Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
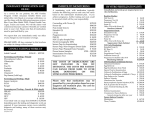
2016 IN VITRO FERTILIZATION FINANCIAL AGREEMENT Patient’s Name _________________________________ DOB_____________SS#_______________________ Spouse/Partner’s name ___________________________ We are requesting to have an in vitro fertilization procedure performed at the Colorado Center for Reproductive Medicine. We understand the following payment policies are in effect at the Center (Financial Agreement and deposit must be received together). Faxed copy can replace the original. In order to be placed on the IVF procedure waiting list, we must make a $1,000 refundable deposit to reserve a place in the current or upcoming session. The $1,000 is applied toward the IVF cycle fees upon completion. If we do not proceed, the $1,000 will be applied to any outstanding charges and remaining amount refunded. There is a minimum $200 patient coordination fee assessed for canceling the cycle prior to beginning mediation. See the canceled cycle fee breakdown for charges assessed for a canceled cycle once medications have begun. All fees for the IVF procedure must be paid in full before beginning any medications for the IVF cycle. This is usually 21 days before the actual IVF procedure is done. There will be NO reduction in the package pricing for any services provided outside our Center. The cycle will be cancelled if the entire IVF payment is not made before the medications are started. The IVF package fees are: $14,630 CCRM’S IVF PackagePackage starts at Lupron consult and ends after first pregnancy test CCRM $ 8,815 Fertility Laboratories of Colorado (FLC) $ 5,815 South Denver Anesthesia Services $ 430 Medications (paid directly to the pharmacy of your choice) $ 3,500 to $ 6,500 approximate Total Estimated Cost of IVF Cycle: $18,560 to $21,560 Additional Services – Not included in package price are: IVF work-up completed prior to IVF cycle $ 4,900 approximately ICSI $ 2,780 IMSI (used with ICSI) $ 515 PICSI (used with ICSI) $ 515 Back-Up Sperm Freeze $ 115 CCS (first 10 embryos) $ 7,075 Testing on embryos over 10 $ 500 per embryo Embryo freezing: Paid to Fertility Laboratories of Colorado $ 975 MESA/Testes Biopsy/PESA/Microdissection varies Pregnancy: First 8 weeks-2nd positive pregnancy test to transfer of care - varies If your cycle results in a freeze-all, you will owe additional fees at time of embryo transfer. If we participate with your insurance and your plan covers IVF, you must obtain written verification of your coverage from them prior to you starting the medications. If you have insurance coverage and we participate with your insurance, you will still owe some fees. Our Surgery Center and FLC are not contracted with any insurance company except United HealthCare, and these services will need to be pre-paid. Please contact the Business Office for the break-down of non-billable fees you will owe. If you do have IVF coverage but we do not participate with your insurance, you will need to prepay the entire cycle. Please request the claim forms from the business office two weeks after embryo transfer to submit to insurance for reimbursement. The Business Office staff is available at 303-781-1085 to answer any questions. We have reviewed and approved the above treatment estimate, payment agreement and terms & conditions. We understand that we are fully responsible for making the payments as outlined. We understand that these prices are subject to change without notice. Patient’s Signature ___________________________Partner’s Signature ___________________________Date ___________ Credit card: VISA____________________ M/C __________________ DISCOVER _______________ exp. date ________ or check #_____________ 3 digit security code________ For Business Office Use Only: Account Number ____________________ $1,000 refundable deposit received ______________ via _________ Business Office Signature______________________ (white copy to business office, yellow copy to patient) sharepoint\sd\businessoffice\financialagreements2016\ivf revised 12-14-15