Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
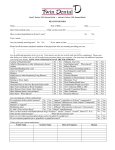
PATIENT REGISTRATION NEUROLOGY ASSOCIATES, P.C. DATE________________ Patient’s Name(Last)_____________________________(First)________________________(M.I.)_______ Responsible Party if Under Age 18:_________________________Race_________Ethnicity____________ SSN:__________________________ Sex: Male____Female_____ Birth Date:______________________ Marital Status: Single________Married________Divorced_______Widowed_______Separated________ Street/Billing Address:_____________________________________________________________________ City:_______________________________________State:_____________Zip:______________-_________ Home Phone:__________________Cell Phone:____________________Work Phone:__________________ Occupation:___________________________Employer’s Name:___________________________________ Referring Physician:__________________________Primary Care Physician:________________________ What is the reason for your evaluation today?__________________________________________________ What is your preferred pharmacy?___________________________________________________________ List any medication allergies:________________________________________________________________ Do you have an allergy to Latex? Yes_____No_____ Preferred Spoken Language___________________ PRIMARY CONTACT PERSON (SPOUSE, PARENT, SIGNIFICANT OTHER, ETC.) Name:__________________________________Relationship:___________________DOB:______________ Address:__________________________________________________Employer:______________________ Home Phone:____________________Cell Phone:__________________Work Phone:__________________ ____Yes____No I give the physicians/staff of NAPC permission to discuss my medical information with this individual. ASSIGNMENT OF BENEFITS AND AUTHORIZATION TO RELEASE MEDICAL INFORMATION I hereby assign all medical benefits, to include major medical benefits to which I am entitled, including Medicare, private insurance, and any other health plan to Neurology Associates, P.C. This assignment will remain in effect until revoked by me in writing. A photocopy of this assignment is to be considered as valid as the original. I understand that I am financially responsible for all charges whether or not paid by said insurance. Should it become necessary to turn my account over to an outside collection agency, I will be responsible for collection costs, attorney fees, litigation fees, and court costs. I hereby authorize Neurology Associates, P.C. and its employees and agents TO RELEASE ALL INFORMATION, reports, and records if necessary for the purposes of treatment, payment and healthcare operations, including a discussion of my medical condition, to the insurance provider, rehabilitation provider, employer, hospitals, and doctors. If I have a liability injury, I understand that I have the option of using my health insurance, if available, or I will be expected to pay for treatment. I acknowledge that I have been offered a copy of Neurology Associates, P.C. Notice of Privacy Practice Policy, which describes how my health insurance information may be used or disclosed. Signature:_________________________________________________Date:__________________________ Responsible Person if Patient is a Minor:___________________________________Date:______________ Form NA 99-1 Name_________________________ Date:_____________ SOCIAL HISTORY Marital Status: Are you currently married? ______No ______Yes Education: How many years of school have you completed?_______ Occupation: Your current employment status: ______Retired ______Homemaker ______Employed Current Occupation(s):___________________________________ Are you disabled? ______No ______Yes Applying for disability? _____No _____Yes MEDICATIONS Please list any medications you are currently taking including any prescription and/or non-prescription medications including vitamins, nutritional supplements, oral contraceptives, pain relievers, etc. Name of Medication Dose How often Taken (Please attach additional paper if more space is needed) ALLERGIES Please list any medications for which you have had an allergic reaction (hives, skin rash, breathing problems, etc.) Name of Medication Describe Allergic Reaction Have you had an allergic reaction to: Iodine or X-ray contrast dye? ____No ____Yes Do you have an allergy to Latex? ____No ____Yes Initial_______ Page 1 Form NA 99-1 Name_________________________ Date:_____________ Have you ever used any of the following substances? Substance Currently use? Previously used? Caffeine _____ Yes _____ No _____ Yes _____ No Tobacco _____ Yes _____ No _____ Yes _____ No Alcohol _____ Yes _____ No _____ Yes _____ No Recreational/ Street Drugs _____ Yes _____ No _____ Yes _____ No Type/Amount/Frequency How Long? (Years) When Stopped? FAMILY HISTORY Family Members Father Living? Present Health Cause of Death Age _____ Yes _____ No Mother _____ Yes _____ No Brother(s) _____ Yes _____ No Sister(s) _____ Yes _____ No Circle any illnesses that have occurred in your blood relatives: Cancer Heart Disease Asthma Stroke Diabetes Blackouts Kidney Disease Seizures Migraines High cholesterol Tremor Mental disorder Nervous Disorder High blood pressure Thyroid Other Hereditary diseases________________________________________________________________ Initial_______ Page 2 Form NA 99-1 Name_________________________ Date:_____________ REVIEW OF SYSTEMS Please indicate whether you have experienced the following symptoms during recent months, unless otherwise specified, by checking “No” or “Yes” for each question. Circle the symptoms(s) you have experienced when multiple symptoms are listed in a question. 1) 2) 3) 4) Skin rash, sore, excessive bruising or change of a mole? Excessive thirst or urination? Change in sexual drive or performance? Significant headaches, seizures, slurred speech or difficulty moving an arm or leg? 5) Eye problems such as double or blurred vision, cataracts, or glaucoma? 6) Diminished hearing, dizziness, hoarseness or sinus problems? 7) Bothered with cough, shortness of breath, wheezing, or asthma? 8) Coughing up sputum or blood? 9) Exposed to anyone with tuberculosis? 10) ‘Blacked out’ or lost consciousness? 11) Chest pain or pressure, rapid or irregular heart beats, or known difficulty with a heart valve? 12) Awakening at night with shortness of breath? 13) Abnormal swelling in the legs or feet? 14) Pain in the calves or your legs when you walk? 15) Difficulty with swallowing, heartburn, nausea, vomiting, or stomach trouble? 16) Significant problems with bowel movements (i.e. constipation, diarrhea, or blood in the stool)? 17) Difficulty starting your urinary stream, completely emptying your bladder, or leaking urine? 18) Burning or pain when urinating? 19) Pain, stiffness, or swelling in your back, joints, or muscles? 20) Fever within the last month? 21) Enlarged glands (lymph nodes)? 22) Feel you are at risk for HIV or AIDS? 23) Immunized for influenza, tetanus/diphtheria and/or pneumonia within the last year? 24) Experiencing an unusually stressful situation? 25) Weight gain or loss of more than 10 lbs during the last 6 months? 26) Problems falling asleep, staying asleep, sleep apnea, or disruptive snoring? 27) Abnormal nipple discharge or breast lump? 28) Have you ever felt a need to cut down on your alcohol consumption? 29) Do relatives/friends worry or complain about your alcohol consumption? 30) Have you been physically, sexually, or emotionally No Yes ___ ___ ____ ____ ____ ____ ____ ____ Space below for physicians use 1)_________________________ 2)_________________________ 3)_________________________ 4)_________________________ ____ ____ 5)_________________________ ____ ____ 6)_________________________ ____ ____ 7)_________________________ ____ ____ ____ ____ ____ ____ ____ ____ 8)_________________________ 9)_________________________ 10)________________________ 11)________________________ ____ ____ ____ ____ ____ ____ ____ ____ 12)________________________ 13)________________________ 14)________________________ 15)________________________ ____ ____ 16)________________________ ____ ____ 17)________________________ ____ ____ ____ ____ 18)________________________ 19)________________________ ____ ____ ____ ____ ____ ____ ____ ____ 20)________________________ 21)________________________ 22)________________________ 23)________________________ ____ ____ ____ ____ 24)________________________ 25)________________________ ____ ____ 26)________________________ ____ ____ ____ ____ 27)________________________ 28)________________________ ____ ____ 29)________________________ ____ ____ 30)________________________ Form NA 