Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
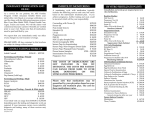
The use of GnRH antagonist for COH as a second line strategy in IVF or ICSI van Os HC, and Jansen CAM. Dept of IVF, Reinier de Graaf hospital Group, loc Diaconessenhuis Voorburg, The Netherlands. Introduction: The use of GnRH agonists has become widespread for Controlled Ovarian Hyperstimulation (COH) in ART treatments. However not all patients respond well, and GnRH agonists often prolong the stimulation as well as introduce a higher risk of the ovarian hyperstimulation syndrome. Some of the disadvantages can be obviated with the use of GnRH antagonists. However all prospective randomised phase III studies have shown lesser pregnancy rates in antagonist cycles, and the question remains whether this is inherent to the medication, due either to the patient population or to the experience with follicle stimulations in antagonist cycles. It still has to be shown whether a select group of patients might benefit specifically from the use of GnRH antagonists. Materials and Methods: Between October 1997 and November 1998 we performed a prospective study with COH using the GnRH antagonist cetrorelix (ASTA Medica AG), in 67 patients specifically selected based on their performance in previous IVF or ICSI treatments. At the start of the study the patients had been classified as either poor responders (N = 20; 25 cycles) or normal responders (N = 46; 52 cycles) based on the oocyte number (more or less than 3) in previous retrievals. There were several reasons for inclusion in the normal response group, such as a premature LH surge, and a poor embryo quality in agonist cycles. Several gonadotropins were used (hMG, uFSH and recFSH) and the daily dose (150 - 400 IU/day) depended on the patient’s previous performance. Cetrorelix (0.25 mg sc once daily) was started according to the size of the leading follicle instead of a fixed stimulation day. In most cycles the antagonist was started when the leading follicle had reached a mean diameter of 14 or 15 mm; this turned out to be on stimulation day 5 or 6. It was continued until the day of the hCG administration, when the largest follicle reached a size of 18 - 22 mm. Follicle aspiration was performed 34 to 35 hours after hCG administration. Two to five days later the embryo transfer was performed. Pregnancy and implantation rates as well as data from the offspring such as birth weight and congenital abnormalities were recorded. Results: In the group of poor responders only one cycle resulted in a pregnancy that ended in an early spontaneous abortion. It was clear that this group did not really benefit from the use of the antagonist. However the results in the normal response group were promising: 46 patients (15 primary, 31 secondary infertility: 30 IVF; 16 ICSI); 52 cycles (34 IVF; 18 ICSI); 23 clinical pregnancies (16 IVF; 7 ICSI), 20 ongoing pregnancies (14 IVF; 6 ICSI) 19 resulting in delivery (14 IVF; 5 ICSI) with the birth of in total 22 healthy children. No congenital abnormalities were detected. The table depicts results in the various categories. Ovum pick ups Transfers Pregnancies Preg rate per OPU Preg rate per ET Impl rate HMG 27 26 14 52 % 54 % 28 % UFSH 5 5 1 20 % 20 % 8% Rec FSH 20 20 8 40 % 40 % 16 % IVF 34 33 16 47 % 48 % 25 % ICSI 18 18 7 39 % 39 % 14 % Over-all 52 51 23 44 % 45 % 22 % In addition one IVF patient became pregnant after transfer of cryopreserved embryos. However this pregnancy ended in a missed abortion. Two patients showed an elevated LH (14.4 and 10.1 IU/l) on the day the GnRH antagonist administration was started (3.8% of all cycles) and two patients experienced a LH-elevation (11.9 and 11.6 IU/l) during the antagonist administration (3.8% of all cycles). In each of these groups one ongoing singleton pregnancy occurred. Three cases of a mild ovarian hyperstimulation syndrome occurred (no hospital admission necessary): one in a non- pregnant patient, two late hyperstimulations (7 tot 10 days after OPU) in relation to pregnancy. Two patients had a short lasting mild local reaction at the injection site of the cetrorelix. Conclusion: GnRH antagonists may yield excellent results as a second line approach in patients who have failed to achieve a pregnancy with a stimulation scheme without GnRH analogues or with GnRH agonists. However poor responders do not benefit from this new treatment strategy. There is a distinct subgroup of patients that may benefit from the use of GnRH antagonists in COH for IVF or ICSI.