Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
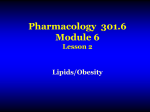
King Saud University 513 PHL College of Pharmacy ID# 430203801 Pharmacology Department Module # 6 Hyperlipidemia Prepared by: Hana M. Alharbi Year: 12-5- 1431 Hyperlipidemia is a major cause of atherosclerosis and atherosclerosis-associated conditions, such as coronary heart disease (CHD), ischemic cerebrovascular disease, and peripheral vascular disease. Dyslipidemias, including hyperlipidemia (hypercholesterolemia) and low levels of high-density-lipoprotein cholesterol (HDLC), are major causes of increased atherogenic risk; both genetic disorders and lifestyle (sedentary behavior and diets high in calories, saturated fat, and cholesterol) contribute to the dyslipidemias seen in developed countries around the world (Grundy et al., 2004). Clinical trial data support extending lipid-lowering therapy to high-risk patients whose major lipid risk factor is a reduced plasma level of HDL-C, even if their LDLC level does not meet the existing threshold values for initiating hypolipidemic drug therapy (The Expert Panel, 2002). In patients with low HDL-C and average LDL-C levels, appropriate drug therapy reduced CHD endpoint events by 20% to 35% (Heart Protection Study Collaborative Group, 2002; Downs et al., 1998; Rubins et al., 1999). Since two-thirds of patients with CHD in the United States have low HDL-C levels (<40 mg/dl), it is important to include low-HDL patients in management guidelines for dyslipidemia, even if their LDL-C levels are in the normal range (Grundy et al., 2004). Etiology Hyperlipidemia (elevated levels of triglycerides or cholesterol) and reduced HDL-C levels occur as a consequence of several interrelated factors that affect the concentrations of the various plasma lipoproteins. These factors may be lifestyle or behavioral (e.g., diet or exercise), genetic (e.g., mutations in a gene regulating lipoprotein levels), or metabolic (e.g., diabetes mellitus or other conditions that influence plasma lipoprotein metabolism) (Grundy et al., 2004). Risk factors Elevated LDL-C, reduced HDL-C, cigarette smoking, hypertension, type 2 diabetes mellitus, advancing age, and a family history of premature (men more than 55 years; women more than 65 years) CHD events in a first-degree relative. (Grundy et al., 2004). Pathophysiology of Hyperlipoproteinemia Normal Lipoprotein Metabolism Structure Lipoproteins have hydrophobic core regions containing cholesteryl esters and triglycerides surrounded by unesterified cholesterol, phospholipids, and apoproteins. Certain lipoproteins contain very high-molecular-weight B proteins that exist in two forms: B-48, formed in the intestine and found in chylomicrons and their remnants; and B-100, synthesized in liver and found in VLDL, VLDL remnants(IDL),LDL (formed from VLDL), and Lp(a) lipoproteins. HDL consist of at least 15 discrete molecular species. All species contain apolipoprotein A-I (apoA-I). Fifty-three other proteins are known to be distributed variously among the HDL species (Oliva et al., 2005). Synthesis & Catabolism Chylomicrons Chylomicrons are formed in the intestine and carry triglycerides of dietary origin, unesterified cholesterol, and cholesteryl esters. They transit the thoracic duct to the bloodstream. (Oliva et al., 2005). Triglycerides are removed in extrahepatic tissues through a pathway shared with VLDL that involves hydrolysis by the lipoprotein lipase (LPL) system. Decrease in particle diameter occurs as triglycerides are depleted. Surface lipids and small apoproteins are transferred to HDL. The resultant chylomicron remnants are taken up by receptor-mediated endocytosis into hepatocytes. (Oliva et al., 2005). Very-Low-Density Lipoproteins VLDL are secreted by liver and export triglycerides to peripheral tissues (Figure 35– 1). VLDL triglycerides are hydrolyzed by LPL, yielding free fatty acids for storage in adipose tissue and for oxidation in tissues such as cardiac and skeletal muscle. Depletion of triglycerides produces remnants (IDL), some of which undergo endocytosis directly by liver. The remainder is converted to LDL by further removal of triglycerides mediated by hepatic lipase. This process explains the "beta shift" phenomenon, the increase of LDL (beta-lipoprotein) in