Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
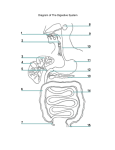
Chapter 23B Digestive System Slides by Barbara Heard and W. Rose. figures from Marieb & Hoehn 9th ed. Portions copyright Pearson Education Digestive System Introduction/Overview Functional Anatomy Mouth, Pharynx, Esophagus Digestive Processes in the Mouth Stomach Small Intestine & Related Organs Large Intestine Physiology of Digestion & Absorption Mouth Oral (buccal) cavity – Bounded by lips, cheeks, palate, and tongue – Lined with stratified squamous epithelium Functions – Ingestion – Mechanical digestion – Chemical digestion – Propulsion © 2013 Pearson Education, Inc. Figure 23.7a Anatomy of the oral cavity (mouth). Soft palate Palatoglossal arch Uvula Hard palate Oral cavity Palatine tonsil Tongue Oropharynx Lingual tonsil Epiglottis Hyoid bone Laryngopharynx Esophagus Trachea © 2013 Pearson Education, Inc. Sagittal section of the oral cavity and pharynx Figure 23.7b Anatomy of the oral cavity (mouth). Upper lip Gingivae (gums) Palatine raphe Hard palate Soft palate Uvula Palatine tonsil Superior labial frenulum Palatoglossal arch Palatopharyngeal arch Posterior wall of oropharynx Tongue Sublingual fold with openings of sublingual ducts Lingual frenulum Opening of Submandibular duct Gingivae (gums) Oral vestibule Lower lip Anterior view © 2013 Pearson Education, Inc. Inferior labial frenulum Tongue Skeletal muscle Functions include – Repositioning and mixing food during chewing – Formation of bolus – Initiation of swallowing, speech, and taste Intrinsic muscles change shape of tongue Extrinsic muscles alter tongue's position Lingual frenulum: attachment to floor of mouth © 2013 Pearson Education, Inc. Tongue Surface bears papillae – Some contain taste buds – All help give traction on food © 2013 Pearson Education, Inc. Figure 23.8 Dorsal surface of the tongue, and the tonsils. Epiglottis Palatopharyngeal arch Palatine tonsil Lingual tonsil Palatoglossal arch Terminal sulcus Foliate papillae Vallate papilla Medial sulcus of the tongue Dorsum of tongue Fungiform papilla Filiform papilla © 2013 Pearson Education, Inc. Salivary Glands • • • • Lie outside oral cavity Parotid Submandibular Sublingual Functions of saliva • • • • Cleanses mouth Dissolves food chemicals for taste Moistens food; compacts into bolus Begins breakdown of starch with enzymes © 2013 Pearson Education, Inc. Figure 23.9 The salivary glands. Tongue Teeth Ducts of sublingual gland Frenulum of tongue Sublingual gland Parotid gland Parotid duct Masseter muscle Body of mandible (cut) Posterior belly of digastric muscle Mylohyoid muscle (cut) Submandibular duct Anterior belly of digastric muscle Submandibular gland © 2013 Pearson Education, Inc. Mucous cells Serous cells forming demilunes Salivary Glands • Two types of secretory cells – Serous cells • Watery, enzymes, ions, bit of mucin – Mucous cells • Mucus • Parotid, submandibular glands mostly serous; sublingual mostly mucous © 2013 Pearson Education, Inc. Composition of Saliva • 97–99.5% water, slightly acidic – Electrolytes—Na+, K+, Cl–, PO4 2–, HCO3– – Salivary amylase and lingual lipase – Mucin – Metabolic wastes—urea and uric acid – Lysozyme, IgA, defensins, and a cyanide compound protect against microorganisms PLAY Animation: Rotating head © 2013 Pearson Education, Inc. Control of Salivation • 1500 ml/day • Intrinsic glands continuously keep mouth moist • Major salivary glands activated by parasympathetic nervous system when – Ingested food stimulates chemoreceptors and mechanoreceptors in mouth – Salivatory nuclei in brain stem send impulses along parasympathetic fibers in cranial nerves VII and IX • Strong sympathetic stimulation inhibits salivation and results in dry mouth (xerostomia) © 2013 Pearson Education, Inc. Teeth Mechanical digestion • Incisors cut • Canines tear or pierce • Premolars (bicuspids) grind & crush • Molars grind & crush © 2013 Pearson Education, Inc. Figure 23.10 Human dentition. Incisors Central (6–8 mo) Lateral (8–10 mo) Canine (eyetooth) (16–20 mo) Molars First molar (10–15 mo) Second molar (about 