Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
ICANCER RESEARCH 49, 1621-1639, April 1, 1989]
Perspectives in Cancer Research
Biological Response Modifiers: The New Immunotherapy
Kenneth A. Foon1
Division of Clinical Immunology, Roswell Park Memorial Institute, and Department of Medicine, Stale University of New York at Buffalo, Buffalo, New York 14263
Immunotherapy is divided into two overlapping categories,
active and passive. The goal of active immunotherapy is the
stimulation of host ant ¡tumorimmunity, either cellular or hu
moral. This can be accomplished in a direct or specific fashion
by using tumor vaccines to generate an immune response to
tumor-associated antigens. Nonspecific antitumor immunity
can be propagated by compounds such as BCG.2 Passive im
munotherapy relies on the administration of biologically active
agents with innate antitumor properties, such as antibodies
reactive with growth factor receptors. In most instances, host
immunity is an important cofactor in active immunotherapy.
In addition, some agents, such as antibodies, can exert antitumor effects via active or passive mechanisms. The complex
immune circuits that are set into motion by these therapies
account for the imperfect, but nonetheless useful division into
active and passive types.
Immunotherapy is very effective in certain animal model
systems and it has been used to treat human cancers for several
decades (1). In the 1960s and 1970s trials of nonspecific immunostimulants including BCG or specific allogeneic or autologous vaccines were evaluated with early promising reports
(2-5). Unfortunately, none of these approaches has been shown
to be effective in controlled trials (6, 7).
During the past decade, renewed interest in immunotherapy
has been stimulated by genetic engineering and mass cell culture
and improved techniques in protein and nucleic acid sequenc
ing. These have made available highly purified molecules in
cluding interferons, interleukins, tumor necrosis factor, and
hematopoietic growth factors. Also, hybridoma technology (8)
has generated murine monoclonal antibodies directed against
tumor-associated antigens. The term "biological response mod
ifiers" (9) is often used to refer to these newer approaches to
to B-cell mitogens, viruses, foreign cells, or tumor cells, ßInterferon is produced by fibroblasts following exposure to
viruses or foreign nucleic acids. 7-Interferon is produced by Tlymphocytes following stimulation of T-cell mitogens, specific
antigens, or IL-2 (13). Complete nucleotide sequences for the
a-, ß-,and 7-interferon genes are known, and amino acid
sequences have been deduced (14-16). Sixteen distinct a-interferon genes are described; each encodes a protein of approxi
mately 166 amino acids (14). Only a single 0-interferon gene
has been identified encoding a protein of 166 amino acids;
similarly there appears to be a single 7-interferon gene encoding
a protein of 144 amino acids (15-17).
The a-interferon first used in clinical trials was obtained from
Sendai virus-stimulated buffy coat leukocytes. Its purity was
about 1% (IO6 units/mg protein; 1 unit of interferon is approx
imately the amount that reduces viral replication in cell culture
by one-half) (18). Use of high performance liquid chromatography, two dimensional polyacrylamide gel electrophoresis, and
immune affinity chromatography has resulted in the purifica
tion of a-interferon to homogeneity (IO8 units/mg protein) (19,
20). Use of recombinant DNA technology can produce large
quantities of pure a-interferon (21).
Large scale production of ßand 7-interferons is more recent
and clinical trials are limited. a-Interferon has been extensively
studied for the past decade in both basic science and clinical
research and is among the most potent biological agents ever
administered to humans. Although antitumor activity is de
tected in some solid malignancies in vitro and in vivo (22-24),
the most impressive responses are in hematological malignan
cies (12).
The mechanisms of interferon-mediated antitumor effects in
murine models and humans are unclear. Putative mechanisms
immunotherapy.
include a direct antiproliferative effect on the tumor, induction
or augmentation of a host effector mechanism, such as NK and
Interferons
monocyte cytotoxicity, and induction or augmentation of
expression of membrane antigens on tumor cells which facilitate
Interferon was initially identified as a soluble factor able to
subsequent immune recognition by the host.
inhibit infection of chick chorioallantoic membranes by influ
ii Interferon has moderate activity in a limited number of
enza A virus (10). Subsequent studies have shown the interfer
solid tumors (Table 2). It is active in bladder cancer when
ons to be a family of closely related proteins and glycoproteins.
instilled directly at very high doses (57-59). It is also active in
In addition to their antiviral activity these molecules are potent
acquired immunodeficiency syndrome-related Kaposi sarcoma
regulators of cell gene expression, structure, and function. They
(45-47), renal cell carcinoma (40-44), malignant melanoma
also exhibit direct antiproliferative activity. These properties
(27-32), and carcinoid tumors (90). There is little evidence of
underlie the current interest in interferon as an anticancer agent.
Three major species of human interferon are identified: a, ß, activity in the common cancers such as breast and colon cancer
and 7(11) (Table 1). a-Interferon is produced by leukocytes (B- and only limited activity for squamous cell tumors of the head
and neck and lung (33-39, 48-52, 48, 53, 54, 60, 61). Clearly,
cells, T-cells, null cells, and macrophages) following exposure
a-interferon as a single agent will not have a major impact in
Received 7/15/88; revised 10/11/88; accepted 1/6/89.
the therapy of solid tumors. Current directions of interferon
' To whom requests for reprints should be addressed, at Division of Clinical
research include combinations with other biologicals and in
Immunology, Roswell Park Memorial Institute, Elm and Carlton Sis.. Buffalo,
NY 14263.
some cases cytotoxic drugs.
2The abbreviations used are: BCG, Bacillus Calmette-Guérin;IL-1, IL-2, ILa-Interferon has had its greatest impact in the treatment of
3, interleukins 1, 2, and 3, respectively; NK natural killer; (MI,, chronic myelogenous leukemia; LAK, lymphokine-activated killer; TNF, tumor necrosis factor;
certain hematological malignancies. Approximately 90% of
i.a., intraarterially; TIL, tumor-infiltrating lymphocytes; CPU, colony-forming
patients with hairy cell leukemia respond to a-interferon (64unit; GM-CSF, granulocyte-macrophage-colony-stimulating
factor; G-CSF, gran71) with a normalization of blood counts. Improvement in
ulocyte-colony-stimulating factor, M-CSF, macrophage-colony-stimulating fac
tor; ALL, acute lymphoblastic leukemia.
natural killer cell activity and immunological surface marker
1621
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
Table l Interferons in clinical use"
Subtype*
(new
nomenclature)
Leukocyte (IFN-a[LE])c
Type
Purity
Amino acid
differences
Source
<r
Leukocytes from
normal blood
Lymphoblastoid
(Namalwa) cells
in culture
Transformed Escherichia coli
Lymphoblastoid (IFN-alfaNl), Wellferon* (Bur
roughs Wellcome Co.)
Recombinant a.1 (IFN-alfa2b), Intron A* (Schering
Corp.)
Recombinant «A(IFN-alfa2a), Roferon-A®(Hoff
mann-La Roche, Inc.)
Recombinant <>D(IFN-aD)
Recombinant a2arg (II Nalfa-2c)
Fibroblast (IFN-/3)
Recombinant 0cys (rlFN0cys)
Recombinant /3ser (rlFNImmune (IFN-f)
>95
Transformed E. coli
>95
Transformed E. coli
Transformed E. coli
>95
>95
Fetal foreskin fibroblast in culture
Transformed E. coli
>95
Transformed E. coli
>95
T-lymphocytes
from normal
blood
Transformed E. coli
>95
Recombinant y (rIFN-y)
" Reproduced with permission from Ref. 12.
* New nomenclature was proposed at a joint meeting of the WHO and USAN council in May 198S.
c IFN, interferon; rIFN, recombinant IFN.
d These crude preparations can be purified to near homogeneity (see text).
Arginine at position
23; deletion at posi
tion 44 when com
pared to other a sub
types.
Lysine at position 23;
deletion at position
44.
29 variations from aA
Arginine at position
23.
Arginine at position
34.
Cysteine at position
17.
Serine at position 17.
Table 2 Clinical trials with a-interferon
Tumor
Solid malignancies
Osteogenic sarcoma
Melanoma
Breast cancer
Renal cell
Kaposi's sarcoma (AIDS-related)
Coloréela!carcinoma
Carcinoid
Lung
Small cell
Non-small cell
Ovarian cancer
Bladder cancer (papillomatosis or superficial)
Head and neck (squamous)
Nasopharyngeal
Cervical cancer
No. of
évaluable
patients
Response rates
CR"
15
185
187
252
120
65
9
0
7
0
6
14
0
0
10
70
42
55
0
0
5
20
4
0
3
11
13
14
PR
MR
1
14
14
37
22
2
6
0
1
3
16
6
2
3
2
10
28
%of
total
response
7
11
7
17
36
3
67
0
1
19
65
91
15
43
Ref.
25,26
27-32
33-39
40-44
45-47
48-52
90
53
48,54
55,56
57-59
60,61
62
63
Hematological malignancies
Hairy cell leukemia*
64-71
158
44
22
96
Non-Hodgkin's lymphoma
74-77
107
6
Low grade
12
37
46
74,75
Intermediate and high grade
1
8
15
61
2
Hodgkin's disease
19
0
2
75,76
21
4
78-80
Cutaneous T-cell lymphoma
14
50
42
8
3
76,77,81,82,91
Chronic lymphocytic leukemia
73
0
12
16
41'
85-87
17
Multiple myeloma
224
3
Chronic myelogenous leukemia
81
88
68
46
8
" CR, complete response (absence of disease); PR, partial response (>50% decrease in disease); MR, minor response (less than a partial response); % of total
response, CR + PR/number of évaluablepatients; AIDS, acquired immunodeficiency syndrome.
* Complete response means absence of hairy cells in the bone marrow and normalization of peripheral blood leukocytes, platelets, and erythrocytes. Partial response
means a normalization of peripheral blood leukocytes, platelets, and erythrocyte counts and a >50% reduction in hairy cells in the bone marrow. Minor response
generally means improvement in hemoglobin to more than 10 g/dl or improvement in platelets to more than 100 x I(("/liter or improvement in neutrophils to more
than 1 x 1(("/liter. Percentage of total response for hairy cell leukemia includes minor responses.
'"Complete response and partial response not available from all trials; percentage of total response includes all responses.
expression parallels immune recovery (68). Complete responses is achieved. Most patients relapse over a period of 6 months to
are rare with a-interferon and there are no cures. However, 2 years (71) but respond to additional treatment with interferon.
patients have durable responses. Side effects are few because Pentostatin is also very effective therapy in hairy cell leukemia
only low doses of interferon are required for response, a- and is an alternative in patients who fail to respond or become
Interferon can be discontinued in most patients after a response resistant to a-interferon (72). Studies to assess the standard
1622
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
low dose of a-interferon (3-4 x IO6 units 3 times/week) with a
lower dose (0.3-0.4 x 106 units 3 times/week) are under way.
Preliminary results suggest efficacy for the lower dose (73).
Although a-interferon should not necessarily replace splenectomy as primary therapy for hairy cell leukemia, it is useful in
patients who are not surgical candidates or who have failed
splenectomy.
o-Interferon is active in several other hematological malig
nancies. Approximately 50% of patients with low grade nonHodgkin's lymphoma or cutaneous T-cell lymphoma respond
to a-interferon (74-80). Although it is not active in advanced
chronic lymphocytic leukemia (76, 77, 81, 82, 91), results in
previously untreated patients are more encouraging (83, 84).
Modest activity is reported in patients with multiple myeloma
(85-87). Over 80% of patients with chronic myelogous leuke
mia in the chronic phase respond to a-interferon with excellent
control of blood counts (88). In a small fraction of these patients
the percentage of cells with the Philadelphia chromosome de
creases or disappears, albeit transiently (88). Studies are under
way to demonstrate whether a-interferon prolongs the duration
of chronic phase and/or survival in CML. 7-Interferon also has
activity in CML (92); trials of a- and 7-interferon in CML are
in progress.
Recombinant 0-interferon recently entered clinical trials. Its
activity seems similar to a-interferon (24). In contrast, 7-inter
feron has demonstrated limited antitumor activity (93-95) with
the possible exception of CML (92). However, 7-interferon
enhances immune responses at low doses (96).
Interleukin 2
IL-2 is a Mr 15,000 glycoprotein of 133 amino acids. IL-2 is
released following antigen recognition and presentation to I
cells, and causes T-cell proliferation. It was originally referred
to as T-cell growth factor. IL-2 is currently available as a
recombinant molecule and has been used in many clinical trials.
IL-2 causes lymphoid proliferation both in vitro and in vivo
(97). It activates the lytic mechanisms of LAK cells for fresh
tumors and appears to activate cytolytic T-cells (98-100). It
enhances the effect of transferred LAK cells and cytolytic Tcells (101, 102). IL-2 affects the vascular endothelium and
causes emigration of lymphoid cells from the blood into tissues
(103, 104). IL-2 causes the release of other lymphokines in
cluding 7-interferon and TNF which likely mediate additional
effects (97, 105).
IL-2 is active during the early stages of tumor growth (day 3)
in both immunogenic and nonimmunogenic murine tumors
(106-108). IL-2 is active in the advanced stages of tumor growth
(day 10) but only in animals with weakly immunogenic tumors.
The antitumor effect in nonimmunogenic tumors is mediated
primarily by LAK cells and in weakly immunogenic tumors by
T-cells as well as LAK cells (109).
Infusion of IL-2 in humans is associated with increases in
mature T-cells (97). It also induces expression of IL-2 receptors
on both T-cells and monocytes and enhances tumor cell lysis
by immune effector cells (110).
IL-2 as a single agent is active in renal cell cancer, melanoma,
and non-Hodgkin's lymphoma (111). Studies are under way in
other tumor types. The toxicity of IL-2 administered systemically is substantial and includes fever, chills, nausea, vomiting,
diarrhea, hypotension, cutaneous erythema, fluid retention, eosinophilia, anemia, and moderate to severe hepatic and renal
dysfunction (111). A limited number of patients develop neu
ropsychiatrie complications heralded by confusion. This may
last days to weeks. Most other IL-2 toxicities resolve within
hours to days following discontinuation of IL-2. IL-2-activated
lymphocytes adhere to endothelial cells in a dose-dependent
manner. These cells are cytotoxic in vitro to endothelial cells
which may explain some of the systemic toxicity (112). In
creased expression of HLA-DR antigens occurs in tumor, endo
thelial cells, and in perivascular T-cells in patients receiving IL2 (104). Preliminary data suggest that this may be greater in
patients whose lesions respond to IL-2 treatment (109). The
mechanisms by which IL-2 mediates antitumor effects are not
known but histológica! examination of tumors before and after
treatment shows infiltration with large activated T-cells con
sistent with a cell-mediated immune response (113).
IL-2 is known to stimulate all subsets of T-cells. A strategy
was designed to decrease T-suppressor cells by injecting lowdose cyclophosphamide prior to IL-2 administration (114). Six
of 24 patients with melanoma responded and all responding
patients had LAK cell activation in vivo. Other strategies to
improve IL-2 activity include combinations with interferons,
tumor necrosis factor, or monoclonal antibodies. One prelimi
nary study reported 6 of 21 (29%) persons with advanced renal
cell carcinoma responding to the combination of IL-2 and ßinterferon (115).
Tumor Necrosis Factor
TNF was first identified in mice primed with BCG and
challenged with endotoxin. Serum from these mice caused
tumor necrosis when transferred into tumor-bearing animals
(116). This factor is produced by monocytes and is called TNFa. Recent data indicate that cachectin, responsible for wasting
in chronic parasitic diseases, is identical to TNF-a (117). A
related cytotoxic protein, called lymphotoxin or TNF-/3, is
produced by lymphocytes (118, 119). The genes for encoding
both TNF-a and TNF-/ÃŽhave been molecularly cloned and
sequenced (120-124). Both molecules have cytostatic and cy
totoxic effects in vitro against a variety of human tumors (125127). Antitumor effects have been demonstrated in syngeneic
murine tumor models and a human tumor xenograft model in
nude mice (128). Tumor necrosis factor has recently been
studied in Phase I trials (129-132). Toxicity was over a broad
range of doses; antitumor activity was minimal. Some serious
toxicities such as hypertension are not dose related. Some
investigators have found synergistic antitumor activities in vitro
and in vivo when TNF is combined with interferon or cyclo
phosphamide (133-136). TNF is currently being studied with
other biologicals.
Adoptive Cellular Therapy
A variety of immune cells have antitumor activity including
T-cells, NK cells, killer cells, monocytes/macrophages,
and
polymorphonuclear leukocytes. B-cells mediate their antitumor
effect by producing antibodies that combine with killer cells,
monocytes, or polymorphonuclear cells and mediate antibodydependent cellular cytotoxicity. Monocytes make TNF and
peroxides which are toxic to tumor cells. Polymorphonuclear
cells also generate peroxides and contain enzymes that are toxic
to tumor cells. NK cells, killer cells, and cytotoxic T-cells all
make lymphokines, such as natural killer cytotoxic factor, that
kill or inhibit the growth of tumor cells.
The different cells that kill tumor cells recognize their targets
in distinct ways. Cytotoxic T-cells recognize the tumor-associ
ated antigen together with self-antigens. Killer cells, monocytes,
1623
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
and polymorphonuclear cells mediate antibody-dependent cel
lular toxicity by binding of their Fc receptor to the Fc portion
of the antibody attached to the target tumor cell.
The most extensively studied adoptive cellular therapy is the
LAK cell described by Grimm et al. (137). They demonstrated
that incubation of normal mouse splenocytes or human periph
eral mononuclear cells with IL-2 in vitro for 3-5 days resulted
in generation of cells capable of lysing a spectrum of fresh and
cultured tumor cells in vitro. LAK cells are distinguished from
NK cells because of their IL-2 dependence. LAK cells are nonmajor histocompatibility complex restricted, and lack mature
T-cell markers (CD3) although they have other T-cell markers
such as CD2. They also express the Fc and C3bi receptors (138).
No efficacy or major toxicity was seen in cancer patients treated
with LAK cells alone. Later studies demonstrated that lympho
cytes obtained by repetitive leukapheresis, cultured with IL-2
for 3-4 days, and reinfused with IL-2 resulted in both partial
and complete responses in patients with disseminated solid
tumors (101). Several investigators have reported responses in
patients with melanoma, renal cell carcinoma, colorectal car
cinoma, and non-Hodgkin's lymphoma treated with IL-2 and
LAK cells (111, 139-145) (Table 3).