serum as hypertriglyceridemia subsides. Increased levels of LDL can also result from increased secretion of VLDL and from decreased LDL catabolism. (Oliva et al., 2005). Low-Density Lipoproteins LDL is catabolized chiefly in hepatocytes and other cells by receptor-mediated endocytosis. Cholesteryl esters from LDL are hydrolyzed, yielding free cholesterol for the synthesis of cell membranes. Cells also obtain cholesterol by synthesis via a pathway involving the formation of mevalonic acid by HMG-CoA reductase. Production of this enzyme and of LDL receptors is transcriptionally regulated by the content of cholesterol in the cell. Normally, about 70% of LDL is removed from plasma by hepatocytes. Even more cholesterol is delivered to the liver via IDL and chylomicrons. Unlike other cells, hepatocytes can eliminate cholesterol by secretion in bile and by conversion to bile acids. (Oliva et al., 2005). LP(a) Lipoprotein Lp(a) lipoprotein is formed from LDL and the (a) protein, linked by a disulfide bridge. The (a) protein is highly homologous with plasminogen but is not activated by tissue plasminogen activator. It occurs in a number of isoforms of different molecular weights. Levels of Lp(a) vary from nil to over 500 mg/dL and are determined chiefly by genetic factors. Lp(a) can be found in atherosclerotic plaques and may also contribute to coronary disease by inhibiting thrombolysis. Levels are elevated in certain inflammatory states. The risk of coronary disease is strongly related to the apo(a) genotype at a single polymorphic site in the coding region (SNP rs3798220). (Oliva et al., 2005). High-Density Lipoproteins The apoproteins of HDL are secreted by the liver and intestine. Much of the lipid comes from the surface monolayers of chylomicrons and VLDL during lipolysis. HDL also acquires cholesterol from peripheral tissues, protecting the cholesterol homeostasis of cells. Free cholesterol is transported from the cell membrane by a transporter, ABCA1, acquired by a small particle termed prebeta-1 HDL, and then esterified by lecithin:cholesterol acyltransferase (LCAT), leading to the formation of larger HDL species. Cholesterol is also exported from macrophages by the ABCG1 transporter to large HDL particles. The cholesteryl esters are transferred to VLDL, IDL, LDL, and chylomicron remnants with the aid of cholesteryl ester transfer protein (CETP). Much of the cholesteryl ester thus transferred is ultimately delivered to the liver by endocytosis of the acceptor lipoproteins. HDL can also deliver cholesteryl esters directly to the liver via a docking receptor (scavenger receptor, SR-BI) that does not cause endocytosis of the lipoproteins. (Oliva et al., 2005). Figure-1: Metabolism of lipoproteins of hepatic origin. The heavy arrows show the primary pathways. Nascent VLDL are secreted via the Golgi apparatus. They acquire additional apoC lipoproteins and apolipoprotein E (apoE) from HDL. Very-low-density lipoproteins (VLDL) are converted to VLDL remnants (IDL) by lipolysis via lipoprotein lipase in the vessels of peripheral tissues. In the process, C apolipoproteins and a portion of the apoE are given back to high-density lipoproteins (HDL). Some of the VLDL remnants are converted to LDL by further loss of triglycerides and loss of apoE. A major pathway for LDL degradation involves the endocytosis of LDL by LDL receptors in the liver and the peripheral tissues, for which apo B-100 is the ligand. Dark color denotes cholesteryl esters; light color denotes triglycerides; the asterisk denotes a functional ligand for LDL receptors; triangles indicate apoE; circles and squares represent C apolipoproteins. FFA, free fatty acid; RER, rough endoplasmic reticulum. (Oliva et al., 2005). Diagnosis Patients must fast for at least 12 hours before blood sampling, because chylomicron clearance can take up to 10 hours. However, a fasted sample is not required for simple cholesterol screening. Laboratory testing of the lipid profile measures total plasma cholesterol, HDL, triglycerides, VLDL levels and LDL levels. (Oliva et al., 2005). DRUG THERAPY OF DYSLIPIDEMIA Statins The statins are the most effective and best-tolerated agents for treating dyslipidemia. These drugs are competitive inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase, which