2 yr) Deciduous (milk) teeth Incisors Central (7 yr) Lateral (8 yr) Canine (eyetooth) (11 yr) Premolars (bicuspids) First premolar (11 yr) Second premolar (12–13 yr) Molars First molar (6–7 yr) Second molar (12–13 yr) Third molar (wisdom tooth) (17–25 yr) © 2013 Pearson Education, Inc. Permanent teeth Number and types of Teeth Primary: Permanent: © 2013 Pearson Education, Inc. Figure 23.11 Longitudinal section of a canine tooth within its bony socket (alveolus). Enamel Dentin Crown Neck Dentinal tubules Pulp cavity (contains blood vessels and nerves) Gingival sulcus Gingiva (gum) Cement Root Root canal Periodontal ligament Apical foramen © 2013 Pearson Education, Inc. Bone Tooth & gum disease Cavities (dental caries) due to destruction of enamel & dentin by lactic acid made by bacteria digesting sugar in a film on tooth surface. Periodontal (gum) disease: affects up to 95% over age 35, accounts for 80-90% of adult tooth loss. Due to bacterial infection btn tooth & gum, preventable by flossing & brushing. College or Department name here Pharynx = throat, passes air and food via sequential contraction of muscles College or Department name here Esophagus • Carries food from throat to stomach, collapsed when empty • Diaphragm and esophageal sphincter (and gravity) keep food in stomach • Heartburn: often due to "gastroesophageal (GE) reflux" (stomach contents spurting up into esophagus), which can be caused by hiatal hernia (top of stomach protrudes above diaphragm) College or Department name here Deglutition=swallowing • Involves coordinated contraction of muscles in tongue, soft palate, pharynx, esophagus • Buccal phase – Voluntary contraction of tongue • Pharyngeal-esophageal phase – Involuntary – primarily vagus nerve – Control center in the medulla and lower pons © 2013 Pearson Education, Inc. Figure 23.13 Deglutition (swallowing) Bolus of food Tongue Uvula Pharynx Bolus Epiglottis Epiglottis Glottis Upper esophageal sphincter Trachea Esophagus 1 During the buccal phase, the upper esophageal sphincter is contracted. The tongue presses against the hard palate, forcing the food bolus into the oropharynx. 2 The pharyngeal-esophageal phase begins as the uvula and larynx rise to prevent food from entering respiratory passageways. The tongue blocks off the mouth. The upper esophageal sphincter relaxes, allowing food to enter the esophagus. 3 The constrictor muscles of the pharynx contract, forcing food into the esophagus inferiorly. The upper esophageal sphincter contracts (closes) after food enters. 5 Relaxed muscles Circular muscles contract Bolus of food 4 Peristalsis moves food through the esophagus to the stomach. Longitudinal muscles contract Relaxed muscles The gastroesophageal sphincter surrounding the cardial oriface opens, and food enters the stomach. Circular muscles contract Gastroesophageal sphincter closed Gastroesophageal sphincter opens Stomach Bolus Stomach: Gross Anatomy Cardia Fundus Body Pyloric region Pyloric sphincter (valve) © 2013 Pearson Education, Inc. Figure 23.14a Anatomy of the stomach. Cardia Fundus Esophagus Muscularis externa • Longitudinal layer • Circular layer • Oblique layer Serosa Body Lumen Lesser curvature Rugae of mucosa Greater curvature Duodenum © 2013 Pearson Education, Inc. Pyloric sphincter (valve) at pylorus Pyloric canal Pyloric antrum Figure 23.30b Mesenteries of the abdominal digestive organs. Liver Gallbladder Lesser omentum Stomach Duodenum Transverse colon Small intestine Cecum Urinary bladder © 2013 Pearson Education, Inc. Figure 23.30c Mesenteries of the abdominal digestive organs. Greater omentum Transverse colon Transverse mesocolon Descending colon Jejunum Mesentery Sigmoid mesocolon Sigmoid colon Ileum © 2013 Pearson Education, Inc. Figure 23.15a Microscopic anatomy of the stomach. Surface epithelium Mucosa Lamina propria Muscularis mucosae Submucosa (contains submucosal Oblique plexus) layer Muscularis Circular externa layer (contains Longitudinal myenteric layer plexus) Stomach wall Serosa Layers of the stomach wall © 2013 Pearson Education, Inc. Figure 23.15b Microscopic anatomy of the