Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
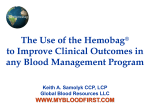
Date Name MRN, DOB Location Mount Sinai Hospital New York, NY 10029 APHERESIS UNIT (212) 241-6104 Physician/Service THERAPEUTIC APHERESIS ORDER SET Patient Diagnosis: _________________________ Patient Age: _______ Referring MD____________________ Vital sign frequency: Routine q1° Location of procedure: Apheresis Unit Other: ______________ Apheresis instrument: Spectra Other_______________ Apheresis Schedule/Frequency: Continuous _____________________________________ Plasmapheresis: Plasma volumes to exchange ___________ Replacement fluid: Red cell exchange: Cytoreduction: Replacement fluid: Anticoagulant: Patient: 5% Albumin___________% 0.9% NaCl ___________ % FFP____________ % Cryo-poor plasma ________% PRBC volumes to exchange ___________ Average Hct of red cell units_______ End point patient Hct__________% Desired FCR___________% WBC Target cell count: Fluid balance desired: ___________ Platelets _________________ Blood volumes for processing: ______________ 5% Albumin______% ACD-A 0.9% NaCl ___________ % FFP____________ % Heparin: ________U/500 mL ACD-A and AC: WB ratio ___________ Weight ____________ lb / kg Safe ECV _________________ mL Height ___________ in / cm Red cell prime: TBV ______________mL Undiluted Diluted Hb/Hct ________ Plts_________ WBC_________ PT/aPTT ___________Serum Ca _______ LFTs _______ Labs to order: Pre______________________________________ □ADMTS-13 (vWFPA) □T & S Post______________________________________ Medications: ______ mL 10% Calcium gluconate (94 mg/mL) in 150mL NS for continuous drip throughout procedure Benadryl IV/po ________mg Tylenol po ___________mg Heparin dwell ________units per lumen. Solu-Cortef/Medrol IV_______mg Sterile dressing change, as needed. Special instruction/comments: ________________________________________________________________________ ____________________________________________________________________________________________ ____________________________________________________________________________________________ Attending Signature _______________________________ Date/Time ____________________ Nurse’s Signature _________________________________ Date/Time____________________ APH 507v2 Page 1 of 2 Physician’s Additional Instructions Date/Time____________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________________________________________________ APH 507v2 Page 2 of 2