catalyzes an early, rate-limiting step in cholesterol biosynthesis. Higher doses of the more potent statins (e.g., atorvastatin and simvastatin) also can reduce triglyceride levels caused by elevated VLDL levels. Some statins also are indicated for raising HDL-C levels, although the clinical significance of these effects on HDL-C remains to be proven. (Law et al., 2003) Mechanism of Action Statins exert their major effect reduction of LDL levels through a mevalonic acid-like moiety that competitively inhibits HMG-CoA reductase. By reducing the conversion of HMG-CoA to mevalonate, statins inhibit an early and rate-limiting step in cholesterol biosynthesis. (Law et al., 2003) Statins affect blood cholesterol levels by inhibiting hepatic cholesterol synthesis, which results in increased expression of the LDL receptor gene. In response to the reduced free cholesterol content within hepatocytes, membrane-bound SREBPs are cleaved by a protease and translocated to the nucleus. The transcription factors then bind the sterol-responsive element of the LDL receptor gene, enhancing transcription and increasing the synthesis of LDL receptors (Horton et al., 2002). Degradation of LDL receptors also is reduced. The greater number of LDL receptors on the surface of hepatocytes results in increased removal of LDL from the blood, thereby lowering LDL-C levels. (Law et al., 2003) Triglyceride Reduction by Statins Triglyceride levels more than 250 mg/dl are reduced substantially by statins, and the percent reduction achieved is similar to the percent reduction in LDL-C (Stein et al., 1998). Accordingly, hypertriglyceridemic patients taking the highest doses of the most potent statins (simvastatin and atorvastatin, 80 mg/day; rosuvastatin, 40 mg/day) experience a 35% to 45% reduction in LDL-C and a similar reduction in fasting triglyceride levels (Ose et al., 2000; Hunninghake et al., 2004). Effect of Statins on HDL-C Levels Most studies of patients treated with statins have systematically excluded patients with low HDL-C levels. (Hunninghake et al., 2004). Effects of Statins on LDL-C Levels Statins lower LDL-C by 20% to 55%, depending on the dose and statin used (Jones et al., 2003). Adverse Effects and Drug Interactions Hepatotoxicity Initial postmarketing surveillance studies of the statins revealed an elevation in hepatic transaminase to values greater than three times the upper limit of normal, with an incidence as great as 1%. (Law et al., 2003) Myopathy The myopathy syndrome is characterized by intense myalgia similar to flu-related myalgia, first in the arms and thighs and then in the entire body, along with weakness and fatigue. Symptoms progress as long as the patient continues to take the statin. Myoglobinuria, renal failure, and death have been reported (Staffa et al., 2002). Statins in Combination with Other Lipid-Lowering Drugs Statins, in combination with the bile acid-binding resins cholestyramine and colestipol, produce 20% to 30% greater reductions in LDL-C than can be achieved with statins alone (Staffa et al., 2002). Bile-Acid Sequestrants The two established bile-acid sequestrants or resins (cholestyramine and colestipol) are among the oldest of the hypolipidemic drugs, and they are probably the safest, since they are not absorbed from the intestine. Colesevelam is a newer bile-acid sequestrant that is prepared as an anhydrous gel and taken as a tablet. Mechanism of Action The bile-acid sequestrants are highly positively charged and bind negatively charged bile acids. Because of their large size, the resins are not absorbed, and the bound bile acids are excreted in the stool. Effects on Lipoprotein Levels The reduction in LDL-C by resins is dose-dependent. Doses of 8 to 12 g of cholestyramine or 10 to 15 g of colestipol are associated with 12% to 18% reductions in LDL-C. In patients with normal triglyceride levels, triglycerides may increase transiently and then return to baseline. HDL-C levels increase 4% to 5%. Statins plus resins or niacin plus resins can reduce LDL-C by as much as 40% to 60%. Colesevelam, in doses of 3 to 3.75 g, reduces LDL-C levels by 9% to 19%. Adverse Effects and Drug Interactions The resins are generally safe, as they are not systemically absorbed. Since they are administered as chloride