinal paralysis. “The application of this technique (balloon) for native coarctation is somewhat controversial due to the high incidence (5-10%) of recurrent coarctation and aneurysm formation” Aneurysm in adults after balloon – 49 pts, mean age 22, f/u 10 yrs – 7.5%. Aneurysm is uncommon (3%) with end-to-end repair.