There are critical questions regarding the mechanism by
which IL-2 in combination with LAK cells mediates their
antitumor effect. In addition, the relative roles of IL-2 and LAK
cells remain to be clarified. It has not been demonstrated that
the LAK cells themselves actually infiltrate the tumor or
whether they are necessary in addition to the IL-2. Current
trials are addressing these issues. Most of the toxicity associated
with this therapy is thought to be related to increase in capillary
permeability directly or indirectly related to IL-2. Recent stud
ies using lower doses of IL-2 given by continuous infusion (36 milliunits/m2 daily) in combination with LAK cells have
reported efficacy (139). Toxicity is decreased with minimal fluid
retention; few patients required intensive care. The in vivo
generation of LAK cells appears to be greater following contin
uous infusion compared to bolus therapy (146). Trials are under
way to determine the efficacy of low dose continuous infusional
therapy. Other approaches to LAK cell therapy with IL-2
include La., i.p., and intrapleural infusions (147-151); clinical
responses have been observed. However, i.p. fibrosis has been
a problem following i.p. therapy (147). Other strategies to
improve LAK therapy include in vitro incubation with IL-4 in
addition to IL-2 which may synergize the generation of LAK
cells (152) (Table 4).
Another approach to adoptive immunotherapy is to expand
tumor-specific T-lymphocytes that have infiltrated the tumor
with IL-2 in vitro. These cells are referred to as tumor-infiltrat
ing lymphocytes and are reported to be 50 to 100 times more
effective than LAK cells in lysis of autologous tumor cells from
tumor-bearing mice (102). IL-2-activated TIL have been iso
lated from human melanoma, renal and head and neck tumors
Table 3 Clinical responses to interleukin 2 with and without lymphokineactivated killer cells
IL-2 + LAK
Total
évaluable CR PR
%
Refs.
139-143111,
cancerMelanomaColorectal
Renal cell
141,143,
139,
144111,
cancerLungNon-Hodgkin's
139111,
139111,
lymphomaHodgkin's
141138,
139,
diseaseGlioblastoma
141145
multiforme"13183261044692111003216212303122121050750111,
°Injected through an Ommaya reservoir.
Table 4 How can we improve 1L-2/LAK therapy?
Optimize dose of IL-2.
Optimal method of delivery (continuous r.v.bolus).
Enhance activation of LAK (i.e., IL-4).
Regional therapy (i.e., i.p., i.a.).
Combination therapy with chemotherapy agents (i.e., cyclophosphamide).
Combinations with other biologicals (i.e.. a-interferon, monoclonal antibodies).
Improved killer cells (i.e., tumor-infiltrating lymphocytes).
(153-156). TIL may expand better and have higher antitumor
cytotoxicity than LAK cells and may be a potentially better
adoptive immunotherapy modality. TIL appear to be hetero
geneous and have demonstrated both major histocompatibilityrestricted (156) and nonrestricted activity (154,155). TIL dem
onstrated strong cytotoxicity when tested against several allogeneic fresh tumor cells and cell lines. The actual cytotoxic
cell(s) within the TIL population is controversial; although
most TIL are reported to be cytolytic CDS-positive T-lympho
cytes (154), the antitumor effector cells were reported to be
large granular lymphocytes by others (155). Clinical trials with
TIL are under way; promising initial results have been reported
(157, 158). In one recent trial (158) 60% of 15 melanoma
patients previously not treated with IL-2 responded to therapy
with cyclophosphamide, TIL, and IL-2. Interestingly, 2 of 5
patients (40%) who had failed prior IL-2 therapy responded to
this combined therapy.
A phase I clinical trial of 7-interferon-activated autologous
monocytes was performed in patients with colon carcinoma
limited to the peritoneal cavity (159). These investigators used
countercurrent centrifugal elutriation to isolate pure prepara
tions of peripheral blood monocytes. These cells were activated
with 7-interferon and administrated to patients who had under
gone an attempted curative resection of residual i.p. colon
cancer. The therapy was well tolerated but efficacy is unknown.
Human Growth Factors
Hematopoietic cells are derived from self-renewing pluripotent stem cells. Pluripotent stem cells are able to differentiate
into committed progenitor cells which eventually give rise to
discrete cell lineages. A variety of in vitro assays are used to
examine stem cells and their progeny. The least differentiated,
pluripotent stem cell that can be identified in culture is the
CPU (colony-forming unit)-blast (160). The CFU-GEMM
(granulocytes, erythrocytes, megakaryocytes and monocytes)
assay detects a progenitor cell with limited self-renewal but the
capacity to generate all of the above cell types (161). More
committed colony-forming stem cells have been identified.
These stem cells can form erythroid, megakaryocytic and mixed
granulocyte/monocyte colonies. Growth factors are essential
for differentiation of all of the aforementioned progenitor cells.
Some growth factors are specific for one type of progenitor cell,
while others are pleiotropic and affect many types of progeni
tors (162,163). Growth factors are produced by many different
cells (164). For instance, T cells produce IL-3 and GM-CSF.
Monocytes produce M-CSF and G-CSF after contact with IL3 and GM-CSF. Monocytes also produce IL-1 and TNF which
stimulate GM-CSF, G-CSF and M-CSF production by endothelial cells. A number of growth factors can now be produced
in large quantities since the complementary DNAs have been
cloned (165-169) (Table 5). In Fig. 1, the hematopoietic cells
responsive to each of the growth factors are shown. While a
comprehensive review of growth factors is beyond the scope of
this paper, this section will focus on those that have current
clinical utility. IL-3 (multi-CSF) appears to be a pan-growth
1624
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
Table 5 Human hematopoietic growth factors
Growth
factorGM-CSFG-CSF nameCSF-alphaCSF-beta
of protein
(kD)14-3518-22
stimulated"CFU-GEMM,
CFU-GM,
BFU-E, CFU-MEG
CFU-GM, BFU-E
35-40 (dimer)
CFU-M
CSF-1
M-CSF
5q33.1
20-2612-19Chromosome5q23-3117qll.2-q21
5q23-312ql3Colonies
CFU-GEMM, CFU-GM,
Multi-CSFLymphocyte
IL-3IL-1Alternate
BFU-E, CFU-MEG
Synergy with M-CSF and IL-3
activating factorSize
°CFU-GM, colony-forming unit-granulocyte, monocyte; BFU-E, burst-forming unit-erythrocyte; CFU-GEMM, colony-forming unit-granulocyte, erythrocyte,
monocyte, megakaryocyte; CFU-MEG, colony forming unit-megakaryocyte.
*
GM-CSF
CFU-GEMM
Fig. 1. Hematopoietic cells responsive to the
various colony-stimulating factors [reproduced
by permission from Dr. J. D. Griffin (164)).
CPU-Blast, blast colony-forming unit; CFUGEMM, CPU for granulocytes. erythrocytes,
megakaryocytes, and monocytes; CFU-E, erythroid CPU; CFU-GM, granulocyte/monocyte
CFU; CFU-Mega, megakaryocyte CFU; Pro,
promyelocyte; Promono, promonocyte; Gran,
granulocyte; Mono, monocyte.
Normo
Blast
Platelets
—¿
M-CSF —¿
I
factor for all lineages. GM-CSF enhances the growth of all
progenitor cells beyond the CPU-blast and is an effective en
hancer of granulocyte and monocyte function. /// vitro admin
istration of G-CSF causes an increase in circulating neutrophils.
M-CSF causes an increase in monocyte number and function.
IL-1 represents a family of polypeptides with a wide range of
biological activities including augmentation of cellular immune
responses (T-, B-, and NK. cells); proliferation of fibroblasts;
chemotaxis of monocytes, neutrophils, and lymphocytes; stim
ulation of prostaglandin E2, increased blood neutrophils; and
neutrophil activation (170). Murine and human complementary
DNAs have been cloned (171,172). IL-1 appears to synergize
with other growth factors as well as having a survival-enhancing
or maintenance effect on primitive hematopoietic cells (173,
174). IL-1 is known to synergize with interferon and IL-2 in
enhancing tumor killing by NK cells (175).
Administration of recombinant growth factors to non-human
animals and patients have been accomplished. While IL-3 has
not been used in humans, injection into experimental animals
,
I
activates all types of progenitor cells and induces cell cycle entry
(176-178). In non-human primates, GM-CSF has been re
ported to cause an increase in neutrophils, eosinophils, platelets
and lymphocytes (179). Recently, neutropenic patients with
AIDS had an increase in neutrophil counts after receiving GMCSF (180), and patients with metastatic sarcoma who were
given recombinant GM-CSF immediately following combina
tion chemotherapy demonstrated a significant reduction in
duration and degree of neutropenia (181). GM-CSF also stim
ulated hematopoiesis in patients with myelodysplastic syn
dromes and aplastic anemia with short-term hematological
improvement (182,183). Patients with melanoma and breast
cancer receiving high dose chemotherapy and autologous bone
marrow transplantation had an accelerated granulocyte recov
ery following infusions with recombinant GM-CSF (184). The
toxicity of GM-CSF has been limited to low grade fever, myal
gias, phlebitis, and flushing. Patients with transitional cell
sarcoma of the bladder received recombinant G-CSF after the
completion of combination chemotherapy and had an absolute
1625
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
neutrophil count over three times higher than those not receiv
ing G-CSF (185) without toxicity. G-CSF was also shown to
reduce neutropenia caused by melphalan in patients with ad
vanced malignancies (186). The role for M-CSF is less clear
because it is not very effective in promoting in vitro growth of
human monocyte progenitor cells. However, it is a potent
stimulator of monocyte cytotoxicity.
There is a potential role for growth factors to decrease
myelosuppression secondary to chemotherapy and/or radiation
therapy. It appears likely that growth factors may allow for
higher doses in situations where the major toxicity is bone
marrow suppression. The increased doses may lead to better
and more durable responses. Clearly, the toxicity to other
organs will limit how high a dose can be given. In the setting
of AML a potential problem is that the myeloid leukemia cells
may proliferate in response to the growth factors (187). The
growth factors may be useful for local administration into
certain infected sites. Enhanced monocyte function by growth
factors may be clinically useful. For example, certain mono
clonal antibodies are active in monocyte-mediated, antibodydependent cellular cytotoxicity. Combination therapy with such
antibodies and M-CSF may augment tumor lysis.
Patients with pancytopenia secondary to aplastic anemia,
myelodysplasia, infections, etc., may also benefit from growth
factor therapy. While aplastic anemia patients could not be
infused continuously with growth factors they may benefit
during infections or bleeding episodes. In transient pancytopenic states growth factors may be a major benefit.
While growth factors may enhance leukemic cell growth in
vitro, it is possible that appropriate growth factor(s) may lead
to terminal differentiation of leukemic cells. Alternatively, the
stimulation of leukemic cell proliferation may be desirable if
combined with cell-cycle specific chemotherapy. Early trails
with growth factors have demonstrated their potentially impor
tant clinical role. Further trials will determine the optimum
dose schedules, toxicity and whether combinations of growth
factors are more effective than single growth factors. This is an
exciting new area of cancer research which will generate impor
tant clinical data over the next few years.
Monoclonal Antibodies
The development of technology to produce monoclonal an
tibodies created substantial enthusiasm for using this approach
in the diagnosis and treatment of cancer. Monoclonal antibod
ies are specific for single antigens, can be produced in large
quantities from ascites fluid or by tissue culture production
techniques with high degrees of purity (greater than 90%), and
can be efficiently coupled to isotopes, drugs, and toxins. The
specificity of monoclonal antibodies should theoretically reduce
toxicity to normal tissues unreactive with the antibody. Unlike
conventional antisera, there is little batch to batch variation,
and they are of a single immunoglobulin subclass.
Critical Factors for Successful Monoclonal Antibody Therapy.
Monoclonal antibodies (8) are useful for in vitro diagnosis
particularly in leukemias and lymphomas (199). In vivo appli
cations have evolved more slowly. Several critical factors need
to be addressed (Table 6). One problem is that for in vivo use
these antibodies must have minimal cross-reactivity with nor
mal tissues. Most monoclonal antibodies cross-react with some
normal tissues. This is not unexpected since these antibodies
are directed against tumor-associated rather than tumor-spe
cific antigens. To be effective these antibodies must not crossreact with antigens on normal tissues or at least the antigen
Table 6 Critical factors for monoclonal antibody tumor localization
Cross-reactivity with normal tissues.
Distribution of surface membrane antigens.
Affinity of antibody.
Antigenic modulation.
Circulating antigen.
Whole immunoglobulin r.\. fragments.
Tumor vascularization.
Tumor size.
Degree of tumor necrosis.
density should be less than on tumors. Ideally, the antigen
should be dense and homogeneous on the tumor cell surface
and the antibody should bind to the antigen with high affinity.
It is also important that the antigen-antibody complex not
dissociate from the cell membrane although internal incorpo
ration of the antigen-antibody complex by pinocytosis might be
advantageous when immunoconjugates with drugs, toxins, or
isotopes are used. Some tumor-associated antigens are present
in the blood. These might bind the antibody and prevent tumor
localization. Ideally, one should choose antibodies selective for
noncirculating antigens.
Another critical issue is the form of the antibody. Intact
immunoglobulin can be broken down into various fragments.
Intact IgG has a half-life of approximately 24 h, F(ab')2 10 h,
and Fab 90 min. The choice of the appropriate form of antibody
varies with the tumor antigen system and the conjugate. For
unlabeled antibody therapy, fragments of antibody would not
be useful as the Fc portion is critical for activating human
effector systems.
For antibody to react with tumor cells, the tumor must be
vascular. The number of blood vessels in the tumor decreases
proportionately as the tumor enlarges. In addition, as the tumor
enlarges, the diameter of the capillaries increases leading to a
decrease in the total vascular cross-sectional area of the tumor.
It is not unusual for the outer, better perfused, more viable
portions of tumors to concentrate more antibodies than the less
vascular, more necrotic interior portions. Other problems are
arteriovenous shunts. Blood entering the tumor is then shunted
to the systemic circulation before it can traverse the capillary
bed, thus preventing exchange of the antibody. In addition, the
low pH of tumors decreases capillary flexibility which further
decreases vascular perfusion.
Human Antiglobulin Response. One major problem in clinical
trials using murine monoclonal antibodies is development of
human anti-mouse antibodies (antiglobulin response). These
antibodies can form immune complexes and result in tissue
damage. They also alter the clearance and organ distribution of
injected antibodies, may neutralize the antibody, or may prevent
it from binding to tumor cells.
Development of antiglobulin varies in different tumor sys
tems (200). Patients with advanced chronic lymphocytic leu
kemia, who are typically hypogammaglobulinemic, rarely de
velop unt¡globulins (201, 202). Most patients with cutaneous
T-cell lymphomas and solid tumors will develop antiglobulins
(200). In some tumors like melanoma, only one-third to onehalf of patients developed antiglobulins (203, 204).
The specificity of the antiglobulin is important. Most antiglobulins cross-react with almost all mouse immunoglobulin
classes. However, in several cases, one component of the antiTable7 Potentialapproachesto theantiglobulinproblem
Large quantities of antibody (.-400 mg) may tolerize patient.
Cyclophosphamide may destroy the antiglobulin clone.
Human antibodies or chimeric human-mouse antibodies may be substi
tuted for murine antibodies.
Fragments of immunoglobulin may reduce antigenicity.
1626
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICALRESPONSE MODIFIERS
Table 8 Monoclonal antibody clinical trials using unlabeled antibodies
of
patients114118308243202021ToxicityFever,
DiseaseB-lymphomaB-lymphomaB-CLL"B-CLLCTCLT-ALLATLCALLAMLGastrointestinalMelanomaMelanomaAntibody/classAnti-idiotype/IgGl,IgG2a,
nausea,vomiting,
chills,
complete
5partial and
headache,diarrhea,
responses1
Ig2blF5/IgG2a(anti-CD20)Anti-idiotype/IgGland
or
transientdyspneaFever,myelosuppressionFever,
responseTransient
partial
urticariaDyspnea,
IgG2bT101/IgG2a(anti-CD5)T101/IgG2a,
hypotension,fever,
malaise.urticariaDyspnea,
anti-Leul/IgG2a(anti-CD5)Anti-Leu-
incirculating
reduction
cellsTransient
incirculating
reduction
cellsMinor
urticaria.fever,
10patientsTransient
responses in
hypotensionCoagulopathyNoneFeverFever,
l/IgG2a(anti-CDS)12E7/IgGl4H9/IgG2aAnti-Tac(anti-CD25)Anti-J5/IgG2a(anti-CD incirculating
reduction
cells1
responseTransient
partial
10)PM/81/IgM,AML-2-23/IgG2b,
incirculating
reduction
cellsTransient
arthralgia.myalgiaUrticaria,bronchospasm,
incirculating
reduction
cellsLimited
29/IgM17-lA/IgG2a9.2.27/IgG2aR24/IgG3No.
PMN
responsesNone4
mildhypotensionFever,
sicknessUrticaria,
serum
pruritis.fever,
partial responsesRef.221,222212201,202,213,214202,214,2152162202172182
wheezingEffect1
' B-CLL, B-chronic lymphocytic leukemia; CTCL, cutaneous T-cell lymphoma; ATL, adult T-cell leukemia/lymphoma; CALL, common acute lymphoblastic
leukemia; AML, acute myelogenous leukemia.
globulin appeared specific for administered antibody. This is
termed an anti-idiotype. Development of anti-idiotype antibod
ies clearly indicates a primary immune response. Responses to
other components of administered antibodies such as the Fc
fragment are rapid in onset and consist primarily of IgG sug
gesting a secondary immune response (200).
Several putative approaches are used to prevent development
of anti-globulins (Table 7). Some data suggest that the use of
fragments will reduce this problem but this is controversial
(205). In other studies, large quantities of antibodies (>400 mg)
are used to "achieve tolerance" (206); these data are also
controversial (203). In one recent study, nonspecific or unre
lated monoclonal antibodies were injected just prior to the
relevant monoclonal antibody (207). The objective was to in
crease the exogenous antibody mass and thereby render the
specific antibody less immunogenic. Other approaches to pre
vent antiglobulins include concomitant use of immunosuppressive drugs, such as azothioprine or cyclophosphamide, given at
an appropriate time to eradicate responsive clones of B cells
that would otherwise produce antiglobulin (208). Other studies
use cyclosporine to interfere with T-cell stimulation of the li
celi responses. None of these approaches has been convincingly
shown to be effective. Another approach might be using human
antibodies or genetically engineering antibodies so that the Fc
and common portions of the antibody are of human origin
whereas the Fab portion is of murine origin (209-211). These
chimeric antibodies offer the possibility of reduced "antigenicity." However, these chimeric molecules would not prevent
anti-allotypic or -idiotypic responses.