salts, rare instances of hyperchloremic acidosis have been reported. Severe hypertriglyceridemia is a contraindication to the use of cholestyramine and colestipol since these resins increase triglyceride levels. Patients taking cholestyramine and colestipol complain of bloating and dyspepsia. Cholestyramine and colestipol bind and interfere with the absorption of many drugs, including some thiazides, furosemide, propranolol, l-thyroxine, digoxin, warfarin, and some of the statins. Niacin (Nicotinic Acid) Niacin, nicotinic acid (pyridine-3-carboxylic acid), one of the oldest drugs used to treat dyslipidemia, favorably affects virtually all lipid parameters. (Karpe and Frayn, 2004). Niacin is a water-soluble B-complex vitamin that functions as a vitamin only after its conversion to NAD or NADP, in which it occurs as an amide (Shlipak et al., 2000). Mechanism of Action In adipose tissue, niacin inhibits the lipolysis of triglycerides by hormone-sensitive lipase, which reduces transport of free fatty acids to the liver and decreases hepatic triglyceride synthesis. Niacin and related compounds (e.g., 5-methylpyrazine-2carboxylic-4-oxide, acipimox) may exert their effects on lipolysis by inhibiting adipocyte adenylyl cyclase (Karpe and Frayn, 2004). In the liver, niacin reduces triglyceride synthesis by inhibiting both the synthesis and esterification of fatty acids, effects that increase apoB degradation (Karpe and Frayn, 2004). Effects on Plasma Lipoprotein Levels Reductions of 25% in LDL-C levels are possible with doses of 4.5 to 6 g per day, but 3 to 6 weeks are required for maximal effect. HDL-C increases less in patients with low HDL-C levels (<35 mg/dl) than in those with higher levels (Sprecher, 2000). Adverse Effects Two of niacin's side effects, flushing and dyspepsia. The cutaneous effects include flushing and pruritus of the face and upper trunk, skin rashes, and acanthosis nigricans. (Karpe and Frayn, 2004). The most common, medically serious side effects are hepatotoxicity, manifested as elevated serum transaminases and hyperglycemia (Karpe and Frayn, 2004). In patients with diabetes mellitus, niacin should be used cautiously, since niacininduced insulin resistance can cause severe hyperglycemia. Niacin also elevates uric acid levels and may reactivate gout. (Karpe and Frayn, 2004). Fibric Acid Derivatives: PPAR Activators Clofibrate as well as two other fibrates, gemfibrozil and fenofibrate. Mechanism of Action The mechanisms by which fibrates lower lipoprotein levels, or raise HDL levels, remain unclear. Recent studies suggest that many of the effects of these compounds on blood lipids are mediated by their interaction with peroxisome proliferator activated receptors (PPARs) (Kersten et al., 2000), which regulate gene transcription. Three PPAR isotypes (α, β, and γ) have been identified. Fibrates bind to PPARα, which is expressed primarily in the liver and brown adipose tissue and to a lesser extent in kidney, heart, and skeletal muscle. Fibrates reduce triglycerides through PPAR α -mediated stimulation of fatty acid oxidation, increased LPL synthesis, and reduced expression of apoC-III (Vakkilainen et al., 2003). Effects on Lipoprotein Levels Fibrate treatment decreases triglyceride levels by up to 50% and increases HDL-C concentrations about 15%; LDL-C levels may be unchanged or increase. The secondgeneration agents, such as fenofibrate, bezafibrate, and ciprofibrate, lower VLDL levels to a degree similar to that produced by gemfibrozil, but they also are more likely to decrease LDL levels by 15% to 20%. (Vakkilainen et al., 2003). Adverse Effects and Drug Interactions Gastrointestinal side effects occur in up to 5% of patients. Other side effects are reported infrequently and include rash, urticaria, hair loss, myalgias, fatigue, headache, impotence, and anemia. (Vakkilainen et al., 2003). Renal failure is a relative contraindication to the use of fibric acid agents, as is hepatic dysfunction. Combined statin-fibrate therapy should be avoided in patients with compromised renal function. (Vakkilainen et al., 2003). Ezetimibe and the Inhibition of Dietary Cholesterol Uptake Ezetimibe is the first compound approved for lowering total and LDL-C levels that inhibits cholesterol absorption by enterocytes in the