stomach. Gastric pits Surface epithelium (mucous cells) Gastric pit Mucous neck cells Parietal cell Gastric gland Chief cell Enteroendocrine cell © 2013 Pearson Education, Inc. Enlarged view of gastric pits and gastric glands Figure 23.15c Microscopic anatomy of the stomach. Pepsinogen Pepsin HCI Mitochondria Parietal cell Chief cell Enteroendocrine cell © 2013 Pearson Education, Inc. Location of the HCl-producing parietal cells and pepsin-secreting chief cells in a gastric gland Gastric Gland Secretions • Parietal cells • Hydrochloric acid (HCl): pH 1.5–3.5 denatures protein, activates pepsin, breaks down plant cell walls, kills bacteria • Intrinsic factor • Glycoprotein required for vitamin B12 absorption • Chief cells • Pepsinogen: Inactive protease; activated to pepsin by HCl and by pepsin itself (positive feedback) • Lipases • Enteroendocrine cells • Serotonin1, histamine1, somatostatin1,2, gastrin2 1. Paracrine (acts locally); 2. Hormone © 2013 Pearson Education, Inc. Mucosal Barrier • Harsh digestive conditions in stomach • Has mucosal barrier to protect – Thick layer of bicarbonate-rich mucus – Tight junctions between epithelial cells • Prevent juice seeping underneath tissue – Damaged epithelial cells quickly replaced by division of stem cells • Surface cells replaced every 3–6 days © 2013 Pearson Education, Inc. Homeostatic Imbalance • Gastritis – Inflammation caused by anything that breaches mucosal barrier • Peptic or gastric ulcers – Erosions of stomach wall • Can perforate peritonitis; hemorrhage – Most caused by Helicobacter pylori bacteria – Some by NSAIDs © 2013 Pearson Education, Inc. Figure 23.16 Photographs of a gastric ulcer and the H. pylori bacteria that most commonly cause it. Bacteria Mucosa layer of stomach A gastric ulcer lesion © 2013 Pearson Education, Inc. H. pylori bacteria Digestive Processes in the Stomach • Mechanical breakdown • Chemical digestion – Denaturation of proteins by HCl – Enzymatic digestion of proteins by pepsin • Propulsion: delivers chyme to small intestine • Absorption: alcohol, aspirin, secretion of intrinsic factor for B12 absorption in S.I. © 2013 Pearson Education, Inc. Neural & Hormonal Regulation of Gastric Secretion • Neural – Vagus nerve activity secretion – Sympathetic activity secretion • Hormonal – Gastrin • Gastrin ⇒ enzyme and HCl secretion • Most small intestine secretions are gastrin antagonists © 2013 Pearson Education, Inc. Phases of Gastric Secretion • Cephalic (reflex) phase: conditioned reflex triggered by aroma, taste, sight, thought • Gastric phase: 3–4 hours – Stimulated by gastrin (from G cells), distension, peptides, low acidity • Intestinal phase – Chyme entering S.I. is initially and briefly stimulatory to stomach – Later, chyme in SI inhibits stomach secretion: enterogastric reflex – Too much chyme entering SI ⇒ dumping syndrome (nausea, vomiting), common after gastric reduction surgery © 2013 Pearson Education, Inc. Figure 23.17 Neural and hormonal regulation of gastric secretion Inhibitory events Stimulatory events Cephalic phase Gastric phase 1 Sight and thought of food Cerebral cortex Conditioned reflex 2 Stimulation of taste and smell receptors Hypothalamus and medulla oblongata 1 Stomach distension activates stretch receptors Vagovagal reflexes Intestinal phase Stimulate Inhibit Vagus nerve Local reflexes 2 Food chemicals G cells (especially peptides and caffeine) and rising pH activate chemoreceptors 1 Presence of partially digested foods in duodenum or distension of the duodenum when stomach begins to empty Medulla Vagus nerve Lack of stimulatory impulses to parasympathetic center Cerebral cortex Gastrin secretion declines G cells Overrides parasympathetic controls Sympathetic nervous system activation 1 Loss of appetite, depression 1 Excessive acidity (pH < 2) in stomach 2 Emotional stress Gastrin release to blood Intestinal (enteric) gastrin release to blood Stomach secretory activity Enterogastric reflex Brief effect Local reflexes Vagal nuclei in medulla Pyloric sphincter Release of enterogastrones (secretin, cholecystokinin, vasoactive intestinal peptide) 