Clinical Trial with Unlabeled Antibodies. Clinical trials with
unlabeled monoclonal antibodies, i.e., not bound to drugs,
toxins, or isotopes, have resulted in only minor responses (Table
8). This was not surprising because most murine antibodies do
not activate human effector systems or have direct cytotoxic
effects. The most impressive clinical responses with unlabeled
antibodies have been with anti-idiotypic antibodies in B-ccll
lymphoma patients (221, 222) and in melanoma patients
treated with an antibody that activates human complement and
effector cells (223).
In some studies monoclonal antibodies to regulatory mole
cule receptors have been studied (224, 225). Preclinical trials
indicate responses in mice treated with monoclonal antibody
directed to epidermal growth factor (224) and transferrin recep
tors (225). A trial in patients with adult T-cell leukemia treated
with the anti-Tac antibody (anti-IL-2 receptor, or CD25 anti
gen) demonstrated a transient response in one patient; a second
patient had a 6-month remission with regression of skin lesions
and hematological abnormalities (220).
One novel therapeutic approach involves the use of mono
clonal anti-idiotype antibodies in B-cell malignancies. Unlike
the aforementioned antibodies in which the antigen is a tumorassociated antigen; anti-idiotype antibodies are directed against
a tumor-specific antigen; the idiotype of the cell surface immunoglobulin present on the malignant B-cells. Since B-cell
lymphomas and leukemias are donai, all of the malignant cells
should express the same idiotype. Since each patients' lym
phoma idiotype is unique; anti-idiotype antibodies must be
"tailor-made" for each patient.
The largest experience with anti-idiotype therapy is that of
Miller et al. (224). Their initial report of this therapy was in a
patient with rapidly progressive lymphoma resistant to chemo
therapy and Interferon. Following eight continuous 6-h i.v.
infusions spaced over the period of 1 month, the patient entered
a complete clinical remission that was sustained for 6 years
without further treatment.3 The mechanism responsible for this
is not clear. Because the antitumor
response continued long
3 R. Levy, personal communication.
1627
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
after the period of passive antibody administration, evidence of
an anti-anti-idiotype antibody response by the patient was in
vestigated; none was detected. It remains possible that indirect
mechanisms may be involved. The immune system is regulated
by networks of interactions between idiotypes and anti-idiotypes
(226). The anti-idiotype could have triggered these interactions
leading to an antiproliferative response against the tumor.
These investigators treated 10 additional patients with indi
vidually tailored anti-idiotype antibodies of different subclasses
(222). Some were treated with multiple antibodies with different
isotype or epitope specificity. Tumor responses were reported
in 50% of patients; no complete responses were observed and
most lasted for less than 6 months. Problems included antiglobulin responses and free idiotype antibody in the serum
which blocked the murine antibody and lead to fever, anthralgias, dyspnea, and headaches. A more serious problem was
emergence of idiotype variants within tumors during treatment
(227). These investigators are currently generating monoclonal
anti-idiotype antibodies that identify "shared idiotypes". Shared
anti-idiotype antibodies react with the tumor cells from more
than one patient. Panels of "shared idiotype" antibodies would
lead to a much broader application of this novel approach to
B-leukemia/lymphoma therapy.
Combination therapy with other biological response modi
fiers might increase the antitumor effect of monoclonal anti
bodies. For instance, M-CSF stimulates monocyte tumoricidal
activity and phagocytosis (164). Antibodies that act through
monocyte-dependent cellular cytotoxicity might have a greater
effect when given with M-CSF or 7-interferon (228). IL-2
activates human killer cells (98-100) and can enhance the
activity of antibodies that mediate killer cell cytotoxicity (229).
IL-2 and a-interferon have been shown to synergistically en
hance the effect of anti-idiotype antibodies in a transplantable
murine B-cell lymphoma (230, 231). A combination of IL-2
and LAK cells incubated with an appropriate monoclonal an
tibody in vitro is particularly appealing. Combination trials
such as those described are under way with several antibodies
and biologicals.
At the turn of the century, Ehrlich coined the term "magic
bullet" (232). He envisioned antibodies (at the time polyclonal
antisera) delivering toxic agents directly to tumor cells to erad
icate the tumor cells. This concept was repopularized with the
introduction of the monoclonal antibody technology. A variety
of potentially toxic molecules have been linked to monoclonal
antibodies. Most of this work has been focused on the use of
isotopes, toxins, and drugs coupled to antibodies. Some advan
tages of these immunoconjugates are reviewed in Table 9.
Radioisotopes have the advantage that the radiation field can
radiate beyond the antibody-binding cell. The extent of the
radiation field depends on the type of isotope used (discussed
below). The disadvantage is that some normal tissues may be
radiated. Another advantage of radioisotopes is that it is not
essential that they be internalized. Toxins and drugs require
Table 9 Advantages of different immunoconjugates
Radioisotopes
Large variety with widely varied characteristics.
Most isotopes radiate beyond a single cell.
Most isotopes will not require internalization.
Toxins
Extremely potent.
Well denned chemistry.
Drugs
Proven "track record" in cancer therapy.
Toxicity well defined.
Maximal tolerated doses known.
New and more potent drugs may be useful as immunoconjugates.
internalization to destroy the target cell.
Immunoconjugates with Toxins. Several potent plant and bac
terial toxins have been coupled to antibodies. Plant toxins
include ricin, abrin, gelonin, pokeweed antiviral protein, and
saporin. The most commonly studied bacterial toxins are diph
theria toxin and Pseudomonas exotoxin. All of these immunotoxin conjugates demonstrate specific antitumor cytotoxicity in
vitro and in vivo (233-237). For many toxins a single molecule
may destroy a cell. Some toxins, such as ricin, abrin, and
diphtheria toxin, consist of A and B chains. The A chain is
cytotoxic to the tumor cell by inhibition of protein synthesis.
The B chain binds galactose which is found in high density on
the surface of most cells. Entry of the A chain into cells depends
on B chain binding to the cell surface. For in vivo therapy with
immunotoxins it is necessary to isolate the A chain and covaleni ly link it to the monoclonal antibody. Elimination of the B
chain prevents nonspecific binding. Clinical trials of this ap
proach are under way (238,239). In one of these studies modest
activity was reported in patients with malignant melanoma
(239).
Immunoconjugates with Cytotoxic Drugs. Another approach
to generating immunoconjugates is by attaching cytotoxic drugs
such as doxorubicin, daunorubicin, methotrexate, vinblastine,
or melphalan to monoclonal antibodies (233, 240). The advan
tage of using drugs is that their antitumor activity and toxicity
are well defined. Conjugation to antibodies allows direct tar
geting of the drug to tumor cells and should reduce toxicity to
normal tissues. Some drugs may be more active against a tumor
when delivered to the tumor cell by a monoclonal antibody. In
addition, some potent drugs not used clinically because of
excessive toxicity may be usable when incorporated into im
munoconjugates. The disadvantage of drugs is that they are not
as potent as toxins and cannot kill cells other than the single
cell the antibody binds.
Antibody-coated liposomes containing chemotherapeutic
agents provide an alternate method of selective drug delivery.
Antibodies are either conjugated to the liposome or linked via
protein A (241). Antibody-labeled liposomes containing chemo
therapy drugs are demonstrated to increase cytotoxicity against
murine and human tumor cell lines (242, 243). A correlation
between growth inhibition and liposome internalization was
demonstrated in one study. These data suggest that this ap
proach may not be useful with antibodies that do not modulate
(244).
Immunoconjugates with Isotopes. The major limitation of
diagnostic imaging techniques is the lack of specificity. The
attractive feature of radiolabeled monoclonal antibodies is the
potential to specifically localize to tumor cells. Similarly, con
ventional radiation therapy is not specific for tumor cells. The
field that can be radiated is also limited. Radiolabeled antibod
ies should be able to radiate tumor deposits throughout the
body with minimal radiation to normal tissues (reviewed in
Refs. 245 and 246).
Diagnostics. Several radionuclides are available that can be
linked to monoclonal antibodies for diagnostic purposes. The
choice is governed by radionuclide energy, half-life, technical
requirements for conjugation, conjugate stability, safety, and
cost. It is preferable to use radionuclides with energies between
100 and 200 keV which is the optimal energy for the gamma
cameras currently in use (Table 10). The radionuclides should
have minimal paniculate radiation to maximize their safety.
They should have an adequate half-life to permit tumor local
ization and background clearance but sufficiently short to min
imize radiation exposure of the patient and medical staff.
1628
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
99mTc,'"In, and 123Ihave suitable properties for diagnostic
imaging. I31I is most often used because of its availability and
low cost. However, 13IIis not ideal because of high 7-ray energy
that degrades images, dehalogenation in vivo; its 8-day half-life
and paniculate ß
emissions limit the total dose. Currently, I23I
is too costly, is not widely available, and dehalogenates in vivo.
'"In is generally conjugated to antibodies via dictation to
^ÉÉyc
diethylenetriaminepentaacetic
acid. Nonspecific localization in
the liver and spleen has been a problem with the '"In. 99mTc
would appear to be the optimal isotope, if the problems of
kinetics and clearance of antibody can be overcome.
The first diagnostic imaging studies were with monoclonal
antibodies using I3'l-labeled anti-carcinoembryonic
antigen
^^ I^^P^H^^
monoclonal antibody. Background subtraction was required in
order for the tumor to be imaged (247). In another study I23Ilabeled antibodies that reacted with the human milk fat globule
was used (248). The first systematic human study of 13ll-labeled
monoclonal antibody Fab fragments was reponed in patients
with malignant melanoma (249). Approximately 60% of the
known sites were detected by scanning and more than 90% of
patients had at least one site detected. Tumors with diameters
<1.5 cm and those with poor antigen expression accounted for
most negative findings. Significant deiodination of the protein
in vivo was reported. Numerous other studies of iodinated
monoclonal antibodies have been reported; all have similar
problems.
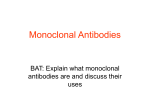
There have been a number of studies using '"In-labeled
antibodies. Lesions as small as 1 cm have been detected (250,
251) (Fig. 2). Problems encountered with "'In have been reticuloendothelial uptake of the antibody which has compromised
imaging of lesions in the liver and spleen.
Several studies report improved localization of the radiolabeled antibody when unlabeled antibody is given simultaneously
with "'In-labeled antibody (251, 252). Detection rates have
increased 2- to 3-fold using this technique. Apparently the
unlabeled antibody favorably affects the biodistribution of the
labeled antibody and improves imaging. An irrelevant antibody
that does not bind to the same site can achieve similar results.
Excellent imaging of cutaneous T-cell lymphoma patients is
observed using '"In-labeled T101 antibody (250). T101 binds
to circulating T-lymphocytes and the antigen-antibody complex
modulates internally (253). It is believed that the circulating
cells with the internalized complex traffic to the malignant
lymph nodes and skin enhancing the localization at these sites.
Concentrations of 0.01 to 0.03% injected dose per g were
achieved in diseased lymph nodes, which is approximately 10fold greater than previously achieved in other systems. A prob
lem with this study was nonspecific reticuloendothelial uptake
Table 10 Isotopes
imaging•Y-Energy
for monoclonal antibody
Isotope
(keV)"Te
14013II
Half-life
6h
siveIodine
364'"I
159'"In
8 days
13 h
3 days
Front
Rear
Fig. 2. Image of a patient with cutaneous T-cell lymphoma (with the Sézary
syndrome) taken 48 h after the i.v. injection of 5 mCi of '"In linked to 1 mg of
T101 antibody + 10 mg unlabeled TI01. Full body scans shows front (left) and
rear (right) views demonstrating excellent localization in cutaneous disease and
involved lymph nodes with nonspecific localization in the liver and spleen.
leading to localization within the liver and spleen. Some studies
in animals (254) report that linking the chelate to oxidized
carbohydrate decreases reticuloendothelial uptake. If confirmed
in humans this could improve results with "'In conjugates.
Utilizing "'In-labeled T101, immunolymphoscintigraphy
with s.c. injections intradigitally led to excellent images below
the diaphragm with minimal uptake in the liver and spleen in
patients with cutaneous T-cell lymphoma (255). This study
reported efficient and specific antibody binding in lymph nodes
nearest to the injection site with progressive uptake of remain
ing antibody in more distal nodes as proximal sites approach
saturation. In one patient, inguinal-femoral lymph node biopsy
contained over 2% of the injected dose of '"In-labeled T101
antibody at 7 days. Although this technology does not allow for
a total body image, it may offer advantages by improving the
quality of imaging in critical regions important for staging
kinetics,renal
certain
lymphoproliferative diseases.
and gas
A
diamide-dimercaptide
(N2S2) chelate was developed to label
trointestinal up
antibody with 99nTc (256). Using the N2S2 chelate, excellent
complexchemistryDehalogenation,high
take,
results in imaging malignant
melanoma were demonstrated
of an anti-melanoma antibody
chem
using F(ab'): and Fab fragments
ß-emissionsDehalogenation,expensive,
i-ray,
istry, inex
pensive,availableIodine
(257). Métastasesin skin, lymph
chem
istry1-EnergyDisadvantagesRapid
notavailableLeaches
173247AdvantagesAvailability,7-energy,inexpen
chelate.expensive,
off
affin
ity for reticuloen
dothelial system
node, lung, liver, brain, bone,
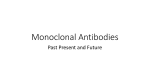
and spleen were detected as early as 6 h after injection. In Fig.
3 lymph node and subcutaneous lesions are demonstrated. A
number of these subcutaneous lesions were not detected clini
cally prior to the scan. There was no significant uptake in the
reticuloendothelial system. Biliary and renal excretions were
visualized but cleared with time. Up to 0.03% injected dose per
1629
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
l88Re, are preferred in tumors with heterogeneous
antibody
binding. This should allow for destruction of nonlabeled tumor
cells but might increase toxicity to normal tissues.
Shorter particle length radionuclides are preferred where
there is uniform antibody binding. Electron capture or internal
conversion decay radionuclides such as 125Iwould be optimal
in such a situation; other choices include «-emitters such as
211Astatine.
Anti-ferritin polyclonal antibody labeled with 131I(Table 12)
produced responses in persons with hepatomus and Hodgkin's
disease (258, 259). Single doses as high as 150 mCi were given
with acceptable hematological toxicity. Interestingly, iodinated
monoclonal anti-ferritin antibody were not as effective as pol
yclonal antibodies. Studies in animal models demonstrate that
isotope-labeled monoclonal antibodies can be effective (264).
There have been relatively few reports of human studies using
radiolabeled monoclonal antibodies. Responses have been re
ported (260) in patients treated with the anti-Lym-1 antibody
labeled with 131I.Although these patients were heavily pretreated several responded. I31l-labeled T101 antibody (150-250
Fig. 3. Image of a patient with malignant melanoma taken 8 h after the
injection of 10 mCi of ""Te linked to 10 mg of the Fab fragments of the NRMl.-05 antibody demonstrating multiple lymph node and s.c. nodules (arrows).
Blood pooling in the heart and nonspecific localization in the sinuses are also
seen.
g was observed in excised tumors. This was comparable to that
reported using "'In-labeled T101 in cutaneous T-cell lymphoma (250). Approximately 80% of known lesions were de
tected and an equal number of not previously diagnosed lesions
were found.
In summary, imaging with monoclonal antibodies is feasible.
Questionable areas can be evaluated by other techniques such
as computerized axial tomography or magnetic resonance im
aging. Some data indicate that tumors undetectable with present
techniques may be visualized with isotope-labeled monoclonal
antibodies.
Therapy. Radioisotopes such as 32P and 13II have been used
mCi) has been used to treat patients with cutaneous T cell
lymphoma (261). Responses were observed in two patients with
skin and lymph node involvement but lasted only 2 to 3 months.
Myelosuppression was dose limiting. Two B-cell lymphoma
patients were treated with 131I-labeledMB-1 (250 and 480 mCi)
with 1 partial and 1 complete response (262). Although both
had significant myelosuppression, no intervention was required.
A Phase I study of 131I-labeledFab in patients with malignant
melanoma was recently reported (249). Patients received up to
529 mCi of I31Iin divided doses; target organ toxicity was bone
marrow associated. Despite good antibody localization in se
lected patients with estimated tumor doses of 1300-5500 cGy,
anti-tumor effects were modest.
Therapy with 131I-labeled anti-ovarian antibodies i.p. dem
onstrated responses in 9 of 24 patients (263). Doses >140 mCi
were more effective than lower doses. Only patients with small
volume (<2 cm) disease responded.
The first isotope other than 131Ito enter clinical trials was
90y »OY
has a more energetic /3-particle than 131I(2.2 versus 0.6
to treat malignancies such as polyeythernia vera and metastatic
thyroid carcinoma for several years (Table 11). A reasonable
extension of this approach is to link isotopes to antibodies.
Several isotopes that can be used include «-emitters; low-,
medium-, and high-energy /3-emitters; and radionuclides that
act by electron capture and/or internal conversion (Auger elec
trons).
Choice of the appropriate radioisotope for therapy is com
plex. Longer particle length radionuclides, such as 90Y and
MeV). It is bound by diethylenetriaminepentaacetic
acid but it
has no imagible 7-ray. Rhenium has two different /3-emitting
isotopes (186Re,188Re)that are chelated by the same N2S2 ligand
used for 99mTc. Rhenium is bound irreversibly to N2S2 as is
99mTc.Both isotopes have imagible 7-ray energies. Clinical trials
with rhenium are expected to commence in 1988.