small intestine (van Heek et al., 2000). It lowers LDL-C levels by about 18% and is used primarily as adjunctive therapy with statins. (Vakkilainen et al., 2003). Mechanism of Action Recent data indicate that ezetimibe inhibits a specific transport process in jejunal enterocytes, which take up cholesterol from the lumen. The putative transport protein is NPC1L1 (Altmann et al., 2004; Davis et al., 2004). Ezetimibe does not affect intestinal triglyceride absorption. In human subjects, ezetimibe reduced cholesterol absorption by 54%, precipitating a compensatory increase in cholesterol synthesis, which can be inhibited with a cholesterol synthesis inhibitor such as a statin (Sudhop et al., 2002). Adverse Effects and Drug Interactions Other than rare allergic reactions, specific adverse effects have not been observed in patients taking ezetimibe. Since all statins are contraindicated in pregnant and nursing women, combination products containing ezetimibe and a statin should not be used by women in childbearing years in the absence of contraception. (Sudhop et al., 2002) References 1- Grundy, S.M., Hansen, B., Smith, S.C., Jr., Cleeman, J.I., and Kahn, R.A. Clinical management of metabolic syndrome: report of the American Heart Association/National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Circulation, 2004c, 109:551-556. 2- Oliva, C.P., Pisciotta, L., Volti, G.I. Inherited apoprotein A-V deficiency in severe hypertriglyceridemia. Arterioscler. Thromb. Vasc. Biol., 2005, in press. 3- Law, M.R., Wald, N.J., and Rudnicka, A.R. Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: Systematic review and meta-analysis. BMJ, 2003, 326:1423. PUBMED 4- Horton, J.D., Goldstein, J.L., and Brown, M.S. SREBPs: Activators of the complete program of cholesterol and fatty acid synthesis in the liver. J. Clin. Invest., 2002, 109:1125-1131. PUBMED 5- Hunninghake, D.B., Stein, E.A., Bays, H.E. Rosuvastatin improves the atherogenic and atheroprotective lipid profiles in patients with hypertriglyceridemia. Coron. Artery Dis., 2004, 15:115-123. PUBMED 6- Ose, L., Davidson, M.H., Stein, E.A. Lipid-altering efficacy and safety of simvastatin 80 mg/day: Long-term experience in a large group of patients with hypercholesterolemia. World Wide Expanded Dose Simvastatin Study Group. Clin. Cardiol., 2000, 23:39-46. PUBMED 7- Jones, P.H., Davidson, M.H., Stein, E.A. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR trial). Am. J. Cardiol., 2003, 92:152-160. PUBMED 8- Staffa, J.A., Chang, J., and Green, L. Cerivastatin and reports of fatal rhabdomyolysis. N. Engl. J. Med., 2002, 346:539-540. PUBMED 9- Karpe, F., and Frayn, K.N. The nicotinic acid receptor¾a new mechanism for an old drug. Lancet, 2004, 363:1892-1894. PUBMED 10- Shlipak, M.G., Simon, J.A., Vittinghoff, E. Estrogen and progestin, lipoprotein(a), and the risk of recurrent coronary heart disease events after menopause. JAMA, 2000, 283:1845-1852. PUBMED 11- Sprecher, D.L. Raising high-density lipoprotein cholesterol with niacin and fibrates: a comparative review. Am. J. Cardiol., 2000, 86(suppl):46L-50L. 12- Vakkilainen, J., Steiner, G., Ansquer, J.C. Relationships between low-density lipoprotein particle size, plasma lipoproteins, and progression of coronary artery disease: the Diabetes Atherosclerosis Intervention Study (DAIS). Circulation, 2003, 107:1733-1737. PUBMED 13- Altmann, S.W., Davis, H.R., Jr., Zhu, L.J. Niemann-Pick C1 like 1 protein is critical for intestinal cholesterol absorption. Science, 2004, 303:1201-1204. PUBMED 14- Davis, H.R., Jr., Zhu, L.J., Hoos, L.M. Niemann-Pick C1 Like 1 (NPC1L1) is the intestinal phytosterol and cholesterol transporter and a key modulator of whole-body cholesterol homeostasis. J. Biol. Chem., 2004, 279:33586-33592. PUBMED 15- van Heek, M., Farley, C., Compton, D.S. Comparison of the activity and disposition of the novel cholesterol absorption inhibitor, SCH58235, and its glucuronide, SCH60663. Br. J. Pharmacol., 2000, 129:1748-1754. 16- Sprecher, D.L. Raising high-density lipoprotein cholesterol with niacin and fibrates: a comparative review. Am. J. Cardiol., 2000, 86(suppl):46L-50L. 17- Sudhop, T., Lutjohann, D., Kodal, A., et al. Inhibition of intestinal cholesterol absorption by ezetimibe in humans. Circulation, 2002, 106:1943-1948. PUBMED