99-1 abused? Initial_______ Name_________________________ Date:_____________ Page 3 PAST MEDICAL HISTORY Have you had any of the following conditions? No Yes Space below for physicians use 1) Abnormal chest X-ray 2) Anxiety, depression, or mental illness 3) Blood problems (abnormal bleeding, anemia, high or low white count) 4) Diabetes 5) High blood pressure 6) High cholesterol or triglycerides 7) Stroke or TIA 8) Heart problems (MI, arrhythmia, pacer) 9) Treatment for alcohol or drug abuse 10) Tuberculosis or positive TB skin test 11) Growth removed from the colon or rectum ____ ____ ____ ____ ____ ____ 1) _______________________ 2) _______________________ 3) _______________________ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ 4) _______________________ 5) _______________________ 6) _______________________ 7) _______________________ 8) _______________________ 9) _______________________ 10) ______________________ 11) ______________________ Please indicate whether you have ever had a medical problem and/or surgery related to each of the following by placing a check mark in the appropriate box(es). If you have had surgery, indicate the approximate year(s) of surgery. Circle the appropriate choice when multiple choices are listed in a question. No problem Medical problem Surgery Year of surgery Space for physicians use 1) Eyes (cataracts, glaucoma) 2) Ears, nose, sinuses, or tonsils 3) Thyroid or parathyroid glands 4) Heart valves or abnormal rhythm 5) Arteries (aorta, arteries to the head, arms, or legs) 6) Veins or blood clots 7) Lungs 8) Esophagus or stomach (ulcer) 9) Bowel (small and large intestine) appendix, or hernia 10) Liver or gallbladder disease 11) Pancreas 12) Lymph nodes or spleen 13) Kidney or bladder 14) Bones, joints, or muscles 15) Back, neck, or spine 16) Brain 17) Skin 18) Breasts 19) Females: uterus, tubes, ovaries 20) Males: prostate, penis, testes, vasectomy ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ______ ______ ______ ______ ______ 1)___________________ 2)___________________ 3)___________________ 4)___________________ 5)___________________ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ______ ______ ______ ______ 6)___________________ 7)___________________ 8)___________________ 9)___________________ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ____ ______ ______ ______ ______ ______ ______ ______ ______ ______ ______ ______ 10)__________________ 11)__________________ 12)__________________ 13)__________________ 14)__________________ 15)__________________ 16)__________________ 17)__________________ 18)__________________ 19)__________________ 20)__________________ Form NA 99-1 Page 4 Initial_______ Name_________________________ Date:_____________ NEUROLOGIC REVIEW Please circle the appropriate response. Handedness: Right or Left Indicate whether you have experienced the following symptoms during recent months by checking ‘No’ or ‘Yes' for each question. Circle the symptoms you have experienced when multiple symptoms are listed. 1) 2) 3) 4) 5) Headache, nausea, vomiting History of seizures or blackouts Numbness, tingling, pain Weakness, cramps, muscle twitching Difficulty walking, incoordination, Involuntary movements 6) Change in vision, hearing, taste, or smell 7) Double vision, drooping of the eyelids 8) Dizziness, lightheadedness, vertigo, ringing in the ears 9) Difficulty with speech or swallowing 10) Difficulty with bowel or bladder control 11) Difficulty with memory, change in behavior or mood 12) Difficulty sleeping, loss of appetite, weight loss or gain No Yes Space below for physicians ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ 1) ____________________ 2) ____________________ 3) ____________________ 4) ____________________ 5) ____________________ ___ ___ ___ ___ ___ ___ 6) ____________________ 7) ____________________ 8) ____________________ ___ ___ ___ ___ ___ ___ 9) ____________________ 10) ___________________ 11) ___________________ ___ ___ 12) ___________________ 13) Have you had any of the procedures performed listed below? If so, when and where? CT Scan MRI Scan Myelogram Carotid dopplers EEG ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ _____________________ _____________________ _____________________ _____________________ _____________________ ______________________________ PHYSICIAN SIGNATURE Page 5