The next 2 years should see the first systematic studies of
targeting radiation therapy directly to metastatic carcinoma
with monoclonal antibodies. Issues such as single dose versus
Table 11 Isotopesfor monoclonalantibodytherapy
¡culaie
maximumenergy(MeV)2.11.10.60.4-0.62.35.97.5AdvantagesGenerator
mode17
Decay
Isotope'"Re""Re13IJ67Cu"¥'"Astatinei»!Half-life
ß3.5
h
Tcchemistry"Te
produced,
0-particleAvailability,
energetic
ß8days
chemistryIodine
specificactivityDehalogenation,
low
ß2.5
days
chemistry, inexpen
siveImagesIndium
abundant7-emission,
half-lifeAvailability,
costNo
offchetateDehalogenationNo
imaging, leaches
ß2.5
days
ß7h
days
chemistryIodine
a2.5
shortrangeIodine
chemistry,
days
Electron
capture(Auger)l'ari
chemistryDisadvantagesVery
dehalogena-tion,
imaging,
availability
1630
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
Table 12 Clinical trials with '"¡-labeled monoclonal antibodies
DiseaseHepatoma"Hodgkin's
of
patients105381862724ToxicityThrombocytopeniaMyelosuppressionFever,
41%partial
complete and
responses40%
responses2
partial
diseaseB-lymphoma
myelo-suppressionDyspnea,
rash,
B-CLLCTCL*B-LymphomaMelanomaOvarianAntibody/classAntiferritin/het-eroantiseraAntiferritin/het-eroantiseraLym-l/IgG2aT101/IgG2a(anti-CD5)MB-1/IgGl8.2/IgGlc96.5/IgG2aHMF
and
complete and 7 par
responses2
tial
urticaria,myelosuppressionMyelosuppressionMyelosuppression,
fever,
minorresponses1
partial, and 3
chills.fever,
hypotensionMyelosuppression,
fever,diarrheaEffect7%
complete and 1 par
responseNo
tial
responses9
partial responsesRefs.258259260261262249263
" Some patients were also treated with external beam irradiation and chemotherapy.
* B-CLL, B-chronic lymphocytic leukemia; CTCL, cutaneous T-cell lymphoma.
' Fab fragments were used in this study.
* i.p. therapy.
fractionated dose must be addressed in these studies. Imaging
of patients for dosimetry prior to the delivery of therapeutic
doses of isotopes is of critical importance. Parallel advances in
in vitro purging of tumor cells from bone marrow followed by
autologous bone marrow transplantation
permits the use of
bone marrow-ablating
doses of radiation if required. These
studies can be undertaken
while further advances in tumor
localization and blood clearance are pursued.
Bone Marrow Transplantation.
An attractive therapeutic ap
plication of monoclonal
antibodies is to remove tumor cells
from bone marrow prior to autotransplantation.
Patients in
clinical remission often have undetectable
tumor cells in the
bone marrow. Theoretically
these could be detected and re
moved with specific antibodies.
Most of the obstacles and
toxicities with monoclonal antibody infusion would be elimi
nated since the treatment is in vitro. Such an approach has been
reported using the anti-Bl monoclonal antibody to purge au
tologous bone marrow in patients with non-Hodgkin's
lym
phoma (265). Several antibodies
ALL (266, 267). Early results
marrow reconstitution
occurs in
well tolerated and most patients
one-third of the patients remain
were used in patients with
have demonstrated
that bone
almost all patients. Therapy is
enter remission. In ALL only
in remission for longer than 1
year, a result not different from that with allogeneic bone
marrow transplants. The results for non-Hodgkin's
lymphoma
are more promising with over 50% of the patients remaining in
remission for a median duration of 22 months. However, in the
absence of controlled trials there is no evidence in lymphoma
or ALL that results of these autotransplants
were related to the
antibody treatment.
Another transplantation
approach with monoclonal antibod
ies is to utilize antibodies in vitro for T-cell depletion. This
approach has been highly successful in preventing graft-verauhost disease but has led to higher incidences of graft rejection
and recurrent
leukemia (188-190).
Mechanisms
underlying
these adverse consequences may be due to the lack of essential
helper cell function and/or growth factors provided by T-cells
leading to graft rejection and loss of graft-vmiw-leukemia
effect
leading to recurrent leukemia.
host's immune response. The tumor-associated
antigens must
be accessible on the tumor cell to serve as a site for antibodymediated or cell-mediated
destruction.
Most studies of active
specific immunotherapy
in humans with hematological
malig
nancies have been disappointing.
For example, early studies in
ALL suggested that children could be successfully immunized
with allogeneic leukemia cells (3). These results could not be
reproduced
in controlled
trials (268, 269). Similarly, early
results in acute myelogenous leukemia patients suggested pro
longed survival with BCG and/or allogeneic leukemia cell (4,
5, 270-272) immunization.
Again, these results could not be
reproduced (7, 273).
Great promise was held for BCG immunotherapy
with or
without cellular vaccines for malignant melanoma (2); longterm results were disappointing. However, a series of interesting
studies focused on melanoma
patients demonstrated
active
immunity in patients with promising preliminary clinical results
(Table 13) (274-280).
Clinical vaccine trials for other solid tumors are limited in
number. In one trial patients with colorectal cancer with transmural extension of tumor or nodal metastasis were randomized
into groups treated by resection alone or resection with active
specific immunotherapy
with autologous tumor cells plus BCG.
At 28 months follow-up recurrences were significantly fewer in
vaccinated patients and they demonstrated
cellular immune
response to autologous tumor cells (281, 282). In a metastatic
renal cell vaccine study, 4 of 14 patients responded to vaccine
treatment with autologous tumor cells mixed with Corynebacterium parvum (283). In another study patients with bronchogenie carcinoma received a vaccine of allogeneic tumor cells in
complete Freund's adjuvant. A 10-year follow-up demonstrated
a statistically significant 5-year survival advantage for patients
treated with specific active immunotherapy
(284).
A major problem with tumor vaccines is our inability to
standardize the contents of a vaccine, particularly with reference
to the tumor-associated
antigen(s) of interest. Perhaps the antiidiotype vaccine approach discussed below will adequately ad
dress this problem.
Anti-Idiotype
Vaccines
Tumor Vaccines
Another novel approach to tumor vaccines based on the
idiotypic network hypothesis warrants discussion (226). TumorAnother potential antitumor
strategy is activation of host
associated antigens are often a part of "self and evoke a very
defenses against tumor-associated
antigens. This is referred to
poor
immune response in the tumor-bearing
host because of Tas active specific immunotherapy
which attempts to boost the
1631
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICALRESPONSE MODIFIERS
Table 13 /mmunotherapy trials for patients with malignant melanoma
No. of
patients
Stage
42
III
55
II and III
39
I and II
10
III
19
III
17
II
26
Active
immunity
Vaccine
Autologous with mela
noma cells with BCG
plus cyclophosphamide
Polyvalent melanoma anti
gen
Vaccinia melanoma oncolysate
Semiautologous melanoma
hybrids with C. parvum
Autologous melanoma cell
(±cyclophosphamide)
Reduction in CD4+ CD45+
T-cells°
69% stage II
53% stage III
64%
Positive delayed hypersensitivity
88% with cyclophosphamide;
29% without cyclophos
phamide
94% developed antibodies to
alloantigens
15% developed anti-GP2 an
tibodies.
38% developed anti-GM2
antibodies.
Allogeneic melanoma lines
with BCG or C. parvum
Allogeneic melanoma cell
lines
Clinical
results
NR"
Ref.
MR
275
Increased
survival
No responses
276
2 complete
responses
278
NR
279
NR
280
274
277
°CD4+ CD45+ T-cells are the subset that induce suppression.
* NR, not reported.
cell-mediated suppression (285, 286) and tolerance to the an
tigen (287). Recent data indicate that a weak antigen can be
turned into a strong antigen by simply changing the molecular
environment of the haptenic structure. These changes in the
hapten carrier activate T-cell help and increase the immune
response. In addition, altering the carrier can turn a tolerogenic
antigen into an immunogenic antigen. The immune status of
cancer patient is often suppressed and they can respond to only
certain T-dependent antigens but not to other antigen forms.
These considerations suggest introduction of molecular changes
into the tumor antigens before using them as vaccines. Pres
ently, this is impossible to accomplish because tumor antigens
are not well defined and are difficult to purify.
According to the idiotypic network hypothesis, certain antiidiotype antibodies express three dimensional shapes which
resemble the structure of external antigens. The existence of
such internal antigenic idiotypes comes as a statistical necessity
of the diverse and "complete" network of idiotypes (288, 289).
The internal antigens are stereochemical copies of nominal
antigens which produce specific immune responses similar to
responses induced by nominal antigen and also can compete
with normal antigens in binding assays.
Assuming one is aiming for a tumor-specific immunotherapy,
the anti-idiotype hybridoma route of making surrogate antigens
could alleviate the problem of making a large amount of purified
antigen associated with a given tumor. Furthermore, idiotypebased tumor antigens are free of the danger of transmitting
human tumor viruses which theoretically may contaminate cellbased human tumor vaccines. Parenthetically, it makes no
difference in this approach whether a de novo tumor antigen is
the target for immunotherapy or whether the target is a "nor
mal" but highly tumor-associated antigen. If a tumor-specific
hybridoma is available then a second anti-hybridoma (antiidiotypic hybridoma) can be made and selected for the structure
which represents the tumor antigen. In Fig. 4, this approach is
diagrammed. An anti-tumor-associated antibody (Abl) is gen
erated and is used to make a second antibody or an anti-idiotype
antibody (Ab2).
There are three different types of Ab2 antibodies a, 0, and 7.
The a type of Ab2 recognizes an idiotype that is distinct from
the binding site of Abl. The y type of Ab2 recognizes a target
idiotope that is close to the binding site so that it can interfere
with the antigen binding (288). The ß
type of Ab2 is the internal
image of the antigen for Ab2 (289, 290). If the ßtype is used
like an antigen, an Ab3 antibody is induced. It has an antigen-
immunize Mouse with Tumor Cell to Generote Abi
Immunize Mouse with Ab) to Generate Anti-idiotype (Ab2)
Abt
Ab2
Immunize Patients with Anti-idiotype
(Subcutaneous with
Adjuvant and/or Carrier)
Ab3
Ab2
Fig. 4. Idiotype tumor network. Concept of monoclonal anti-idiotypic vac
cines. An Abl is generated to a tumor-associated antigen. The Abl is used to
immunize mice to generate an anti-idiotypic monoclonal Ab2. The Ab2 which is
the mirror image of the tumor-associated antigen is then used to immunize
patients to generate an Ab3 response to the tumor-associated antigen. Note that
the Ab3 (or Abl') has a binding specificity identical to that of the Abl.
combining site (paratope) similar to that of Abl. Because of
this paratope similarity, the Ab3 is also called the Abl' to
indicate that it might differ in its other idiotypes from the Abl.
The cyclic nature of complementary binding sites and idiotopes serves as the basis for the idiotope vaccines. The exper
imental evidence that idiotypes or anti-idiotypes mimic antigens
and produce antitumor immunity is quite strong (288, 291293). Treatment of mice with injection of anti-idiotype that
appears to mimic tumor antigen structures has been reported
to induce antitumor immunity in human melanoma (294),
mammary adenocarcinoma (295), and rat sarcoma (296). Re
cently, anti-idiotypes produced in goats that contained antibody
components that mimic human gastrointestinal tumor-associ
ated antigens have been generated. Mice and rabbits immunized
with this anti-idiotype produced antibodies (Ab3) that bound
to human tumor antigen (297). Monoclonal anti-idiotypes to a
leukemia/lymphoma T cell associated antigen have evoked an
Ab3 response in animals (298, 299). These Ab3 anti-antiidiotypes bound to the tumor antigen and immunoprecipitated
an antigen identical to the Abl. In a clinical trial where patients
were given i.v. injections of murine antitumor antibodies, those
patients that developed an anti-idiotype response improved
clinically and had longer remissions from their disease (300).
1632
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
Indirectly, these results appeared to be consistent with the antiidiotypic hypothesis. They did not demonstrate Ab3 responses
in these patients, however. In another clinical trial (301), pa
tients with colorectal carcinoma were immunized with goat
anti-idiotypic antibodies to murine monoclonal antibody CD 171A (Abl). All patients developed Ab3 with binding specificities
on the surfaces of tumor cells similar to the Abl specificity.
The Ab3 also inhibited binding of Ab2 to Abl suggesting shared
idiotopes with Abl. Three of 30 treated patients responded. In
another clinical trial 15 patients with disseminated melanoma
were immunized with monoclonal anti-idiotypic antibodies to
a high molecular weight melanoma-associated antigen (302).
Seven patients developed antibodies (Ab3) which inhibited the
binding of anti-idiotypic antibody (Ab2) to the Abl antibody
and 3 patients showed tumor reduction. Current clinical trials
are ongoing to further study the effects of anti-idiotypic vaccine.
Conclusion
Biological therapy may be considered the "Fourth Modality
of Cancer Treatment" (321). The past decade of research has
demonstrated that there is indeed a role for biological agents
in cancer therapy. Over the next decade, combination therapies,
new cloned molecules, and more sophisticated chemistry for
immunoconjugates should lead to major advances in cancer
diagnosis and therapy.
Acknowledgments
I am indebted to Drs. R. P. Gale, M. Goldrosen, L. Vaickus, and W.
Biddle for their careful review of this manuscript, NeoRx Corporation
for the "Te scan, and Pat Alvarado for the preparation of this
manuscript.
References
Immunomodulation
Immunomodulation
is a rapidly expanding field and is appli
cable in a variety of clinical settings including autoimmune
diseases, graft rejection, as well as the treatment of cancer.
Immunomodulation
with lymphokines such as interferon and
IL-2 have been discussed previously, and the use of BCG,
Cornybacterium parvum, and other stimulants of the immune
system was also briefly reviewed. There exists a growing list of
drugs, synthetic agents, hormones, and bacterial cell products
that have immunomodulatory
activity.
Cyclophosphamide,
in relatively low doses, has an anti-sup
pressor T-cell effect. Cyclophosphamide
has been used to enhance the response to IL-2 (1 14) and tumor vaccines (274, 278)
and also as a single agent. In one melanoma study, cyclophosph amide depression of suppressor T-cells was restricted to those
patients who demonstrated
increased suppressor T-cell activity
prior to Cyclophosphamide
treatment (303). Other cytotoxic
agents such as mitoxantrone
(304, 305) and doxorubicin (306)
also have immunomodulatory
activity. Corticosteroids
have a
profound suppressive effect on both humoral and cellular im
munity and are used to treat autoimmune
diseases and graft
rejection. They are also lympholytic and are used to treat a
variety of lymphoid neoplasms. Diethylstilbestrol
(307) and the
antiestrogen
tamoxifen (308) also have immunomodulatory
activity. Cyclosporin has been shown to have suppressor effects
on both humoral and cellular arms of the immune response
(309). Nonsteroidal
antiinflammatory
agents (310), morphine
(311), marijuana (311), and antibiotics such as amikacin and
cefotoxime (312) also have immunomodulatory
activity.
A variety of synthetic agents modulate the immune system
such as polyribonucleotides
which augment natural killer activ
ity and induce interferon production (313). Thymosin fraction
S acts as an immunostimulant
and has a significant antitumor
effect in animal models (314). Removal of IgG and circulating
immune complexes by passing plasma over a protein A column
may also modulate the immune system. Responses have been
reported in a variety of cancer patients (315). Bacterial cell
products such as Bordetella pertussis (316), Corynebacterium
granulosum (317), and Listeria monocytogenes (318) and many
others have potent immunomodulatory
activity.
Another innovative approach to immunomodulation
has been
with monoclonal antibodies. The use of monoclonal antibodies
to remove T-cells prior to allogeneic bone marrow transplant
has been discussed previously (188-190). Monoclonal antibodies can also be utilized systemically to alter cell populations
such as T-cells or T-cell subsets (319, 320).
Terry, W. D., and Rosenberg, S. A. (eds.). Immunotherapy of Human
Cancer. Amsterdam: Elsevier, North-Holland BiomédicalPress, 1982.
Eilber, F. R., Morton, D. L., Holmes, E. C., et al. Adjuvant immunotherapy
with BCG in treatment of regional lymph node métastasesfrom malignant
melanoma. N. Engl. J. Med., 294: 237-240, 1976.
Mathé,G., Amiel, J. L., Schwarzenberg, L., el al. Active immunotherapy
for acute lymphoblastic leukaemia. Lancet, /: 697-699, 1969.
4- Gutterman, J. U., Hersh, E. M., Rodriguez, B., et al. Chemoimmunotherapy
of adult acute leukaemia: prolongation of remission in myeloblastic leukae
mia with BCG. Lancet, 2:1405-1409, 1974.
5. Vogler, W., Bartolucci, A. A., Omura, G. A., et al. A randomized clinical
trial of remission induction, consolidation and chemo-immunotherapy
maintenance in adult acute myeloblastic leukemia. Cancer Immunol. Immunother., 3: 163-170, 1978.
6- Mastrangelo, M. J., Berd, D., and Maguire, H. C, Jr. Current condition
and prognosis of tumor immunotherapy: a second opinion. Cancer Treat.
Rep., 68: 207-219, 1984.
7. Foon, K. A., Smalley, R. V., Riggs, C. H., and Gale, R. P. The role of
immunotherapy in acute myelogenous leukemia. Arch. Intern. Med., 143:
1726-1731, 1983.
g Kohler, G., and Milstein, C. Continuous cultures of fused cells secreting
antibody of predefined specificity. Nature (Lond.), 256:495-497, 1975.
Oldham, R. K. Biological response modifiers. J. Nati. Cancer Inst., 70:
789-796, 1983.
10. Isaacs, A., Lindenman, J. Virus interference. 1. The interferons. Proc. R.
Soc. Lond. B Biol. Sci., ¡47:258-267, 1957.
11. Stewart, W. E., II, Blalock, J. E., Burke, D. C., et al. Interferon nomencla
ture (letter). J. Immunol., 125: 2353, 1980.
12. Roth, S. M., and Foon, K. A. «-Interferon in the treatment of hématologie
malignancies. Am. J. Med., 81: 871-882, 1986.
13. Fleischmann, W. R., Kumpel, G. R., Tyring, S. K., Voss, W. R., and Baron,
S. Interferon and cancer: current use and novel approaches. In: P. S. Sunkara
(ed.), Novel Approaches to Cancer Chemotherapy, pp. 1-22. Orlando, FL:
Academic Press, 1984.
14. Sehgal, P. B. The interferon gene. Biochim. Biophys. Acta, 695: 17-33,
1982.
15- Borden, E.C. Progress toward therapeutic application of interferons 19791983. Cancer (Phila.), 54:1770-1776, 1984.
16 Epstein, L. B. Interferon-7: success, structure and speculation. Nature
(Lond.), 295:453-454, 1982.
