Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
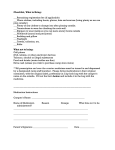
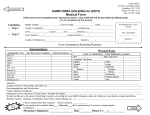
BEAVER CROSS CAMPS CAMPER MEDICAL FORM Beaver Cross Camps, 575 Burton Road, Greenwich NY 12834 phone: 518-692-9550 | fax 518-692-8777 | [email protected] Register online at www.beavercrossministries.org Camper Name__________________ _____________ Cabin/Group__________________ Session____________ This side to be completed by a parent or legal guardian, and returned prior to your child’s camp session. New forms are required yearly. Camper Name___________________________________ Date of Birth_____________ Age_____ Sex_____ Home Address_______________________________________________________________________________ Street City State Zip Mother's Name__________________________ Phone______________________ _______________________ First Number Second Number Father's Name___________________________ Phone______________________ _______________________ First Number Second Number Additional Emergency Contact__________________________________ Phone__________________________ Medical Insurance Carrier_____________________________ Card holder’s Name ________________________ Policy# _______________________________________________ Group # _____________________________ Permission for Camp Activities: Typical camp activities at include supervised hiking, swimming, boating, high ropes, climbing tower, sports, archery, crafts, music, worship and field trips. My signature below indicates my child has my permission to engage in all camp activities on and off camp grounds, and to be transported to, and participate in, outings and field trips off Christ the King/Beaver Cross grounds under the supervision of the Camp staff except at note below: ________________________________________________________________________ ________________________________________________________________________ Parental Concerns: List concerns you, as parents/guardians, believe the Camp Staff should be aware of including emotional or behavioral issues, eating disorders, bedwetting, nightmares, home sickness and the like. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ Authorization for Emergency Medical Treatment: I give the staff of Christ the King/Beaver Cross, a ministry of the Episcopal Diocese of Albany, permission to act for me on behalf of my child for treatment at a medical facility and to arrange necessary related transportation. In the event I cannot be reached in an emergency, I give permission to the attending physician to administer tests and treatment for my child. I understand that I am responsible for all health related costs incurred, and that I fully release Beaver Cross and the Episcopal Diocese of Albany from liability in connection with health related decisions made for your child on your behalf. I understand that all medications, including over-the-counter, must be kept in the Health Officer’s office with the exception of inhalers and epi-pens. Meningococcal Meningitis Response: This question is required by the NYS Department of Health for campers who will attending 7 or more consecutive nights at Camp. _____My child had the meningococcal meningitis immunization within the last ten years on _____________ _____I have read, or have had explained to me, the information regarding meningococcal meningitis disease. I understand the risks of not receiving the vaccine. I have decided that my child will not obtain immunization against meningococcal meningitis disease. Parent's Signature___________________________________________________ Date____________________ Updated 2-11-16 This side must be completed by a licensed Physician, Physician’s Assistant, or Nurse Practitioner within one year of the first camp session the camper is attending. Attach a copy of this child's immunization record. Individualized Health History and Physician’s orders for _________________________________ Camper name Health History Asthma/Breathing Difficulty Seizures Infectious Diseases Serious Injuries Heart Condition Surgery Diabetes Major Orthodontia Work Allergies Other Health Concerns? ________________ Date of Birth (Y) (N) Description Standard over-the counter medications are available in the Camp Infirmary, and will be distributed by the Camp RN if approval is indicated by the camper’s Physician. The dosage and schedule will be dispensed per label by weight and age unless otherwise noted by the camper’s Physician. Drug Name Acetaminophen (Tylenol) Ibuprofen (Advil) Benadryl Halls Cough Drops Regular Strength Tums Triple Antibiotic Ointment Hydrocortisone 1% Physician’s Order Yes No Yes No Yes No Yes No Yes No Yes No Yes No Dosage Schedule Comments Please list the prescription medications and parent-supplied non-prescription medications and vitamins the camper will bring to camp. All medications must be in original containers, and will be kept secured in the Camp Health Office. Drug Name Dosage Schedule Comments Please list any limitations or restrictions to camp activities for the camper. _____________________________________________________________________________ _____________________________________________________________________________ Physician’s Printed Name____________________________________________ Phone_________________________ Address___________________________________________________________________________________________ Physician’s Signature_______________________________________________ Examination Date_________________ Updated 2-11-16