Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
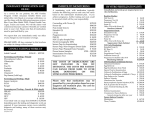
OSPITAL NG MAYNILA MEDICAL CENTER DEPARTMENT OF PEDIATRICS Quirino Ave. corner Roxas Blvd., Malate, Manila Patient’s Name: Address: Age/Sex: Date Admitted: Admitting Diagnosis: Physicians-in-charge: Junior Intern-in-charge: Mendoza, Bb. Boy 2312A Agusdo St., San Miguel, Manila Newborn/Boy May 2, 2009 Hypoxic-Ischemic Encephalopathy Drs. Nunez/Cortes/Reyes JI Narciso/Nepomuceno/Nosa/Ocampo/Odevilas Hospital No.: 649229 Patient Discharge Summary HISTORY OF PRESENT ILLNESS This is a case of a newborn live baby boy born full term to a 26 year old G1P1 (1-0-0-1) mother, 40-41 weeks AOG via LTCS x breech at OMMC. Patient was subsequently admitted due to subcostal retractions and alar flaring. Prenatal History: Patient’s mother had a total of 5 prenatal check ups at OMMC Health Center. Patient had CBC, blood typing, urinalysis, and ultrasonography, all with normal results. Mother had intake of multivitamins and ferrous sulfate during her pregnancy. Mother denied any use of illicit drugs, teratogenic substances nor any exposure to radiation during her pregnancy. Mother had pre-eclampsia, during her pregnancy. She had gestational hypertension (unknown BP) but did not experience DM, thyroid problems, asthma, and history of twinning. Obstetrical History G1P0 (1-0-0-0) G1 Present pregnancy PHYSICAL EXAMINATION General: good activity, good cry and good tone. Vital Signs: HR: 130 bpm RR: 40 cpm Temp: 37.3 °C HC: 34 CC: 31 AC: 28 AS: 2, 2 BW: 2.6 kg BL: 49 cm BS: 40-41 weeks AOG Skin: pink color, good skin turgor, (-) rashes, (-) hematoma, (-) desquamation Head: (+) caput, (-) molding, (-) craniotabes, (-) cephalhematoma, Face: (-) asymmetry, ENT: (-) conjunctivitis, (-) discharge, (+) patent nose, (-) cleft lip, (-) cleft palate Chest and Lungs: (+) breast bud, (-) clavicular fracture, (+) NRRR, clear breath sound Abdomen: flat, (-) masses Genitalia: normal Extremities: (-) cyanosis, (-) edema, (-) polydactylism, (-) syndactylism, (-) club foot, (+) full and equal pulses ASSESSMENT: Live baby boy born full term to a 26 year old G1P1 (1-0-0-1) mother, 40-41 weeks AOG via LTCS x breech at OMMC Hypoxic-Ischemic Encephalopathy . Course in the Wards: Patient was admitted at NICU under the services of Dr. Juico/Salloman/Ang/Manalo/Lucas. Patient was placed on NPO temporarily. Patient was intubated with ET size 3.5 level 10-11. Patient was ambubagged and given FiO2 100%. IVF given was D10 water 156 cc for 24 hours to run at a rate of 6-7 ugtts/min. Diagnostics were: CBC with PC, CXR APL, blood CS and ABG. Therapeutics given were ampicillin 65 mg TIV every 6 hours (100 mkday) and Gentamycin 13 mg IV given OD (5 mkday). The patient is being watched for progression of respiratory distress. The patient was kept thermoregulated, and vital signs were monitored every hour. At 3 pm, the patient was active with good activity. Ampicillin was revised to 150g SIVP every 12 hours. Ranitidine 3 g q8 was started. HCO3 7 meqs + 7 mL of distilled water was given thru SIVP. FiO2 was decreased to 80% and RR to 55. Mouth and ET were suctioned as needed. On the second hospital day, the patient was active with good cry and good activity. Patient was still intubated. No retractions were noted. Abdomen was soft. Patient was maintained on NPO. IVF was D10W 182 cc for 24 hours to run at a rate of 7-8 ugtts/min. Mech vent set up was maintained. Medications were given: Ampicillin D1, Gentamicin D1, Ranitidine. ABG was done. Secretions were suctioned q4. The patient was kept thermoregulated at all times. If ABG’s are OK, FiO2 will be decreased by 5 alternate with RR by 2 every 2 hours until FIO2 is 40 and RR is 20. At 9 PM, NaHCO3 4 meqs + equal amount of DW SIVP was given. On the third hospital day, the patient was noted to have minimal retractions and occasional crackles. The patient was maintained on NPO and Hgt was done once a day. IVF was D10W 208 cc to run at a rate of 8-9 ugtts/min. Medications were shifted to Piptazo 260 mg TIV q12 and Amikacin 39 mg TIV q24. ABG was done. Secetions were suctioned q1. The patient was thermoregulated. Portable x ray was done. On the fourth hospital day, the patient had spontaneous movement and spontaneous breathing. No cyanosis noted nor alar flaring was noted. The patient had minimal retractions and occasional wheezes. OGT feeding was started at 5 cc 6. The patient was being watched for feeding intolerance or vomiting. Medications were maintained as ordered. Secretions were suctioned as needed. On the fifth hospital day, the patient was comfortable with good activity. No retractions were noted. Milk feeding at 5 cc q6 thru OGT was given. IVF was revised to D10W 260 cc for 24 hours to run at 10-11 ugtts/min. IV medications were continued: Piptazo D1, Amikacin D1, Ranitidine. Secretions were suctioned as needed. At 3:30 PM, the patient had good cry and god activity. Patient was extubated, and O2 support was maintained via O2 hood at 10 Lpm. Patient was placed on NPO temporarily for 24 hours. OGT was inserted. Secretions were suctioned as needed. At 7 PM, patient was transferred to isolation room due to growth on Burkholderia cepacia. Piptazo and Amikacin was shifted to meropenem 60 mg TIV q12. On the sixth hospital day, the patient was active and comfortable. No cyanosis nor retractions were noted. Milk feeding was started at 5 cc q4 with SAP. IVF was revised to D10W 286 cc to run for 24 hours at the rate of 11-12 ugtts/min. O2 support via funnel at 4-6 Lpm was given. Meropenem was revised to 80 mg TIV q12. The patient is subjected to minimal handling. The patient was kept thermoregulated. On the seventh hospital day, the patient was active and comfortable. No cyanosis nor retractions were noted. Milk feeding was increased to 10 cc q3 with SAP. IVF was shifted to D5IMB 282 cc for 24 hours to run at a rate of 11-12 ugtts/min. Medications were continued: Meropenem D1, Amikacin D3. O2 support was discontinued. Ranitidine was discontinued. The patient was kept thermoregulated. SUMMARY OF LABORATORY RESULTS CBC WBC neutrophils lymphocytes monocytes eosinophils Basophils RBC HGB HCT MCV MCH MCHC Platelet RDW ABG pH pCO2 pO2 HCO3 TCO2 BEb O2St 5/2 15 42.2 46.5 10.0 1.3 0.0 4 170 0.49 112 38 34 201 18 5/2 7.292 32.30 192.00 15.80 16.80 -9 99.60 Blood CS: (+) for Burkholderia cepacia 5/3 7.331 36.00 48.00 19.20 20.30 -5.4 81.10 5/4 7.47 27.80 72.00 20.40 21.20 -1.3 95.60