17. Yip, Y. K., Pang, R. H. L., Urgan, C., and Vilcek, J. Partial purification
and characterization of human -y (immune) interferon. Proc. Nati. Acad.
Sci. USA, 78:1601-1605, 1981.
18. Cantell, K., and Hirvonen, S. Preparation of human leukocyte interferon
for clinical use. Tex. Rep. Biol. Med., 35: 138-144, 1977.
19. Lin, L. S., and Stewart, W. E., II. Purification of human leukocyte interferon
by two-dimensional polyacrylamide gel electrophoresis. Methods Enzymol.,
7«:481-487, 1981.
20. Berg, K., and Heron, I. Antibody affinity chromatography of human leu
kocyte interferon. Methods Enzymol., 78: 487-499, 1981.
21. Pestka, S. The purification and manufacture of human interferons. Sci.
Am., 249: 37-43, 1983.
22. Kirkwood, J. M., and Ernstoff, M. S. Interferons in the treatment of human
cancer. J. Clin. Oncol., 2: 336-352, 1984.
23. Bonnern, E. M., and Spiegel, R. J. Interferon-a: current status and future
promise. J. Biol. Response Modif., 3: 580-598, 1984.
24. Roth, M. S., and Foon, K. A. Current status of interferon therapy in
oncology. Prog. Hematol., 15:19-38, 1987.
2S- Ito, H., Murakami, K., Yanagawa, T., et al. Effect of human leukocyte
interferon on the metastatic lung tumor of osteosarcoma. Cancer (Phila.),
46:1562-1565, 1980.
26. Caparros, B., Rosen, G., and Cunningham-Rundles, S. Phase II trial of
1633
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
interferon (IFN) in metastatic osteogenic sarcoma. Proc. Am. Assoc. Cancer
Res., 23: 121, 1982.
Krown, S. E., Burk, M. W., Kirkwood, J. M., Kerr, D., Morton, D. L., and
Oettgen, H. F. Human leukocyte (a) interferon in metastatic malignant
melanoma: the American Cancer Society phase II trial. Cancer Treat. Rep.,
68: 723-726, 1984.
Retsas, S., Priestman, T. J., Newton, K. A., and Westbury, G. Evaluation
of human lymphoblastoid interferon in advanced malignant melanoma.
Cancer (Phila.), 51: 273-276, 1983.
Goldberg, R. M., Ayoob, M., Silgáis,R., Ahlgren, J. D., and Neefe, J. R.
Phase II trial of lymphoblastoid interferon in metastatic malignant mela
noma. Cancer Treat. Rep., 69: 813-816, 1985.
Creagan, E. T., Ahmann, D. L., Green, S. J., et al. Phase II study of lowdose recombinant leukocyte A interferon in disseminated malignant mela
noma. J. Clin. Oncol., 2: 1002-1005, 1984.
Kirkwood, J. M., Ernstoff, M. S., Davis, C. A., Reiss, M., Ferraresi, R.,
and Rudnick, S. A. Comparison of intramuscular and intravenous recom
binant a-2 interferon in melanoma and other cancers. Ann. Intern. Med.,
¡03:32-36, 1985.
Hersey, P., Hasic, E., MacDonald, M., et al. Effects of recombinant leuko
cyte interferon (rIFN-a A) on tumour growth and immune responses in
patients with metastatic melanoma. Br. J. Cancer, 57: 815-826, 1985.
Gutterman, J. U., Blumenschein, G. R., Alexanian, R., et al. Leukocyte
interferon-induced tumor regression in human metastatic breast cancer,
multiple myeloma, and malignant lymphoma. Ann. Intern. Med., 93: 399406, 1980.
Borden, E. C., Holland, J. F., Dao, T. L., et al. Leukocyte-derived interferon
(a) in human breast cancer. Ann. Intern. Med., 97:1-6, 1982.
Muss, H. B., Kempf, R. A., Martino, S., et al. A phase II study of
recombinant interferon in patients with recurrent or metastatic breast can
cer. J. Clin. Oncol., 2:1012-1016, 1984.
Sherwin, S. A., Mayer, D., Ochs, J. J., et al. Recombinant leukocyte A
interferon in advanced breast cancer. Ann. Intern Med., 98: 598-602,1983.
Sarna, G. P., and Figlin, R. A. Phase II trial of a-lymphoblastoid interferon
given weekly as treatment of advanced breast cancer. Cancer Treat. Rep.,
69:547-549, 1985.
Nethersell, A., Smedley, H., Katrak, M., Wheeler, T., and Sikora, K.
Recombinant interferon in advanced breast cancer. Br. J. Cancer, 49: 615620, 1984.
Quesada, J. R., Hawkins, M., Horning, S., et al. Cooperative phase I-II
study of recombinant DNA-produced leukocyte interferon (clone A) in
metastatic breast cancer, malignant lymphoma, and multiple myeloma. Am.
J. Med., 77:427-432, 1984.
Kirkwood, J. M., Harris, J. E., Vera, R., Sandier, S., Fischer, D. S.,
Khandekar, J., Ernstoffo, M. S., Gordon, L., Lutes, R., Bononie, P., Lytton,
B., Cobleigh, M., and Taylor, S. J., IV. A randomized study of low and high
doses of leukocyte -,-interferon in metastatic renal cell carcinoma: the
American Cancer Society collaborative trial. Cancer Res., 45: 863-871,
1985.
Quesada, J. R., Rios, A., Swanson, D., Trown, P., and Gutterman, J. U.
Antitumor activity of recombinant-derived interferon a in metastatic renal
cell carcinoma. J. Clin. Oncol., 3: 1522-1528, 1985.
Vugrin, D., Hood, L., Taylor, W., and Laszlo, J. Phase II study of human
lymphoblastoid interferon in patients with advanced renal carcinoma. Can
cer Treat. Rep., 69: 817-820, 1985.
Neidhart, J. A., Gagen, M. M., Young, D., Tuttle, R., Melink, T. J.,
Ziccarrelli, A., and Kisner, D. Interferon-« therapy of renal cancer. Cancer
Res., 44:4140-4143, 1984.
de Kernion, J. B., Sarna, G., Figlin, R, et al. The treatment of renal cell
carcinoma with leukocyte interferon. J. Urol., 130:1063-1066, 1983.
Krown, S. E., Real, F. X., Vadhan-Raj, S., et al. Kaposi's sarcoma and the
acquired immune deficiency syndrome. Treatment with redcombinant inter
feron a and analysis of prognostic factors. Cancer (Phila.), 57:1662-1665,
1986.
Rios, A., Mansell, P., Newell, G. R., Reuben, J. M., Hersh, E. M., and
Gutterman, J. U. Treatment of acquired immunodeficiency syndrome-re
lated Kaposi's sarcoma with lymphoblastoid interferon. J. Clin. Oncol., 3:
506-512, 1985.
Groopman, J. E., Gottlieb, M. S., Goodman, J., el al. Recombinant a-2
interferon therapy for Kaposi's sarcoma associated with the acquired immunodeficiency syndrome. Ann. Intern. Med., 700:671-676, 1984.
Figlin, R. A., Sarna, G. P. Human leukocyte interferon (IFN): phase II
trials in non-small cell lung cancer (NSCLC) and adenocarcinoma of the
colon/rectum. Proc. Am. Soc. Clin. Oncol., 2:45, 1983.
Figlin, R. A., Callaghan, M., and Sarna, G. Phase II trial of (human
leukocyte) interferon administered daily in adenocarcinoma of the colon/
rectum. Cancer Treat. Rep., 67: 493-494, 1983.
Chaplinski, T., Laszlo, J., Moore, J., and Silverman, P. Phase II trial of
lymphoblastoid interferon in metastatic colon carcinoma. Cancer Treat.
Rep., 67:1009-1012,1983.
Neefe, J. R., Silgáis,R., Ayoob, M., and Schein, P. S. Minimal activity of
recombinant clone A interferon in metastatic colon cancer. J. Biol. Response
Modif., 3: 366-370, 1984.
Eggermont, A. M., Weimar, W., Marguet, R. L., Lameris, J. D., and Jeekel,
J. Phase II trial of high-dose recombinant leukocyte a-2 interferon for
metastatic coloréela!cancer without previous systemic treatment. Cancer
Treat. Rep., 69: 185-187, 1985.
Jones, D. H., Bleechan, N. M., Slater, A. J., et al. Human lymphoblastoid
interferon in the treatment of small cell carcinoma of the lung. Br. J. Cancer,
47:361-366, 1983.
54. Grunberg, S. M., Kempf, R. A., Uri, I. M., Venturi, C. L., Bosell, W. D.,
Jr., and Mitchell, M. S. Phase II study of recombinant a interferon in the
treatment of advanced non small cell lung carcinoma. Cancer Treat. Rep.,
69: 1031-1032, 1985.
55. Einhorn, N., Cantei!, K., Einhorn, S., and Strander, H. Human leukocyte
interferon therapy for advanced ovarian carcinoma. Am. J. Clin. Oncol., 5:
167-172, 1982.
56. Niloff, J. M., Knapp, R. C., Jones, G., Schaetzl, E. M., and Bast, R. C.
Recombinant leukocyte a interferon in advanced ovarian carcinoma. Cancer
Treat. Rep., 69: 895-896, 1985.
57. Torti, F. M., Shortliffe, L. D., Williams, R. D., et al. a-Interferon in
superficial bladder cancer: a Northern California Oncology Group Study. J.
Clin. Oncol., 6:476-483, 1988.
58. Ikic, D., Maricic, /.., Oresic, V., et al. Applications of human leucocyte
interferon in patients with urinary bladder papillomatosis, breast cancer and
melanoma. Lancet, /: 1022-1024, 1981.
59. Scorticatti, C. H., de la Pena, N. C., Bellora, O. G., et al. Systemic IFN-a
treatment of multiple bladder papilloma grade I or II patients: pilot study.
J. Interferon Res., 2: 339-343, 1982.
60. Ikic, D., Brodarec, I., Padovan, I., Knezevic, M., and Soos, E. Applications
of human leukocyte interferon in patients with tumours of the head and
neck. Lancet, 7: 1025-1027,1981.
61. Padovan, I., Brodarec, I., Ikic, D., et al. Effect of interferon in therapy of
skin and head and neck tumors. J. Cancer Res. Clin. Oncol., 100:295-310,
1981.
62. Connors, J. M., Andiman, W. A., Howarth, C. B., et al. Treatment of
nasopharyngeal carcinoma with human leukocyte interferon. J. Clin. Oncol.,
3:813-817,1985.
63. Ikic, D., Kirhmajer, V., Maricic, /... et al. Application of human leucocyte
interferon in patients with carcinoma of the uterine cervix. Lancet, 1:10271030, 1981.
64. Quesada, J. R., Reuben, J., Manning, J. T., Hirsch, E. M., and Gutterman,
J. U. a interferon for induction of remission in hairy cell leukemia. N. Engl.
J. Med., 370:15-18, 1984.
65. Quesada, J. R., Hersh, E. M., Manning, J. T., et al. Treatment of hairy cell
leukemia with recombinant a interferon. Blood, 68:493-497, 1986.
66. Ratain, M. J., Golomb, H. M., Vardiman, J. W., Vokes, E. E., Jacobs, R.
H., and Daly, K. Treatment of hairy cell leukemia with recombinant a-2
interferon. Blood, 65: 644-648, 1985.
67. Jacobs, A. D., Champlin, R. E., and Golde, D. W. Recombinant a-2interferon for hairy cell leukemia. Blood, 65: 1017-1020, 1985.
68. Foon, K. A., Maluish, A. E., Abrams, P. G., et al. Recombinant leukocyte
A interferon therapy for advanced hairy cell leukemia: therapeutic and
immunologie results. Am. J. Med., 80: 351-356, 1986.
69. Thompson, J. A., Brady, J., Kidd, P., and Fefer, A. Recombinant a-2
interferon in the treatment of hairy cell leukemia. Cancer Treat. Rep., 69:
791-793, 1985.
70. Worman, C. P., Catovsky, D., Bevan, P. C., et al. Interferon is effective in
hairy cell leukemia. Br. J. Haematol., 60:759-763,1985.
71. Ratain, M. H., Golomb, H. M., Bardawil, R. G., et al. Durability of
responses to interferon a-2b in advanced hairy cell leukemia. Blood, 69:
872-877, 1987.
72. Spiers, S. D. C., Moore, D., Cassileth, P. A., et al. Hairy cell leukemia:
complete remission with pentostatin (2'-deoxycoformycin). N. Engl. J.
Med., 3/6:825-830, 1987.
73. Moormeier, J., Ratain, M., Westbrook, C., Vardiman, J., Daly, K., and
Golomb, H. M. Low dose interferon in the treatment of hairy cell leukemia.
Proc. Am. Assoc. Cancer Res., 29: 215, 1988.
74. Foon, K. A., Sherwin, S. A., and Abrams, P. G. Treatment of advanced
non-Hodgkin's lymphoma with recombinant leukocyte A interferon. N.
Engl. J. Med., 377: 1148-1152, 1984.
75. Leavitt, R. D., Ratanatharathorn, V., Ozer, H., et al. a-2b interferon in the
treatment of Hodgkin's disease and non-Hodgkin's lymphoma. Semin.
Oncol., 74:18-23, 1987.
76. Horning, S. J., Merigan, T. C., Krown, S. E., et al. Human interferon a in
malignant lymphoma and Hodgkin's disease. Cancer (Phila.), 56: 13051310, 1985.
77. O'Connell, M. J., Colgan, J. P., Oken, M. M., Ritts, R. E., Jr., Kay, N. E.,
78.
79.
80.
81.
82.
and Itri, L. M. Clinical trial of recombinant leukocyte A interferon as initial
therapy for favorable histology non-Hodgkin's lymphomas and chronic
lymphocytic leukemia. An Eastern Cooperative Oncology Group pilot study.
J. Clin. Oncol., 4:128-136, 1986.
Bunn, P. A., Idhe, D. C., and Foon, K. A. The role of recombinant leukocyte
A interferon in the therapy of cutaneous T-cell lymphomas. Cancer (Phila.),
57:1315-1321, 1986.
Bunn, P. A., Foon, K. A., Ihde, D. C., et al. Recombinant leukocyte A
interferon: an active agent in advanced cutaneous T-cell lymphomas. Ann.
Intern. Med., 707:484-487, 1984.
Olsen, E. A., Rosen, S. T., Vollmer, R. T., et al. Interferon o-2a in the
treatment of cutaneous T cell lymphoma. J. Am. Acad. Dermatol., in press,
1989.
Misset, J. L., Mathc, G., Gastiabuni, J., et al. Treatment of leukemias and
lymphomas by interferons: phase II trial of chronic lymphoid leukemia by
human interferon a+. Biomed. Pharmacother., 36:112-116, 1982.
Schulof, R. S., Lloyd, M. J., Stallings, J. J., et al. Recombinant leukocyte
A interferon in B cell chronic lymphocytic leukemia: in vivo effects on
1634
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
autologous antitumor immunity. J. Biol. Response Mod it'.. 4: 310-323,
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
1985.
Rozman, C, Montserrat, E., VÃ-nolas,N., et al. Recombinant a2-interferon
in the treatment of B chronic lymphocytic leukemia in early stages. Blood,
71:1295-1298, 1988.
Pangalis, G. A., and Griva, E. Recombinant n-2b-interferon in untreated
stages A and B chronic lymphocytic leukemia: a preliminary report. Cancer
(Phila.), 61: 869-872, 1988.
Costanzi, J. J., Cooper, M. R., Scarffe, J. H., et al. Phase II study of
recombinant a-2 ¡murieronin resistant multiple myeloma. J. Clin. Oncol.,
5:654-659, 1985.
Wagstaff, J., Loynds, P., and Scarffe, J. H. Phase II study of rDNA human
a-2 interferon in multiple myeloma. Cancer Treat. Rep., 69:495-498,1985.
Ohno, R., and Kimura, K. Treatment of multiple myeloma with recombinant
interferon a-2a. Cancer (Phila.), 57: 1685-1688, 1986.
Talpaz, M., Kantarjian, H. M., McCredie, K.. Trujillo, J. M., Keating. M.
J., and Gutterman, J. V. Hématologieremission and cytogenetic improve
ment induced by recombinant human interferon a A in chronic myelogenous
leukemia. N. Engl. J. Med., 314: 1065-1069, 1986.
Hill, N. O., Pardue, A., Khan, A., Alemán,C., Hilario, R., and Hill, J. M.
Clinical trials of human leukocyte interferon in malignancy. Tex. Rep. Biol.
Med., 41:634-640, 1981-82.
Oberg, K., Fuña,K., and Aim, G. Effects of leukocyte interferon on clinical
symptoms and hormone levels in patients with midgut carcinoid tumors and
carcinoid syndrome. N. Engl. J. Med., 309: 129-133, 1983.
Foon, K. A., Bottino, G., and Abrams, P. G. Phase II trial of recombinant
leukocyte A interferon in patients with advanced chronic lymphocytic leu
kemia. Am. J. Med., 78: 216-220, 1985.
Kur/rock. R., Talpaz, M., Kantarjian, H., et al. Therapy of chronic myelog
enous leukemia with recombinant interferon-7. Blood, 70: 943-947, 1987.
Kurzrock, R., Quesada, J. R., Talpaz, M., et al. Phase I study of multiple
dose intramuscularly administered recombinant 7 interferon. J. Clin. On
col., 4:1101-1109, 1985.
Foon, K. A., Maluish, A., Sherwin, S. A., et al. A phase I trial of recombinant
y interferon in patients with cancer. Cancer Immunol. Immunother., 20:
193-197, 1985.
Ernstoff, M. S., Trautman, T., Davis, C. A., et al. A randomized Phase I/
II study of continuous versus intermittent intravenous interferon -. in pa
tients with metastatic melanoma. J. Clin. Oncol., 5: 1804-1810, 1987.
Maluish, A. E., Urba, W. J., Longo, D. L., et al. The determination of an
immunologically active dose of interferon--y in patients with melanoma. J.
Clin. Oncol., 6:434-445, 1988.
Lotze, M. T., Matory, Y. L., Ettinghausen, S. E., et al. In vivoadministration
of purified human interleukin 2. II. Half-life, immunologie effects, and
expansion of peripheral lymphoid cells in vivo with recombinant IL 2. J.
Immunol., 135: 2865-2875, 1985.