1 Distension of duodenum; presence of fatty, acidic, or hypertonic chyme; and/or irritants in the duodenum 2 Distension; presence of fatty, acidic, partially digested food in the duodenum Response of the Stomach to Filling • Stretches to accommodate incoming food – Pressure constant until 1.5 L food ingested • Reflex-mediated receptive relaxation – Coordinated by swallowing center of brain stem – Gastric accommodation • Plasticity (stress-relaxation response) of smooth muscle (see Chapter 9) © 2013 Pearson Education, Inc. Gastric Contractile Activity • Peristaltic waves move toward pylorus at rate of 3 per minute • Distension and gastrin increase force of contraction • Most vigorous near pylorus © 2013 Pearson Education, Inc. Figure 23.19 Deglutition (swallowing). Pyloric valve closed 1 Propulsion: Peristaltic waves move from the fundus toward the pylorus. © 2013 Pearson Education, Inc. Slide 1 Pyloric valve closed 2 Grinding: The most vigorous peristalsis and mixing action occur close to the pylorus. Pyloric valve slightly opened 3 Retropulsion: The pyloric end of the stomach acts as a pump that delivers small amounts of chyme into the duodenum, simultaneously forcing most of its contained material backward into the stomach. Small Intestine: Gross Anatomy • Major organ of digestion and absorption • 2-4 m long; from pyloric sphincter to ileocecal valve • Subdivisions – Duodenum (retroperitoneal) – Jejunum (attached posteriorly by mesentery) – Ileum (attached posteriorly by mesentery) © 2013 Pearson Education, Inc. Figure 23.1 Alimentary canal and related accessory digestive organs. Mouth (oral cavity) Tongue* Parotid gland Sublingual gland Submandibular gland Salivary glands* Pharynx Esophagus Stomach Pancreas* (Spleen) Liver* Gallbladder* Transverse colon Small intestine Anus © 2013 Pearson Education, Inc. Duodenum Jejunum Ileum Descending colon Ascending colon Cecum Sigmoid colon Rectum Appendix Anal canal Large intestine Figure 23.21 The duodenum of the small intestine, and related organs. Right and left hepatic ducts of liver Cystic duct Common hepatic duct Bile duct and sphincter Accessory pancreatic duct Mucosa with folds Tail of pancreas Pancreas Jejunum Gallbladder Major duodenal papilla Hepatopancreatic ampulla and sphincter © 2013 Pearson Education, Inc. Main pancreatic duct and sphincter Duodenum Head of pancreas Small Intestine • Duodenum 0.25 m long; receives bile & pancreatic enzymes; common bile duct, main pancreatic duct join at hepatopancreatic ampulla, enter duodenum at major duodenal papilla, controlled by hepatopancreatic sphincter • Jejunum 2.5 m long • Ileum 3.6 m long; joins large intestine at ileocecal valve © 2013 Pearson Education, Inc. Small Intestine • Innervated by vagus nerve (parasympathetic) and sympathetics from thoracic splanchnic nerves • Blood supply: Superior mesenteric artery • Portal circulation – Capillaries to portal vein to more capillaries: – Nutrient-rich blood from small intestine caps goes by hepatic portal vein to liver & liver capillaries © 2013 Pearson Education, Inc. Structural Features to Increase Surface Area • Circular folds Permanent folds (~1 cm deep) force chyme to slowly spiral through lumen, increases nutrient absorption • Villi Extensions (~1 mm high) of mucosa with capillary bed and lacteal for absorption • Microvilli (brush border) Contain enzymes for carbohydrate and protein digestion © 2013 Pearson Education, Inc. Figure 23.22a Structural modifications of the small intestine that increase its surface area for digestion and absorption. Vein carrying blood to hepatic portal vessel Muscle layers Circular folds Villi © 2013 Pearson Education, Inc. Lumen Figure 23.22b Structural modifications of the small intestine that increase its surface area for digestion and absorption. Microvilli (brush border) Absorptive cells Lacteal Goblet cell Blood capillaries Mucosaassociated lymphoid tissue Intestinal crypt Muscularis mucosae Duodenal gland © 2013 Pearson Education, Inc. Villus Enteroendocrine cells Venule Lymphatic vessel Submucosa Figure 23.22c Structural modifications of the small