Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
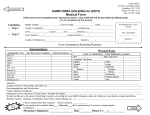
St. Luke Summer Day Camp – Registration 985-641-6429 Fax: 985-847-0742 Email: [email protected] (A $40.00 per family Non-Refundable registration fee must accompany each registration form) Parent’s Name:________________________ Mother’s Cell:_______________ Father’s Cell_______________ Address: _________________________ ________ City: _____________ Zip Code:__________ Parent’s (or guardian) place of employment: Mother_____________________ Phone:______________ Father _____________________ Phone:_______________ Campers must have written permission from a parent or guardian to leave camp with an individual other than the custodian. My child/children are under the custodial care of: ___Both parents ____Mother only _____ Father only _____ ____ Other (Please specify) __________________________ In Case of emergency, if parents cannot be reached, please contact: Name: ____________________________________ Relationship: ______________________ Work Phone: ___________________ Home or Cell Phone: _______________________ Camper Information: Family Doctor: ____________________________ Phone #: _________________ Have all of the children listed on this form had a tetanus shot in the last five years? ______ 1st Camper: _____________________ _________Age: ____ __ Date of Birth: ___/___/___ Sex: ______ # of Weeks Attending: 1st__ _ 2nd___ 3rd___ 4th ___ 5th ___ 6th___ 7th___ All 7 ___ Prohibited Activities? _____________________________ _______ School Attending:_____________________ Please list any allergies, disabilities, physical or emotional limitations your child’s counselor should know about: ___________________________________________________________________ Camper will bring medication to camp: Yes ___ No ___ Name of medication: ___________________ Camper May take Acetaminophen (Tylenol): Yes___No__ _Camper may take Pepto-Bismol: Yes __ No 2nd Camper: _____________________ _________Age: ____ __ Date of Birth: ___/___/___ Sex: ______ # of Weeks Attending: 1st__ _ 2nd___ 3rd___ 4th ___ 5th ___ 6th___ 7th___ All 7 ___ Prohibited Activities? _____________________________ _______ School Attending:_____________________ Please list any allergies, disabilities, physical or emotional limitations your child’s counselor should know about: ___________________________________________________________________ Camper will bring medication to camp: Yes ___ No ___ Name of medication: ___________________ Camper May take Acetaminophen (Tylenol): Yes___No__ _Camper may take Pepto-Bismol: Yes __ No _ 3rd Camper: _____________________ _________Age: ____ __ Date of Birth: ___/___/___ Sex: ______ # of Weeks Attending: 1st__ _ 2nd___ 3rd___ 4th ___ 5th ___ 6th___ 7th___ All 7 ___ Prohibited Activities? _____________________________ _______ School Attending:_____________________ Please list any allergies, disabilities, physical or emotional limitations your child’s counselor should know about: ___________________________________________________________________ Camper will bring medication to camp: Yes ___ No ___ Name of medication: ___________________ Camper May take Acetaminophen (Tylenol): Yes___No__ _Camper may take Pepto-Bismol: Yes __ No __ _