Lotze, M. T., Line, B. T., Mathisen, D. J., et al. The in vivo distribution of
autologous human and murine lymphoid cells grown in T cell growth factor
(TCGF): implications for the adoptive immunotherapy of tumors. J. Im
munol., 125:1487-1493, 1980.
Lotze, M. T., Grimm, E. A., Mazumder, A., et al. Lysis of fresh and cultured
autologous tumor by human lymphocytes cultured in T-cell growth factor
(TCGF). Cancer Res., 41:4420-4425, 1981.
Grimm, E. A., Robb, R. J., Roth, J. A., et al. Lymphokine-activated killer
cell phenomenon. Ill Evidence that IL-2 is sufficient for direct activation of
peripheral blood lymphocytes into lymphokine-activated killer cells. J. Exp.
Med., 158: 1356-1361, 1983.
Rosenberg, S. A., Lotze, M. T., Muul, L. M., et al. Observations on the
systemic administration of autologous lymphokine-activated killer cells and
recombinant interleukin-2 to patients with metastatic cancer. N. Engl. J.
Med., 313: 1485-1492, 1985.
Rosenberg, S. A., Spiess, P., and Lafreniere, R. A new approach to the
adoptive immunotherapy of cancer with tumor-infiltrating lymphocytes.
Science (Wash. DC), 233: 1318-1321, 1986.
Cohen, P. J., Lotze, M. T., Roberts, J. R., et al. The immunopathology of
sequential tumor biopsies in patients treated with interleukin-2: correlation
of response with T-cell infiltration and HLA-DR expression. Am. J. Pathol.,
729:208-216,1987.
Cotran, R. S., Pober, J. S., Gimbrone, M. A., Jr., et al. Endothelial
activation during interleukin-2 (IL-2) immunotherapy: a possible mecha
nism for the vascular leak syndrome. J. Immunol., 140: 1883-1888, 1988.
Lotze, M. T., Frana, L. W., Sharrow, S. O., et al. In vivo administration of
purified human interleukin-2. I. Half-life and immunologie effects of the
Jurkat cell line-derived interleukin-2. J. Immunol., 134: 157-166, 1985.
Lafreniere, R., and Rosenberg, S. A. Successful immunotherapy of murine
experimental hepatic métastaseswith lymphokine-activated killer cells and
recombinant interleukin-2. Cancer Res., 45: 3735-3741, 1985.
Rosenberg, S. A., Mule, J. J., Spiess, P. J., et al. Regression of established
pulmonary métastasesand subcutaneous tumor mediated by the systemic
administration of high-dose recombinant interleukin-2. J. Exp. Med., ¡61:
1169-1188,1985.
Mule, J. J., Yang, J. C., Lafreniere, R., et al. Identification of cellular
mechanisms operational in vivo during the regression of established pul
monary métastasesby the systemic administration of high-dose recombinant
interleukin 2. J. Immunol., 139: 285-294, 1987.
Lotze, M. T., and Rosenberg, S. A. The immunologie treatment of cancer.
CA—Cancer J. Clin., 38:68-94, 1988.
Lotze, M. T., Custer, M. C., Sharrow, S. O., et al. In vivo administration of
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
135.
136.
purified human interleukin-2 to patients with cancer: development of inter
leukin-2 receptor positive cells and circulating soluble interleukin-2 recep
tors following IL-2 administration. Cancer Res., 47: 2188-2195, 1987.
Rosenberg, S. A., Lotze, M. T., Muul, L. M., et al. A progressive report on
the treatment of 157 patients with advanced cancer using lymphokine
activated killer cells and interleukin-2 or high dose interleukin-2 alone. N.
Engl. J. Med., 316:889-897,1987.
Damle, N. K.. Doyle, L. V., Bender. J. R., and Bradley, E. C. Interleukin
2-activated human lymphocytes exhibit enhanced adhesion to normal vas
cular endothelial cells and cause their lysis. J. Immunol., 138: 1779-1785,
1987.
Lotze, M. T., Chang, A. R., Seipp, C. A., et al. High-dose recombinant
interleukin 2 in the treatment of patients with disseminated cancer: re
sponses, treatment-related morbidity, and histologie findings. JAMA, 256:
3117-3124,1986.
Mitchell, M. S.. Kempf, R. A., Harel, W.,etal. Effectiveness and tolerability
of low-dose cyclophosphamide and low-dose intravenous interleukin-2 dis
seminated melanoma. J. Clin. Oncol., 6:409-424, 1988.
Krigel, R., Padavic, K., Rudolph, A., and Comis. R. Phase II study of
recombinant interleukin-2 (rIL-2) plus recombinant 0-interferon (1FN-/3) in
advanced renal cell carcinoma. Proc. Am. Soc. Clin. Oncol., 7: 132, 1988.
Carswell, E. A., Old, L. J., Kassel, R. L., Green, S., Fiore, N., and
Williamson, B. An endotoxin-induced serum factor that causes necrosis of
tumors. Proc. Nati. Acad. Sci. USA, 72: 3666-3670, 1975.
Beutler, B., Greenwald, D., Hulmes, J. D., et al. Identity of tumour necrosis
factor and the macrophage-secreted factor cachectin. Nature (Lond.), 318:
522-524, 1985.
Aggarwal. B. B., Henzel, W. J., Moffat, B., Kohr, W. J., and Harkins, R.
N. Primary structure of human lymphotoxin derived from 1788 lymphoblastoid cell line. J. Biol. Chem., 260: 2334-2344, 1985.
Aggarwal, B. B., Kohr, W. J., Hass, P. E., et al. Human tumor necrosis
factor. J. Biol. Chem., 260: 2345-2354, 1985.
Shirai, T., Yamaguchi, H., Ito, H., Todd, C. W., and Wallace, R. B. Cloning
and expression in Escherichia coli of the gene for human tumour necrosis
factor. Nature (Lond.), 313: 803-806, 1985.
Gray, P. W., Aggarwal, B. B., Benton, C. V., et al. Cloning and expression
of cDNA for human lymphotoxin, a lymphokine with tumour necrosis
activity. Nature (Lond.), 312: 721-729, 1984.
Pennica, D., Nedwin, G. E., Hayflick, J. S., et al. Human tumour necrosis
factor: precursor structure, expression and homology to lymphotoxin. Na
ture (Lond.), 312: 721-729, 1984.
Aggarwal, B. B., Kohr, W. J., Hass, P. E., et al. Human tumor necrosis
factor. Production, purification and characterization. J. Biol. Chem., 260:
2345-2354, 1985.
Wang, A. M., Creasey, A. A., Ladner, M. B., et al. Molecular cloning of
the complementary DNA for human tumor necrosis factor. Science (Wash.
DC), 22«:149-154, 1985.
Carswell, E. A., Old, L. J., Kassel, R. L., Green, S., Fiore, N., and
Williamson, B. An endotoxin-induced serum factor that causes necrosis of
tumors. Proc. Nati. Acad. Sci. USA, 72: 3666-3670, 1975.
Carswell, E. A., Green, S., Everson, T. C., et al. Effect of tumor necrosis
factor on cultured human melanoma cells. Nature (Lond.), 258: 731-732,
1975.
Haranaka, K., and Satomi, N. Cytotoxic activity of tumor necrosis factor
(TNF) on human cancer cells in vitro. Jpn. J. Exp. Med., 51: 191-194,
1981.
Haranaka, K. H., Satomi, N., and Sakurai, A. Antitumor activity of murine
tumor necrosis factor (TNF) against transplanted murine tumors and heterotransplanted human tumors in nude mice. Int. J. Cancer, 34: 263-267,
1984.
Sherman, M. L., Spriggs, D. R., Arthur, K. A., Imamura, K., Frei, E., Ili,
and Kufe, D. W. Recombinant human tumor necrosis factor administered
as a five-day continuous infusion in cancer patients: phase I toxicity and
effects on lipid metabolism. J. Clin. Oncol., 6: 344-350, 1988.
Blick, M., Sherwin, S. A., Rosenblum, M., and Gutterman, J. Phase I study
of recombinant tumor necrosis factor in cancer patients. Cancer Res., 47:
2986-2989, 1987.
Kimura, K., Taguchi, T., Urushizaki, I., et al. Phase I study of recombinant
human tumor necrosis factor. Cancer Chemother. Pharmacol., 20: 223229, 1987.
Creaven, P. J., Plager, J. E., Dupere, S., et al. Phase I clinical trial of
recombinant human tumor necrosis factor. Cancer Chemother. Pharmacol.,
20:137-144, 1987.
Williamson, B. D., Carswell, E. A., Rubin, B. Y., Prendergast, J. S., and
Old, L. J. Human tumor necrosis factor produced by human II crii lines;
synergistic cytotoxin interaction with human interferon. Proc. Nati. Acad.
Sci. USA, 80: 5397-5401, 1983.
Sugarman, B. J., Aggarwal, B. B., Hass, P. E., Figari, I. S., l'alludimi, M.
A., Jr., and Shepard, M. J. Recombinant human tumor necrosis factor-a;
effect on proliferation of normal and transformed cells in vitro. Science
(Wash. DC), 230: 943-945, 1985.
Kloke, O., Kummer, G., Matika, S., Niederle, N., and Schmidt, C. G.
Synergistic effects of tumor necrosis factor and interferon a-2b on the
proliferation and differentiation of HL60 cells. Proc. Am. Assoc. Cancer
Res., 29:415, 1988.
Krosnick, J. A., Mule, J. J., and Rosenberg, S. A. Synergistic anti-tumor
efficacy of recombinant tumor necrosis factor and chemotherapeutic agents
in vivo. Proc. Am. Assoc. Cancer Res., 29:432, 1988.
1635
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
137. Grimm, E. A., Mazumder, A., Zhang, H. Z., and Rosenberg, S. A. The
lymphokine activated killer cell phenomenon: lysis of natural killer resistant
fresh solid tumor cells by interleukin 2 activated autologous human periph
eral blood lymphocytes. J. Exp. Med., 755: 1823-1841, 1982.
138. Roberts, K., Lotze, M. T., and Rosenberg, S. A. Separation and functional
studies of the human lymphokine-activated killer cell. Cancer Res., 47:
4366-4371, 1987.
139. West, W. H., Tauer, K. W., Yannelli, J. R., et al. Constant-infusion
recombinant interleukin-2 in adoptive immunotherapy of advanced cancer.
N. Engl. J. Med., 316: 898-905, 1987.
140. Fisher, R. I., Coliman, C. A., Jr., Doroshow, J. H., et al. Metastatic renai
cancer treated with interleukin-2 and lymphokine-activated killer cells: a
phase II clinical trial. Ann. Intern. Med., 70«:518-523, 1988.
141. Paciucci, P. A., Bhardwaj, R., Odchimar, R., Glidewell, O., and Holland,
J. F. Immunotherapy for metastatic cancer with recombinant interleukin-2
(rIL2) by continuous infusion with and without adoptive cell transfer. Proc.
Am. Soc. Clin. Oncol., 7: 163, 1988.
142. West, W. H., Tauer, K. W., Schwartzberg, L. S., Marshall, G. D., Orr, D.
W., and Oldham, R. K. Constant infusion recombinant interleukin-2 (rIL2) in the treatment of advanced renal carcinoma. Proc. Am. Soc. Clin.
Oncol., 7: 124, 1988.
143. Stahel, R. A., Sculier, J. P., Jost, L., et al. IL-2 and lymphokine activated
killer cells (IL-2/LAK) in solid tumors. Proc. Am. Soc. Clin. Oncol., 7:125,
1988.
144. Rayner, A. A., Lionetto, R., Atkins, M. B., et al. Phase II trial of inter leukin
2 bolus priming followed by continuous infusion with lymphokine activated
killer cells (IL-2/LAK) in metastatic melanoma. Proc. Am. Soc. Clin.
Oncol., 7: 246, 1988.
145. Barba, D., Oldfield, E. H., Saris, S. C, Rosenberg, S. A., Hamilton, J. M.
Phase II immunotherapy of cystic primary brain tumors (PBT) with IL-2/
LAK cells. Proc. Am. Soc. Clin. Oncol., 7: 82, 1988.
146. Sosman, J. A., Kohler, P. C., Hank, J. A., et al. Repetitive weekly cycles of
interleukin-2 (rIL-2): effects of dose, schedule of administration and indomethacin on parameters of biologic and immune function. Proc. Am. Soc.
Clin. Oncol., 7:172, 1988.
147. Steis, R., Bookman, M., Clark, J., et al. IntraperÃ-toneal lymphokine acti
vates killer (LAK) cell and interleukin-2 therapy for peritoneal carcinomatosis: toxicity, efficacy and laboratory results. Proc. Am. Soc. Clin. Oncol.,
6:250, 1987.
148. Oldham, R. K., Banal, A. H., Birch, R., et al. Regional adoptive immunotherapy with IL-2 activated cells in patients with metastatic cancer. Proc.
Am. Soc. Clin. Oncol., 7: 172, 1988.
149. Stewart, J., Belinson, J., Grant, B., et al. Phase I evaluation of intraperitoneal (IP) interleukin-2 (IL-2) and lymphokine activated killer cells (LAK)
in patients with ovarian cancer. Proc. Am. Soc. Clin. Oncol., 7: 162, 1988.
150. Kowal, C., Baldiserri, M., Roth, A., et al. Phase I-II trial of intraperitoneal
(IP) interleukin-2 (IL-2) in refractory stage III ovarian cancer (OVCA): a
search for optimal biological dosage. Proc. Am. Soc. Clin. Oncol., 7: 141,
1988.
151. Mavligit, G., Charnsangavej, C., Talpaz, M., Gutterman, J., and Wallace,
C. Splenic versus hepatic artery infusion of recombinant interleukin-2 (rIL2) for patients with liver métastases.Proc. Am. Soc. Clin. Oncol., 7: 207,
1988.
152. Mule, J. J., Smith, C. A., and Rosenberg, S. A. Interleukin-4 (B-cell
stimulatory factor-1) can mediate the induction of LAK activity directed
against fresh tumor cells. J. Exp. Med., 760: 792-797, 1987.
153. Itoli. K., Tilden, A. B., and Balch, C. M. Interleukin 2 activation of cytotoxic
T-lymphocytes infiltrating into human metastatic melanomas. Cancer Res.,
Â¥6:3011-3017, 1986.
154. Belldegrum, A., Muul, L. M., and Rosenberg, S. A. Interleukin 2 expanded
tumor-infiltrating lymphocytes in human renal cell cancer. Isolation, characterization, and antitumor activity. Cancer Res., 48: 206-217, 1988.
155. Heo, D. S., Whiteside, T. L., Johnson, J. T., Chen, K., Barnes, E. L., and
Herberman, R. B. Long-term interleukin-2 dependent growth and cytotoxic
activity of tumor-infiltrating lymphocytes from human squamous cell carcinomas of the head and neck. Cancer Res., 47:6353-6362, 1987.
156. Muul, L. M., Spiess, P. J., Director, E. P., and Rosenberg, S. A. Identifi
cation of specific cytolytic immune responses against autologous tumor in
humans bearing malignant melanoma. J. Immunol., 138:989-995, 1987.
157. Tapalian, S. L., Solomon, D., Avis, F. P., et al. Immunotherapy of patients
with advanced cancer using tumor-infiltrating lymphocytes and recombinant
interleukin-2: a pilot study. J. Clin. Oncol., 6: 839-853, 1988.
158. Rosenberg, S. A., Packard, B. S., Aebersold, P. M., et al. Use of tumorinfiltrating lymphocytes and interleukin-2 in the immunotherapy of patients
with metastatic melanoma. A preliminary report. N. Engl. J. Med., 319:
1676-1680, 1988.
159. Stevenson, H. C., Keenan, A.M., Woodhouse, C., et al. Fate of y-interferonactivated killer blood monocytes adoptively transferred into the abdominal
cavity of patients with peritoneal carcinomatosis. Cancer Res., 47: 61006103, 1987.
160. Leary, A. G., and Ogawa, M. Blast cell colony assay for umbilical cord
blood and adult bone marrow progenitors. Blood, 69: 953-959, 1987.
161. Fauser, A. A., and Messner, H. A. Identification of megakaryocytes, macrophages and eosinophils in colonies of human bone marrow containing
neutrophilic granulocytes and erythroblasts. Blood, 53: 1023-1027, 1979.
162. Metcalf, D. The molecular biology and functions of the granulocyte-macrophage colony-stimulating factors. Blood, 67: 257-267, 1986.
163. Clark, S. C., and Kamen, R. The human hematopoietic colony-stimulating
factors. Science (Wash. DC), 236: 1229-1237, 1987.
164. Griffin, J. D. Clinical applications of colony-stimulating factors. Oncology
(Basel), Z-15-21, 1988.
165. Yang, Y-C, Ciarletta, A. B., Temple, P. A., et al. Human IL-3 (multi-CSF):
identification by expression cloning of a novel hemapoietic growth factor
related to murine IL-3. Cell, 47: 3-10, 1986.
166. Wong, G. G., Witek, J. S., Temple, P. A., et al. Human GM-CSF: molecular
cloning of the complementary DNA and purification of the natural and
recombinant proteins. Science (Wash. DC), 228: 810-815, 1985.
167. Souza, L. M., Boone, T. C., Gabrilove, J., et al. Recombinant human
granulocyte colony-stimulating factor. Effects on normal and leukemic
myeloid cells. Science (Wash. DC), 232: 61-65, 1986.
168. Kawasaki, E. S., Ladner, M. B., Wang, A. M., et al. Molecular cloning of a
complementary DNA encoding human macrophage-specific colony stimu
lating factor (CSF-1). Science (Wash. DC), 230: 291-296, 1985.
169. Wong, G. G., Temple, P. A., Leary, A. C., et al. Human CSF-1: molecular
cloning and expression of 4-kb cDNA encoding the human urinary protein.
Science (Wash. DC), 235: 1504-1509, 1987.
170. Dinarello, C. A. An update on human interleukin-1: from molecular biology
to clinical relevance. J. Clin. Immunol., 5: 287-297, 1985.
171. Auron, P. E., Webb, A. C., Rosenwasser, L. J., et al. Nucleotide sequence
of human monocyte interleukin-1 precursor cDNA. Proc. Nati. Acad. Sci.
USA, «7:7907-7911, 1984.
172. Lomedico, P. T., Gubler, U., Hellman, C. P., et al. Cloning and expression
of murine interleukin-1 in Escherichia coli. Nature (Lond.l, 312: 458-462,
1984.