intestine that increase its surface area for digestion and absorption. Absorptive cells Goblet cells Villi © 2013 Pearson Education, Inc. Intestinal crypt Homeostatic Imbalance • Chemotherapy targets rapidly dividing cells – Kills cancer cells – Kills rapidly dividing GI tract epithelium nausea, vomiting, diarrhea © 2013 Pearson Education, Inc. Mucosa • Peyer's patches protect especially distal part against bacteria – May protrude into submucosa • B lymphocytes leave intestine, enter blood, protect intestinal lamina propria with their IgA • Duodenal (Brunner's) glands of the duodenum secrete alkaline mucus to neutralize acidic chyme © 2013 Pearson Education, Inc. Intestinal Juice • 1-2 L secreted daily in response to distension or irritation of mucosa • Slightly alkaline; isotonic with blood plasma • Largely water; enzyme-poor (enzymes of small intestine only in brush border); contains mucus • Facilitates transport and absorption of nutrients © 2013 Pearson Education, Inc. Accessory Organs: Liver and Gallbladder • Liver – Many functions – Digestive function: produce bile (emulsify fats) – Largest gland • Gallbladder – Chief function: store bile © 2013 Pearson Education, Inc. Figure 23.24a Liver Sternum Bare area Liver Falciform ligament Left lobe of liver Right lobe of liver Gallbladder Round ligament (ligamentum teres) Figure 23.21 Liver, Pancreas, Duodenum Right and left hepatic ducts of liver Cystic duct Common hepatic duct Bile duct and sphincter Accessory pancreatic duct Mucosa with folds Tail of pancreas Pancreas Jejunum Gallbladder Major duodenal papilla Hepatopancreatic ampulla and sphincter Main pancreatic duct and sphincter Duodenum Head of pancreas Figure 23.25a–b Microscopic anatomy of the liver. Lobule © 2013 Pearson Education, Inc. Central Connective vein tissue septum Liver: Microscopic Anatomy • Portal triad at each corner of lobule – Branch of hepatic artery supplies oxygen – Branch of hepatic portal vein brings nutrient-rich blood – Bile duct receives bile from bile canaliculi • Liver sinusoids - leaky capillaries between hepatic plates © 2013 Pearson Education, Inc. Interlobular veins (to hepatic vein) Central vein Microscopic anatomy of the liver Sinusoids Bile canaliculi Plates of hepatocytes Bile duct (receives bile from bile canaliculi) Fenestrated lining (endothelial cells) of sinusoids Stellate macrophages in sinusoid walls Portal vein © 2013 Pearson Education, Inc. Bile duct Portal venule Hepatic arteriole Portal triad Hepatocytes • Abundant rough & smooth ER, Golgi, mitochondria • Process bloodborne nutrients • Store fat-soluble vitamins • Detoxification • Produce ~900 ml bile per day • Regenerative capacity Jean Louis Cesar Lair, 1819 Homeostatic Imbalance • Hepatitis – Usually viral infection, drug toxicity, wild mushroom poisoning • Cirrhosis – Progressive, chronic inflammation from chronic hepatitis or alcoholism – Liver fatty, fibrous portal hypertension • Liver transplants successful, but livers scarce © 2013 Pearson Education, Inc. Bile • Yellow-green, alkaline solution containing – Bile salts = compounds derived from cholesterol. Help emulsify & absorb lipids. – Bilirubin = pigment formed from heme • Brown color of feces due to bilirubin, after bacteria convert it to stercobilin – Cholesterol – Triglycerides, phospholipids, electrolytes – Water © 2013 Pearson Education, Inc. The Gallbladder • Thin-walled muscular sac on ventral surface of liver • Stores and concentrates bile by absorbing water and ions • Muscular contractions release bile via cystic duct, which flows into bile duct • “Biliary tree” = gall bladder plus the ducts © 2013 Pearson Education, Inc. Gallstones • Cholelithiasis = gallstone formation • “Stones” are crystals of compounds found in bile • Most gallstones are cholesterol stones – Bile salts help keep cholesterol in solution – Cholesterol stones more likely to form if bile is low in bile salts • Obstruct flow of bile from gallbladder • May cause pain, obstructive jaundice, fat malabsorption, diarrhea, … • Tx: drugs, lithotripsy, minimally invasive removal • If recurrent: cholecystectomy = gall