Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
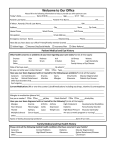
Park Avenue Dermatology Patient Name______________________________________ Date__________________ Sex____M____F Age_____ Height_____ Weight______ Are you allergic to any medications? ___yes ___no If yes please list below: 1.________________________ 2._________________________ 3.________________________ 4._________________________ List ALL medications you are currently taking (including prescriptions, over the counter, vitamins, and herbals): 1.________________ 2._________________ 3.________________ 4.________________ 5._________________ 6.________________ 7.________________ 8._________________ 9.________________ Do you have now, or have you ever had any of the following diseases or conditions: (please circle Y for yes and N for no) Lungs: Bronchitis Emphysema Asthma Chronic Cough Morning Cough Shortness of Breath Wheezing Cardiovascular: High Blood Pressure Chest Pain Heart Attack Heart Murmur Irregular Heartbeat Phlebitis Inflammation of vein Blood clots Pacemaker YES NO Y Y Y Y Y Y Y N N N N N N N YES Y Y Y Y Y Y Y Y NO N N N N N N N N Y N Skin: (please circle your answer) When you are exposed to sun do you: Have you ever had skin cancer? Malignant Melanoma? Has anyone in your family had skin cancer? Malignant Melanoma? Other Systemic: YES Diabetes Excessive thirst/hunger Thyroid Kidney Bladder Frequency/Burning Gastrointestinal/Stomach absorptive disorder Nausea, vomiting, diarrhea when taking antibiotics Yeast infection when taking antibiotics Arthritis/Joint Deformity Arthralgia Limited Motion Artificial joint Convulsions, Epilepsy, or Seizures Fainting Tan only Yes Yes Yes Yes NO Y Y Y Y Y Y N N N N N N Y N Y N Y Y Y Y Y N N N N N Y Y N N Tan and burn No No No No Burn If yes, who?____________________________________________________________________________ Do you have a history of any specific skin disease? (please circle your answer) YES NO If yes, please list:________________________________________________________________________ Are you currently receiving any treatment for any specific skin diseases? YES NO (please circle your answer) If yes, please list any treatment, including the name of the physician treating you and any medications you are currently using (prescription, over the counter, or herbal):____________________________________ _____________________________________________________________________________________ Do you develop skin rashes in reaction to _____Food or _____Environment? If yes, please list any know foods or environmental factors that produce rashes:______________________ ______________________________________________________________________________________ List any other diseases or conditions:________________________________________________________ List any surgical procedures you have had in the last 6 months:___________________________________ ______________________________________________________________________________________ Social History: (circle your answer) Do you drink alcohol? YES NO If yes, __________drinks per day. Do you use IV drugs? YES NO If yes, what?_________How much?_____ Do you smoke? YES NO If yes, _________packs per day. Do you “dip” or “chew” YES NO If yes, what?_________How much?______ Do you have AIDS or have you ever been exposed to HIV(AIDS)? YES NO Do you bleed easily? YES NO (Women)Are you pregnant or breastfeeding? ________________________________________ Patient or Guardian signature Date YES NO ____________________________________ Reviewed by Date