173. Zsebo, K. M., Wypych, J., Yuschenkoff, V. N., et al. Effects of hematopoietin-1 and interleukin-1 activities on early hematopoietic cells of the
bone marrow. Blood, 71: 962-968, 1988.
174. Fibbe, W. E., van Damme, J., Billiau, A., et al. Interleukin-1 (IL-1) stimu
lates myeloid progenitor cells to proliferate in human long term bone
marrow cultures. Blood, 70(Suppl. 1): 172a, 1987.
175. Dempsey, R. A., Dinarello, C. A., Mier, J. W., et al. The differential effects
of human leukocytic pyrogen/lymphocyte activating factor, T cell growth
factor and interferon on human natural killer cell activity. J. Immunol., 729:
2504-2510, 1982.
176. Metcalf, D., Begley, C. G., Johnson, G. R., et al. Effects of purified
bacterially synthesized murine multi-CSF (IL-3) on hematopoiesis in normal
adult mice. Blood, 68:46-57, 1986.
177. Kindler, V.. Thorens, B., de Kossodi, S., et al. Stimulation of hematopoiesis
in vivo by recombinant bacterial murine interleukin-3. Proc. Nati. Acad. Sci.
USA, 83:1001-1005, 1986.
178. Broxmeyer, H. E., Williams, D. E., Cooper, S., et al. Comparative effects
in vivo of recombinant murine interleukin-3, natural murine colony-stimu
lating factor-1, and recombinant murine granulocyte-macrophage colonystimulating factor on myelopoiesis in mice. J. Clin. Invest., 79: 721-730,
1987.
179. Donahue, R. E., Wang, E. A., Stone, D. K., et al. Stimulation of haematopoiesis in primates by continuous infusion of recombinant human GM-CSF.
Nature (Lond.), 321: 872-875, 1986.
180. Groopman, J. E., Mitsuyasu, R. T., DeLeo, M. J., et al. Effects of recom
binant human granulocyte-macrophage colony-stimulating factor on mye
lopoiesis in the acquired immunodeficiency syndrome. N. Engl. J. Med.,
577:593-598,1987.
181. Antman, K. S., Griffin, J. D., Elias, A., et al. Effect of recombinant human
granulocyte-macrophage colony-stimulating factor on chemotherapy-in
duced myelosuppression. N. Engl. J. Med., 319: 593-604, 1988.
182. Vadhan-Raj, S., Keating, M., LeMaistre, A., et al. Effects of recombinant
human granulocyte-macrophage colony-stimulating factor in patients with
myelodysplastic syndrome. N. Engl. J. Med., 317:1545-1552, 1987.
183. Vadhan-Raj, S., Buescher, S., Broxmeyer, H. E., et al. Stimulation of
myelopoiesis in patients with aplastic anemia by recombinant human gran
ulocyte-macrophage colony-stimulating factor. N. Engl. J. Med., 319:16281634, 1988.
184. Brandt, S. J., Peters, W. P., Atwater, S. K., et al. Effects of recombinant
human granulocyte-macrophage colony-stimulating factor on hematopoietic
reconstitution after high-dose chemotherapy and autologous bone marrow
transplantation. N. Engl. J. Med., 318:869-876,1988.
185. Gabrilove, J. L., Jakubowski, A., Sher, H., et al. Effects of granulocyte
colony-stimulating factor on neutropenia and associated morbidity due to
chemotherapy for transitional-cell carcinoma. N. Engl. J. Med., 318:14141422, 1988.
186. Morstyn, G., Campbell, L., Souza, L. M., et al. Effects of granulocyte
colony stimulating factor on neutropenia induced by cytotoxic chemother
apy. Lancet, 7:667-671, 1988.
187. Griffin, J. D., Young, D., Herrmann, F., et al. Effects of recombinant
human GM-CSF on proliferation of clonogenic cells in acute myeloblastic
leukemia. Blood, 67:1448-1453, 1986.
188. Waldmann, H., Polliak, A., Hale, G., et al. Elimination of graft-versm-host
disease by in vitro depletion of alloreactive lymphocytes with a monoclonal
rat anti-human lymphocyte antibody (CAMPATH-1). Lancet, 2: 483-486,
1984.
189. Marlin, P. J., Hansen, J. A., Buckner, C. D., et al. Effects of in vitro
depletion of T cells in HLA-identical allogeneic marrow grafts. Blood, 66:
664-672, 1985.
190. Mitsuyasu, R. T., Champlin, R. E., Gale, R. P., et al. Treatment of donor
bone marrow with monoclonal anti-T cell antibody and complement for the
prevention of graft ivrai.vhosi disease. A prospective, randomized, double-
1636
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
blind trial. Ann. Intern. Med., 105: 20-26, 1986.
191. Metcalf, D., Begley, C. G., Johnson, G. R., et al. Biologic properties in vitro
of a recombinant human granulocyte-macrophage colony-stimulating factor.
Blood, 67: 37-45, 1986.
192. Fleischmann, J., Golde, D. W., Weisbart, R. H., and Gasson, J. C. Granulocyte-macrophage colony-stimulating factor enhances phagocytosis of bac
teria by human neutrophils. Blood, 68: 708-711, 1986.
193. Lopez, A. F., Williamson, D. J., Gamble, J. R., et al. Recombinant human
granulocyte-macrophage colony-stimulating factor stimulates in vitro ma
ture human neutrophil and eosinophil function, surface receptor expression,
and survival. J. Clin. Invest., 78: 1220-1228, 1986.
194. Weisbart, R. H., Kwan, L., Golde, D. W., and Gasson, J. C. Human GMCSF primes neutrophils for enhanced oxidative metabolism in response to
the major physiological chemoattractants. Blood, 69:18-21, 1987.
195. Weisbart, R. H., Golde, D. W., Clark, S. C., Wong, G. G., and Gasson, J.
C. Human granulocyte-macrophage colony-stimulating factor is a neutrophil
activator. Nature (Lond.), 314: 361-363, 1985.
196. Vadas, M. A., Nicola, N. A., and Metcalf, D. Activation of antibodydependent cell-mediated cytotoxicity of human neutrophils and eosinophils
by separate colony-stimulating factors. J. Immunol., 130: 795-799, 1983.
197. Fletcher, M. P., and Gasson, J. C. Enhancement of neutrophil function by
granulocyte-macrophage-colony-stimulating
factor involves recruitment of
a less responsive subpopulation. Blood, 71:652-658, 1988.
198. Cannistra, S. A., Bellenga, E., Groshek, P., Rambaldi, A., and Griffin, J.
D. Human granulocyte-monocyte colony-stimulating factor and interleukin3 stimulate monocyte cytotoxicity through a tumor necrosis factor-depend
ent mechanism. Blood, 71: 672-676, 1988.
199. Foon, K. A., and Todd, R. F., III. Immunologie classification of leukemia
and lymphoma. Blood, 68: 1-31, 1986.
200. Schroff, R. W., and Stevenson, H. C. Human immune responses to murine
monoclonal antibodies. In: K. A. Foon and A. C. Morgan (eds.), Monoclonal
Antibody Therapy of Human Cancer, pp. 121-138. The Hague: Martinus
Nijhoff, 1985.
201. Foon, K. A., Schroff, R. W., Bunn, P. A., et al. Effects of monoclonal
antibody therapy in patients with chronic lymphocytic leukemia. Blood, 64:
1085-1094, 1985.
202. Dillman, R. O. Shawler, D. L., Dillman, J. B., and Roystan, I. Therapy of
chronic lymphocytic leukemia and cutaneous T cell lymphoma with T101
monoclonal antibody. J. Clin. Oncol., 2: 881-891, 1984.
203. Schroff, R. W., Morgan, A. C., Woodhouse, C. S., et al. Monoclonal
antibody therapy in malignant melanoma: factors effecting in vivo localiza
tion. J. Biol. Response Modif., 6:457-472, 1987.
204. Schroff, R. W., Foon, K. A., Beatty, S. M., Oldham, R. K., and Morgan,
A. C. Human anti-murine immunoglobulin responses in patients receiving
monoclonal antibody therapy. Cancer Res., 45: 879-885, 1985.
205. Carrasquillo, J. A., Krohn, K. A., Beaumier, P. L., et al. Diagnosis and
therapy of solid tumors with rad iolabeled antibodies and immune fragments.
Cancer Treat. Rep., 68: 317-327, 1984.
206. Sears, H. G., Herlyn, D., Steplewski, Z., and Koprowski, H. Effects of
monoclonal antibody immunotherapy in patients with gastrointestinal adenocarcinoma. J. Biol. Response Modif., 3: 138-150, 1984.
207. Schroff, R. W., Beatty, S. M., Abrams, P. G., et al. Use of an irrelevant
murine monoclonal antibody (MoAb) to reduce antiglobulin responses to a
relevant MoAb. J. NucÃ-.Med., J. NucÃ-.Med., 28: 615, 1987.
208. Khazaeli, M., LoBuglio, A. F., Wheeler, R., Haynes, A., Mischak, R., and
Spitler, L. E. The effects of immunosuppressive regimens on human immune
response to murine monoclonal anti-melanoma antibody ricin A chain.
Proc. Am. Soc. Clin. Oncol., 29:418, 1988.
209. Liu, A. Y., Robinson, R. R., Hellström, K. E., Murray, E. D., Jr., Chang,
C. P., and Hellström, I. Chimeric mouse-human IgGl antibody that can
mediate lysis of cancer cells. Proc. Nati. Acad. Sci. USA, 84: 3439-3443,
1987.
210. Shaw, D. R., Khazaeli, M. B., Sun, L. K., et al. Characterization of a mouse/
human chimeric monoclonal antibody (17-1 A) to a colon cancer tumorassociated antigen. J. Immunol., 138: 4534-4538, 1987.
211. Liu, A. Y., Robinson, R. R., Murray, E. D., Jr., Ledbetter, J. A., Hellström,
I., and Hellström,K. E. Production of a mouse-human chimeric monoclonal
antibody to CD20 with potent Fc-dependent biologic activity. J. Immunol.,
139: 3521-3526, 1987.
212. Press, O. W., Appelbaum, F., Ledbetter, J. A., et al. Monoclonal antibody
l F5 (anti-CD20) serotherapy of human B-cell lymphomas. Blood, 69: 584591, 1987.
213. Dillman RO, Shawler DL, Sobel RE, et al. Murine monoclonal antibody
therapy in two patients with chronic lymphocytic leukemia. Blood, 59:10361045, 1982.
214. Bertram, J. H., Gill, P. S., Levine, A. M., et al. Monoclonal antibody T101
in T cell malignancies: a clinical, pharmacokinetic, and immunologie cor
relation. Blood, 68: 752-761, 1986.
215. Miller, R. A., Oseroff, A. R., Stratte, P. T., and Levy, R. Monoclonal
antibody therapeutic trials in seven patients with T cell lymphoma. Blood,
62:988-995, 1983.
216. Levy, R., and Miller, R. A. Tumor therapy with monoclonal antibodies.
Fed. Proc., 42: 2650-2656, 1983.
217. Ritz, J., Pesando, J. M., Sallan, S. E., et al. Serotherapy of acute lymphoblastic leukemia with monoclonal antibody. Blood, 58: 141-152, 1981.
218. Ball, E. D., Bernier, G. M., Cornwell, G. G., Mclntyre, O. R., O'Donnell,
J. F., and Fanger, M. W. Monoclonal antibodies to myeloid differentiation
219.
220.
221.
222.
223.
224.
225.
226.
227.
228.
229.
230.
231.
232.
233.
234.
235.
236.
237.
238.
239.
240.
241.
242.
243.
244.
245.
246.
247.
antigens: in vivo studies of three patients with acute myelogenous leukemia.
Blood, 62: 1203-1210, 1983.
Oldham, R. K., Foon, K. A., Morgan, A. C., et al. Monoclonal antibody
therapy of malignant melanoma: in vivo localization in cutaneous metastasis
after intravenous administration. J. Clin. Oncol., 2: 1235-1244, 1984.
Waldmann, T. A., Longo, D. L., Leonard, W. J., et al. Interleukin-2 receptor
(Tac antigen) expression in HTLV-I-associated adult T-cell leukemia. Can
cer Res., 45:4559s-4562s, 1985.
Miller, R. A., Maloney, D. G., Warnke, R., and Levy, R. Treatment of a B
cell lymphoma with monoclonal anti-idiotype antibody. N. Engl. J. Med.,
306:517-522,1982.
Meeker, T. C., Lowder, J., Maloney, D. G., et al. The generation of
monocloncal anti-idiotype therapy for B cell malignancy. Blood, 65: 13491363, 1985.
Vadhan-Raj, S., Cordon-Cardo, C., Carswell, E., et al. Phase I trial of a
mouse monoclonal antibody against CD3 ganglioside in patients with mel
anoma: Induction of inflammatory responses at tumor sites. J. Clin. Oncol.,
6: 1636-1648, 1988.
Masui-H., Kawamoto, T., Sato, J-D., Wolf, B., Sato, G., and Mendelsohn,
J. Growth inhibition of human tumor cells in athymic mice by anti-epidermal
growth factor receptor monoclonal antibodies. Cancer Res., 44:1002-1007,
1984.
Trowbridge, I. S. Therapeutic potential of monoclonal antibodies that block
biological function. In: B. D. Boss, R. Langman, I. Trowbridge, and R.
Dulbecco (eds.). Monoclonal Antibodies and Cancer, pp. 53-61. New York:
Academic Press, 1983.
Jerne, N. K. Towards a network theory of the immune system. Ann.
Immunol. (Paris), 125C: 373-389, 1974.
Meeker, T., Lowder, J., Cleary, M. L., et al. Emergence of idiotype variants
during treatment of B-cell lymphoma with anti-idiotype antibodies. N. Engl.
J. Med., 312: 1658-1665, 1985.
Weiner, L. M., Steplewski, Z., Koprowski, H., Litwin, S., and Comis, R.
L. Divergent dose-related effects of 7-interferon therapy on in vitro antibodydependent cellular cytotoxicity by human peripheral blood monocytes. Can
cer Res., 48: 1042-1046, 1988.
Munn, D. H., and Cheung, N-K. V. Interleukin-2 enhancement of mono
clonal antibody-mediated cellular cytotoxicity against human melanoma.
Cancer Res., 47:6600-6605, 1987.
Basham, T. Y., Kaminski, M., Kitamura, K., Levy, R., and Merigan, T.
Synergistic antitumor effect of interferon and anti-idiotype monoclonal
antibody in murine lymphoma. J. Immunol., 137: 3019-3024, 1986.
Berinstein, N., and Levy, R. Treatment of a murine B cell lymphoma with
monoclonal antibodies and IL-2. J. Immunol., 139:972-976, 1987.
Himmelweit, B. (ed.). The Collected Papers of Paul Ehrlich. Elmsford, NY:
Pergamon Press, 1975.
Dillman, R. O., Johnson, D. E., and Shawler, D. L. Comparisons of drugs
and toxin immunoconjugates. Antibody, Immunoconjugates Radiopharm.,
/: 65-77, 1988.
Vitella, E. S., and Uhr, J. W. Immunotoxin. Annu. Rev. Immunol., 3:197212, 1985.
Paslan, I., Willingham, M. C., and FitzGerald, D. J. P. Immunotoxins.
Cell., 47:641-648, 1986.
Blakey, D. C., and Thorpe, D. C. An overview of therapy with immunoloxins
conlaining ricin or ils A chain. Anlibody, Immunoconjugales, Radiopharm.,
/: 1-16, 1988.
Olsnes, S., and Pihl, A. Chimeric toxins. Pharmacol. Then, 75: 355-381,
1982.
Laurenl, G., Pris, J., and Parcel, J-P. Effecls of therapy with T101 ricin Achain immunotoxin in iwo leukemia palienls. Blood, 67: 1680-1687, 1986.
Spitler, L., del Rio, M., Khenligan, A., et al. Therapy of palienls wilh
malignanl melanoma using a monoclonal anlimelanoma anlibody ricin A
chain immunoloxin. Cancer Res., 47: 1717-1723, 1987.
Pielersz, G. A., Smylh, M. J., Kanells, J., Cunningham, Z., Sacks, N. P.
M., and McKenzie, I. F. C. Preclinical and clinical sludies wilh a variely of
immunoconjugales. Antibody, Immunoconjugates Radiopharm., /: 79-103,
1988.
Weinslein, J. N., and Leserman, L. D. Liposomes as drug carriers in cancer
chemolherapy. Pharmacol. Ther., 24: 207-233, 1984.
Martin, F. J., and Papahadjopoulos, D. Irreversible coupling of immuno
globulin fragments to preformed vesicles. J. Biol. Chem., 257: 286-288,
1982.
Matthay, K. K., Healh, T. D., Badger, C. C., Bernstein, I. D., and Papahad
jopoulos, D. Antibody-directed liposomes: comparison of various ligands
for associalion, endocylosis, and drug delivery. Cancer Res., 46:4904-4910,
1986.
Berinslein, N., Mallhay, K. K., Papahadjopoulos, D., Levy, R., and Sikie,
B. I. Anlibody-directed largeling of liposomes to human cell lines: role of
binding and inlernalizalion on growlh inhibilion. Cancer Res., 47: 59545959, 1987.
Halpern, S. E., and Dillman, R. O. Problems associaled wilh radioimmunodetection and possibilities for future solution. J. Biol. Response Modif.,
6:235-262, 1987.
Abrams, P. G., Carrasquillo, J. A., Schroff, R. W., et al. Imaging and
Iherapy of melaslatic carcinoma with radiolabeled monoclonal antibodies.
In: R. K. Oldham (ed.), Principles of Cancer Biolherapy, pp. 337-354. New
York: Raven Press, 1987.
Mach, J. P., Bucheggar, F., Forni, M., et al. Use of radiolabeled monoclonal
anli-CEA anlibodies for deleclion of human carcinomas by external pholo-
1637
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
248.
249.
250.
251.
252.
253.
254.
255.
256.
257.
258.
259.
260.
261.
262.
263.
264.
265.
scanning and tomoscintigraphy. Immunol. Today, 2: 239-249, 1981.
Epenetos, A. A., Mather, S., Granowska, M., et al. Targeting of iodine-123labeled tumor-associated monoclonal antibodies to ovarian, breast and gas
trointestinal tumors. Lancet, 2:999-1004, 1982.