bladder removal – Many patients do OK without a gall bladder (must modify diet) – Some have pain, diarrhea, bloating, etc Pancreas • Mostly retroperitoneal, deep to greater curvature of stomach; head by duodenum, tail by spleen • Endocrine: pancreatic islets secrete insulin and glucagon • Exocrine: secretes pancreatic juice – To duodenum via main pancreatic duct – Zymogen granules contain proenzymes – Secreted in inactive form, activated in gut © 2013 Pearson Education, Inc. Figure 23.26a Enzyme-producing tissue of pancreas Small duct Acinar cell Basement membrane Zymogen granules Rough endoplasmic reticulum Duct cell One acinus Pancreatic Juice • 1200-1500 ml/day, alkaline (pH 8, HCO3-) neutralizes chyme • Enzymes – Amylase, lipases, nucleases secreted in active form but require ions or bile for optimal activity – Proteases secreted in inactive form, activated in duodenum – Trypsinogen activated to trypsin by brush border enzyme enteropeptidase – Procarboxypeptidase, chymotrypsinogen activated by trypsin © 2013 Pearson Education, Inc. Figure 23.27 Activation of Pancreatic Proteases in Small Intestine Stomach Pancreas Epithelial cells Membrane-bound enteropeptidase Trypsinogen (inactive) © 2013 Pearson Education, Inc. Trypsin Chymotrypsinogen (inactive) Chymotrypsin Procarboxypeptidase (inactive) Carboxypeptidase Regulation of Bile Secretion • Bile secretion stimulated by secretin from intestinal cells • Gallbladder contraction stimulated by – Cholecystokinin (CCK) from intestinal cells exposed to acidic, fatty chyme – Vagal activity • CCK also causes – Secretion of pancreatic juice – Hepatopancreatic sphincter to relax © 2013 Pearson Education, Inc. Regulation of Pancreatic Secretion • CCK induces secretion of enzyme-rich pancreatic juice by acini • Secretin causes secretion of bicarbonaterich pancreatic juice by duct cells • Vagal stimulation also causes release of pancreatic juice (minor stimulus) © 2013 Pearson Education, Inc. Figure 23.28 Promotion of Bile and Pancreatic Juice Secretion and Release 1. Chyme entering duodenum causes duodenal enteroendocrine cells to release cholecystokinin (CCK) and secretin. 2. CCK (red dots) and secretin (yellow dots) enter blood. 3. CCK, secretin induce pancreatic juice secretion. 4. Bile salts & secretin stimulate liver to produce more bile. 5. CCK causes gallbladder to contract and hepatopancreatic sphincter to relax; bile enters duodenum. 6. During cephalic and gastric phases, vagus nerve activity causes weak gallbladder contractions. CCK secretion Secretin secretion Digestion in the Small Intestine • Chyme from stomach contains – Partially digested carbohydrates and proteins – Undigested fats • 3–6 hours in small intestine – Most water absorbed – ~ All nutrients absorbed • Small intestine, like stomach, no role in ingestion or defecation © 2013 Pearson Education, Inc. Requirements for Digestion and Absorption in the Small Intestine • Slow delivery of acidic, hypertonic chyme • Delivery of bile, enzymes, and bicarbonate ions from liver and pancreas • Mixing © 2013 Pearson Education, Inc. Motility of the Small Intestine • Segmentation – Most common motion of small intestine – Initiated by intrinsic pacemaker cells – Mixes/moves contents toward ileocecal valve – Intensity altered by long & short reflexes; hormones • Parasympathetic ; sympathetic – Wanes in late intestinal (fasting) phase © 2013 Pearson Education, Inc. Motility of the Small Intestine • Peristalsis – Initiated by rise in hormone motilin in late intestinal phase; every 90–120 minutes – Each wave starts distal to previous • Migrating motor complex – Meal remnants, bacteria, and debris moved to large intestine – From duodenum ileum ~ 2 hours © 2013 Pearson Education, Inc. Figure 23.3a Peristalsis and segmentation. From mouth © 2013 Pearson Education, Inc. Peristalsis: Adjacent segments of alimentary tract organs alternately contract and relax, moving food along the tract distally. Motility of the Small Intestine • Local enteric neurons coordinate intestinal motility • Cholinergic sensory neurons may activate myenteric plexus – Causes contraction of circular muscle proximally and of longitudinal muscle distally – Forces chyme along tract © 2013 Pearson Education, Inc. Motility of the Small Intestine • Ileocecal sphincter relaxes, admits chyme into large intestine when – Gastroileal reflex enhances force of segmentation in ileum – Gastrin increases motility of ileum • Ileocecal valve flaps close when chyme exerts backward pressure – Prevents regurgitation into ileum © 2013 Pearson Education, Inc. Large Intestine Cecum: connects to ileum at ileocecal valve Appendix: part of MALT of immune system Colon: more below Rectum Anal canal • Opens to body exterior at anus • Internal anal sphincter—smooth muscle • External anal sphincter—skeletal muscle © 2013 Pearson Education, Inc. Unique features of Large Intestine • Teniae coli Three bands of longitudinal smooth muscle in muscularis • Haustra Pocketlike sacs created by tone of teniae coli • Epiploic appendages Fat-filled pouches of visceral peritoneum © 2013 Pearson Education, Inc. Figure 23.29a Large Intestine Left colic (splenic) flexure Right colic (hepatic) flexure Transverse mesocolon Transverse colon Epiploic appendages Superior mesenteric artery Descending colon Haustrum Ascending colon IIeum Cut edge of mesentery IIeocecal valve Tenia coli Sigmoid colon Cecum Appendix Rectum Anal canal © 2013 Pearson Education, Inc. External anal sphincter Colon • Retroperitoneal except for transverse and sigmoid regions • Ascending colon (right side – to level of right kidney) • Transverse colon • Descending colon • Sigmoid colon in pelvis rectum © 2013 Pearson Education, Inc. Figure 23.30c Mesenteries of the Abdomen Greater omentum Transverse colon Descending colon Jejunum Mesentery Sigmoid colon Ileum Figure 23.30d Mesenteries of the Abdomen Liver Lesser omentum Pancreas Stomach Duodenum Transverse mesocolon Transverse colon Mesentery Greater omentum Jejunum Ileum Visceral peritoneum Parietal peritoneum Urinary bladder Rectum Figure 23.29b Rectum and Anus Rectum Hemorrhoidal veins Anal canal External anal sphincter Internal anal sphincter Anus Bacterial Flora • Enter from small intestine or anus – Colonize colon – Synthesize B complex vitamins and vitamin K – Metabolize some host-derived molecules (mucin, heparin, hyaluronic acid) – Ferment indigestible carbohydrates – Release irritating acids and gases (~500 ml/day) © 2013 Pearson Education, Inc. Digestive Processes in the Large Intestine • Residue remains in large intestine 12–24 hours • No food breakdown except by enteric bacteria • Vitamins (made by bacterial flora), water, and electrolytes (especially Na+ and Cl–) reclaimed • Major functions - propulsion of feces to anus; defecation • Colon not essential for life © 2013 Pearson Education, Inc. Large Intestinal Motility • Most colonic activity is haustral contractions – Slow segmenting movements • Gastrocolic reflex – Initiated by presence of food in stomach – Activates three to four slow powerful peristaltic waves per day in colon (mass movements) © 2013 Pearson Education, Inc. Homeostatic Imbalance • Irritable bowel syndrome – Functional GI disorder – Recurring abdominal pain, stool changes, bloating, flatulence, nausea, depression – Stress common precipitating factor • Stress management important in treatment © 2013 Pearson Education, Inc. Figure 23.31 Defecation Reflex Impulses from cerebral cortex (conscious control) Sensory nerve fibers Voluntary motor nerve to external anal sphincter Sigmoid colon External anal sphincter (skeletal muscle) Rectum 1 Feces move into and distend the rectum, stimulating stretch receptors there. The receptors transmit signals along afferent fibers to spinal cord neurons. Stretch receptors in wall 2 A spinal reflex is initiated in which parasympathetic motor (efferent) fibers stimulate contraction of the rectum and sigmoid colon, and relaxation of the internal anal sphincter. Involuntary motor nerve (parasympathetic division) Internal anal sphincter (smooth muscle) 3 If it is convenient to defecate, voluntary motor neurons are inhibited, allowing the external anal sphincter to relax so feces may pass.