Larson, S. M., Carrasquillo, J. A., Krohn, K. A., et al. Localization of I3IIlabeled p97 specific Fab fragments in human melanomas as a basis for
radiotherapy. J. Clin. Invest., 72: 2101 -2114, 1983.
Carrasquillo, J. A., Bunn, P. A., Jr., Keenan, A. M., et al. Radioimmunodetection of cutaneous T-cell lymphoma with ' "In-labeled T101 monoclonal
antibody. N. Engl. J. Med., 315: 673-679, 1985.
Carrasquillo, J. A., Abrams, P. G., Schroff, R. W., et al. Effect of '"In9.2.27 monoclonal antibody dose on the imaging of metastatic melanoma.
J. NucÃ-.Med., 29: 37-47, 1988.
Murray, J. L., Rosenblum, M. G., Lamki, L., et al. Clinical parameters
related to optimal tumor localization of indium-111-labeled mouse antimelanoma monoclonal antibody ZME-018. J. NucÃ-.Med., 28:25-33,1987.
Schroff, R. W., Farrell, M. M., Klein, R. A., Oldham, R. K., and Foon, K.
A. T65 antigen modulation in a phase I monoclonal antibody trial with
chronic lymphocytic leukemia patients. J. Immunol., 133:1641-1648,1984.
Rodwell, J. D., Alvarez, V. L., Lee, C, et al. Site-specific covalent modification of monoclonal antibodies. In vitro and in vivo evaluations. Proc. Nati.
Acad. Sci. USA, 83: 2632-2636, 1986.
Keenan, A. M., Weinstein, J. N., Carrasquillo, J., et al. Immunolymphoscintigraphy and the dose dependence of "'In-labeled T101 monoclonal
antibody in patients with cutaneous T-cell lymphoma. Cancer Res., 47:
6093-6099, 1987.
Fritzberg, A. R., Abrams, P. G., Beaumier, P. L., et al. Specific and stable
labeling of antibodies with technitium-99m with a diumide dithiolate chelating agent. Proc. Nati. Acad. Sci. (USA), 85:4025-4029, 1988.
Feun, L., Kotler, J., Serafini, A., et al. Anti-melanoma Te 99m FAB
antibody for imaging metastatic melanoma (MM). Proc. Am. Soc. Clin.
Oncol., 7: 249, 1988.
Order, S. E., Stillwagon, G. B., Klein, J. L., et al. Iodine-131-antiferritin, a
new treatment modality in hepatomas: a radiation therapy oncology group
study. J. Clin. Oncol., 3: 1573-1582, 1985.
Lenhard, R. E., Order, S. E., Spunberg, J. J., Asbell, S. O., and Leibel, D.
A. Isotopie immunoglobulin: a new systemic therapy for advanced Hodgkin's disease. J. Clin. Oncol., 3: 1296-1300, 1985.
DeNardo, S. J., O'Grady, L. F., DeNardo, G. L., and Mills, S. L. Radioimmunotherapy of lymphoproliferative disease. Blood, 72 (Suppl. 1): 241 a,
1988.
Rosen, S., Zimmer, A. M., Goldman-Neiken, R., et al. Radioimmunodetection and radioimmunotherapy of cutaneous T-cell lymphomas using an '"Ilabeled monoclonal antibody: an Illinois Cancer Council Study. J. Clin.
Oncol., 5: 562-573, 1987.
Press, O., Badger, C., Eary, J., et al. Radioimmunotherapy of refractory
human malignant B cell lymphomas. Blood, 70 (Suppl. 1): 248a, 1988.
Epenetos, A. A., Munro, A. J., Stewart, S., et al. Antibody-guided irradiation
of advanced ovarian cancer with intraperitoneally administered radiolabeled
monoclonal antibodies. J. Clin. Oncol., 5: 1890-1899, 1987.
Badger, C. C, Krohn, K. A., Peterson, A. V., Shulman, H-, and Bernstein,
I. D. Experimental radiotherapy of murine lymphoma with '31I-labeled antiThy 1.1 monoclonal antibody. Cancer Res., 45: 1536-1544,1985.
Takvorian, T., Canellos, G. P., Ritz, J., et al. Prolonged disease-free survival
after autologous bone marrow transplantation in patients with non-Hodgkin's lymphoma with a poor prognosis. N. Engl. J. Med., 316: 1499-1505,
1987.
266. Ritz, J., Bast, R. C., Clavell, L. A., et al. Autologous bone marrow trans
plantation in CALLA-positive acute lymphoblastic leukemia after in vivo
treatment with .15 monoclonal antibody and complement. Lancet, 2:60-63,
1982.
267. Ramsay, N., LeBien, T., Nesbit, M., et al. Autologous bone marrow trans
plantation for patients with acute lymphoblastic leukemia after in vivo
treatment with monoclonal antibodies BA-1, BA-2, and BA-3 plus comple
ment. Blood, 66: 508-513, 1985.
268. Medical Research Council. Treatment of acute lymphoblastic leukaemia.
Comparison of immunotherapy (BCG), intermittent methotrexate, or no
therapy after a five-month intensive cytotoxic regimen (Concord trial). Br.
Med. J., 4: 189-194, 1971.
269. Heyn, R. M., Joo, P., Karon, M., et al. B.C.G. in the treatment of acute
lymphoblastic leukaemia. Blood, 46:431-442, 1975.
270. Zuhrie, S. R., Harris, R., Freeman, C. B., et al. Immunotherapy alone vs.
no maintenance treatment in acute myclogenous leukemia. Br. J. Cancer,
41: 372-377, 1980.
271. Powles, R. L., Rüssel,J., Lister, T. A. Immunotherapy for acute myelogenous leukemia: A controlled clinical study 2'h years after entry of the last
patient. Br. J. Cancer, 35: 265-272, 1977.
272. Holland, J. R., and Bekasi, J. G. Comparison of chemotherapy with chemo
therapy plus VCN-treated cells in acute myelocytic leukemia. In: W. D.
Terry, and D. Windhorst (eds.), Immunotherapy of Cancer: Present Status
of Trials in Man. pp. 353-374. New York: Raven Press, 1978.
273. Omura, G. A., Vogler, W. R., Lefante, J., et al. Treatment of acute
myelogenous leukemia: Influence of three induction regimens and mainte
nance with chemotherapy or BCG immunotherapy. Cancer, 49:1530-1536,
1982.
274. Berd, D., and Mastrangelo, M. J. Effect of low dose cyclophosphamide on
the immune system of cancer patients: depletion of CD4+, 2H4+ suppressor-inducer T-cells. Cancer Res., 48: 1671-1675, 1988.
275. Brystryn, J. C., Oratz, R., Harris, M. N., Roses, D. F., Colomb, F. M., and
Speyer, J. L. Immunogenicity of a polyvalent melanoma antigen vaccine in
humans. Cancer (Phila.), 61: 1065-1070, 1988.
276. Wallack, N. K., Bash, J. A., Leftheriotis, E., et al. Positive relationship of
clinical and serologie responses to vaccinia melanoma oncolysate. Arch.
Surg., 122: 1460-1463, 1987.
277. McCune, C. S., Henshaw, E. C., Marquis, D. M., Sahasrabudhe, D., Leary,
J., and O'Donnell, R. W. Human hybrid tumor cells: observations on their
production and clinical effects. J. Biol. Response Modif., 6:130-140,1987.
278. Berd, D., Maguire, H. C., Jr., and Mastrangelo, M. J. Induction of cellmediated immunity to autologous melanoma cells and regression of métas
tases after treatment with a melanoma cell vaccine preceded by cyclophos
phamide. Cancer Res., 46: 2572-2577, 1986.
279. Livingston, P. O., Kaelin, K., Pinsky, C. M., Oettgen, H. F., and Old, L. J.
The serologie response of patients with stage II melanoma to allogeneic
melanoma cell vaccines. Cancer (Phila.), 56: 2194-2200, 1985.
280. Tai, T., CalÃ-an,L. D., Tsuchida, T., Saxton, R. E., Irie, R. F., and Morton,
D. L. Immunosensitivity of melanoma-associated gangliosides in cancer
patients. Int. J. Cancer, 35:607-612, 1985.
281. Hoover, H. C., Jr., Surdyke, M., Dangel, R. B., Peters, L. C., and Hanna,
M. G., Jr. Delayed cutaneous hypersensitivity to autologous tumor cells in
colorectal cancer patients immunized with an autologous tumor cell: Bacillus
Calmette-Guérinvaccine. Cancer Res., 44:1671-1676, 1984.
282. Hoover, H. C., Jr., Surdyke, M. G., Dangel, R. B., Peters, L. C., and Hanna,
M. G., Jr. Prospectively randomized trial of adjuvant active-specific im
munotherapy for human colorectal cancer. Cancer (Phila.), 55:1236-1243,
1985.
283. McCune, C. S., Schapira, D. V., and Henshaw, E. C. Specific immunother
apy of advanced renal carcinoma. Evidence for the polyclonality of metas
tasis. Cancer (Phila.), 47:1984-1987, 1981.
284. Hollinshead, A., Stewart, G. H. M., Takita, H., Dalbow, M., and Concannon, J. Adjuvant specific active lung cancer immunotherapy trials. Tumorassociated antigens. Cancer (Phila.), 60:1249-1262, 1987.
285. Haubeck, H. D., and KölschE. Tumor-specific T suppressor cells induced
at early stage of tumorigenesis act on the induction phase of cytotoxic T
cells. Immunology, 47: 503-510, 1982.
286. Howie, S. M., and McBride, W. H. Tumor specific T helper activity can be
abrogated by two distinct suppressor cell mechanisms, tur. J. Immunol.,
72:671-675,1982.
287. McBride, W. H., and Howie, S. M. Induction of tolerance to a murine
fibrosarcoma in two zones of dosage-the involvement of suppressor cells.
Br. J. Cancer, 53: 707-711, 1986.
288. Bona, C. A., and Kohler, H. Anti-idiotypic antibodies and internal images.
In: J. C. Venter, C. M. Fraser, and J. Lindstrom (eds.), Probes for Receptor
Structure and Function, Vol. 4, pp. 141-150. New York: Alan R. Liss, Inc.,
1984.
289. Kohler, H., Muller, S., and Bona, C. Internal antigen and immune network.
Proc. Soc. Exp. Biol. Med., 178: 189-195, 1985.
290. Jerne, N. K. Idiotypic networks and other preconceived ideas. Immunol.
Rev., 79:5, 1984.
291. Kennedy, R. C., Zhou, E-M., Lanford, R. E., Chanh, T. C., and Bona, C.
A. Possible role of anti-idiotypic antibodies in the induction of tumor
immunity. J. Clin. Invest, 80:1217-1224,1987.
292. Lindemann, J. Speculations on idiotypes and homebodies. Ann. Immunol.
(Paris), I24C: 171, 1973.
293. Kohler, H. The immune network revisited. In: H. Kohler, J. Urgain, and P.
Cazenave (eds.), Idiotypes in Biology and Medicine, pp. 13-28. New York:
Academic Press, 1985.
294. Nepon, G. T., Nelson, K. A., Holbeck, S. L., Hellström,L, and Hellström,
K. E. Induction of immunity to a human tumor marker by in vivo adminis
tration of anti-idiotypic antibodies in mice. Proc. Nati. Acad. Sci. USA, 81:
2864-2867,1985.
295. Gorczynski, R. M., Kennedy, M., Polidoulis, I., and Price, G. B. Altered
tumor growth in vivo after immunization of mice with antitumor antibodies.
Cancer Res., 44: 3291-3298, 1984.
296. Dunn, P. L., Johnson, C. A., Styles, J. M., Pease, S. S., and Dean, C. J.
Vaccination with syngeneic monoclonal anti-idiotype protects against a
tumour challenge. Immunology, 60: 181-186, 1987.
297. Herlyn, D., Ross, A. H., and Koprowski, H. Anti-idiotypic antibodies bear
the internal image of a human tumor antigen. Science (Wash. DC), 232:
100-102, 1986.
298. Bhattacharya-Chatterjee, M., Pride, M. W., Seon, B. K., and Kohler, H.
Idiotype vaccines against human T cell acute lymphoblastic leukemia. I.
Generation and characterization of biologically active monoclonal amiidiotopes. J. Immunol., 139: 1354-1360, 1987.
299. Bhattachayra-Chatterjee, M., Chatterjee, S. K., Vasile, S., Seon, B. K.,
Kohler, H. Idiotype vaccines against human T cell leukemia, II. Generation
and characterization of a monoclonal idiotype cascade (Abl, Ab2, and Ab3).
J. Immunol., 141:1398-1403, 1988.
300. Koprowski, H., Herlyn, D., Lübeck,M., DeFreitas, E., and Sears, H. F.
Human anti-idiotype antibodies in cancer patients: is the modulation of the
immune response beneficial for the patient? Proc. Nati. Acad. Sci. USA,
«7:216-219, 1984.
301. Herlyn, D., Wettendorff, M., Iliopoulos, D., Schmoll, E., Schede!, I., and
Koprowski, H. Immunotherapy of colorectal cancer with anti-idiotypic
antibodies. Proc. Am. Assoc. Cancer Res., 2: 408, 1988.
302. Mittelman, A., Kageshita, T., Kusama, K., Kim, J. W., Arlin, Z., and
Ferrone, S. A clinical trial of murine antiidiotype monoclonal antibodies to
1638
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
BIOLOGICAL RESPONSE MODIFIERS
303.
304.
305.
306.
307.
308.
309.
310.
311.
312.
high molecular weight melanoma associated antigens. Proc. Am. Soc. Clin.
Oncol., 7:248, 1988.
Livingston, P. ( ).. Cunningham-Rundles, S., Marfleet, G., et al. Inhibition
of suppressor-cell activity by cyclophosphamide in patients with malignant
melanoma. J. Biol. Response Modif., 6: 392-403, 1987.
Periti, P., and Mini, E. Immunomodulation by cancer chemotherapeutic
agents. Chemotherapia, 6: 399-402, 1987.
Fidler, J. M., DeJoy, S. Q., and Gibbons, J. J., Jr. Selective immunomodulation by the antineoplastic agent mitoxantrone. I. Suppression of B
lymphocyte function. J. Immunol., 137: 727-732, 1986.
Ehrke, M. J., Tomazic, V., Ryoyama, K., Cohen, S. A., Mil.¡eli,E. Adriamycin induced immunomodulation: dependence upon time of administra
tion. Int. J. Immunopharmacol., 5: 43-48, 1983.
Ackerman, M. F., Mark, R., Chakraborty, P. R., and Moraban, P. S. Effects
of diethylstilbestrol on Propionibacterium acnes immunomodulation: inhi
bition of macrophage activation and antitumor activity. J. Leukocyte Biol.,
40: 549-559, 1986.
Nagy, E., and Berczi, I. Immunomodulation by tamoxifen and persolide.
Immunopharmacology, 12: 145-153, 1986.
Kopp, W. C, Dierks, S. E., Butler, J. E., Upadrashta, B. S., and Richerson,
H. B. Cyclosporine immunomodulation in a rabbit model of chronic hypersensitivity pneumonitis. Am. Rev. Respir. Dis., 132:1027-1033, 1985.
Kobayashi, K., Abe, C., lizuka, Y.. and Shiokawa, Y. Immunomodulation
by RS 2131. a new non-steroidal antiinflammatory drug. Immunopharma
cology, 12: 213-220, 1986.
Yahya, M. 1>., Watson, R. R. Immunomodulation by morphine and mari
juana. Life Sci., 41: 2503-2510, 1987.
Roszkowski, W., Ko, H. L., Roszkowski, K., Jeljaszewicz, J., and Pulverer,
G. Antibiotics and immunomodulations: effects of cefotaxime, amikacin,
313.
314.
315.
316.
317.
318.
319.
320.
321.
mezlocillin, piperacillin and clindamycin. Med. Microbiol. Immunol., 173:
279-289, 1985.
Hilsers, L. A., Snippe, H., Jansze, M., and Willers, J. M. Route-dependent
immunomodulation: local stimulation by a surfactant and systemic stimu
lation by a polyanion. Int. Arch. Allergy Appi. Immunol., 79: 388-391,
1986.
Talmadge, J. E., Uithoven, K. A., Lenz, B. F., and Chingos, M. Immuno
modulation and therapeutic characterization of thymosin fraction five. Can
cer Immunol. Immunother., 18: 185-194, 1984.
Messerschmidt, G. L., Henry, D. H., Snyder, W. H., Jr., et al. Protein A
immunoadsorption in the treatment of malignant disease. J. Clin. Oncol.,
6:203-212, 1988.
Black, W. J., Muñoz,J. J., Peacock, M. G., et al. ADP-ribosyltransferase
activity of pertussis toxin and immunomodulation by Bordetella pertussis.
Science (Wash. DC), 240:656-659, 1988.
Fuster, M. J., and Lagrange, P. H. Immunomodulation with P40, an
insoluble delipidated fraction of Corynebacterium granulosum. I. Immune
response to sheep red blood cells. Ann. Immunol., 133: 253-267, 1982.
Galsworthy, S. B. Immunomodulation by surface components of Listeria
monocytogenes: a review. Clin. Invest. Med., 7: 223-227, 1984.
Sriram, S., Carroll, L., Fortin, S., Cooper, S., Ranses, G. in vivo immuno
modulation by monoclonal anti-CD4 antibody. II. Effect of T cell response
to nuclin basic protein and experimental allergic encephalomyelitis. J.
Immunol., 141: 464-468, 1988.
Ranses, G. E., Cooper, S. M., and Sriram, S. In vivo immunomodulation
by monoclonal anti-1.3 I 4. 1. Effects on humoral and cell-mediated immune
response. Cell. Immunol., 106: 163-173, 1987.
Oldham, R. Biotherapy: The 4th Modality of Cancer Treatment. J. Cell.
Physiol. (Suppl.), 4: 91-99, 1986.
1639
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.
Biological Response Modifiers: The New Immunotherapy
Kenneth A. Foon
Cancer Res 1989;49:1621-1639.
Updated version
E-mail alerts
Reprints and
Subscriptions
Permissions
Access the most recent version of this article at:
http://cancerres.aacrjournals.org/content/49/7/1621.citation
Sign up to receive free email-alerts related to this article or journal.
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Department at [email protected].
To request permission to re-use all or part of this article, contact the AACR Publications
Department at [email protected].
Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1989 American Association for Cancer Research.