Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
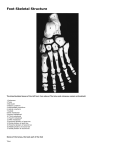
Metatarsalgia Background Metatarsalgia is a common overuse injury. The term describes pain and inflammation in the ball of the foot. It is often thought of as a symptom of other conditions, rather than as a specific disease. The classic symptom is pain in the front (ball) of the foot. Many people say that it is "like walking on pebbles," but x-rays usually show nothing irregular. The problem affects males and females from adolescents to older adults. It is most common in middle-aged women. Cause Metatarsalgia is caused by the compression of a small toe nerve between two displaced metatarsal bones. Inflammation occurs when the head of one displaced metatarsal bone presses against another and they catch the nerve between them. With every step, the nerve is pushed together by the bones and then rubbed, pressed again, and irritated without relief. Consequently, the surrounding nerve tissue becomes enlarged, with a sheath of scar tissue that forms to protect the nerve fibers. You may experience metatarsalgia if you're physically active and you participate in activities that involve running and jumping. Or, you may develop metatarsalgia by wearing ill-fitting shoes. There are other causes as well. Although generally not serious, metatarsalgia can sideline you. Fortunately, conservative treatments, can often relieve metatarsalgia symptoms. Symptoms The primary symptom of metatarsalgia is pain at the end of one or more of the metatarsal bones. Most often, the pain comes on gradually, for example over a period of several months, rather than suddenly. A condition known as Morton's neuroma (interdigital neuroma) produces symptoms of metatarsalgia due to irritation and inflammation of nerves. People with Morton's neuroma may experience toe numbness in addition to pain in the forefoot. Symptoms of metatarsalgia may include: Sharp, aching or burning pain in the ball of your foot — the part of the sole just behind your toes Pain in the area around your second, third or fourth toes — or, only near your big toe Pain that gets worse when you stand, walk or run and improves when you rest Sharp or shooting pain in your toes Numbness or tingling in your toes Pain that worsens when you flex your feet A feeling in your feet as if you're walking with a pebble in your shoe Increased pain when you're walking barefoot, especially on a hard surface When to see a doctor Not all foot problems need medical care. Sometimes your feet simply ache after a long day of standing or a punishing workout. But it's best not to ignore any foot pain that lasts more than a few days. Talk to your doctor if you experience a burning pain in the ball of your foot that doesn't improve after changing your shoes and modifying your activities. Causes In each foot, five metatarsal bones run from your arch to your toe joints. The first metatarsal is shorter and thicker than the other four bones, which are usually similar in size. During the push-off phase when you walk, jump or run, your body weight is transferred to your toes and metatarsals. The first and second metatarsal bones take the brunt of this force. Most metatarsal problems develop when something changes in the way your foot normally works (mechanics), affecting how your weight is distributed. This can put excess pressure on the metatarsals, leading to inflammation and pain, especially in the metatarsal heads — the rounded ends of the bones that connect with your toe bones. Sometimes a single factor can lead to metatarsalgia. More often, several factors are involved, including: Intense training or activity. Runners are at risk of metatarsalgia, primarily because the front of your foot absorbs significant force when you run. But anyone who participates in a high-impact sport is also at risk, especially if your shoes are ill-fitting or are worn out. Certain foot shapes. A high arch can put extra pressure on the metatarsals. So can having a second toe that's longer than the big toe, which causes more weight than normal to be shifted to the second metatarsal head. Hammertoe. This foot problem can develop when high heels or too-small shoes prevent your toes from lying flat. As a result, one of your toes — usually the second — curls downward because of a bend in the middle toe joint. This contraction depresses the metatarsal heads. Bunion. This is a swollen, painful bump at the base of your big toe. Sometimes the tendency to develop bunions is inherited, but the problem can also result from wearing high heels or too-small shoes. Bunions are much more common in women than in men. A bunion can weaken your big toe, putting extra stress on the ball of your foot. Surgery to correct a bunion can also lead to metatarsalgia if you don't rest long enough for your foot to heal completely. Excess weight. Because most of your body weight transfers to your forefoot when you move, extra pounds mean more pressure on your metatarsals. Losing weight may reduce or eliminate symptoms of metatarsalgia. Poorly fitting shoes. High heels, which transfer extra weight to the front of your foot, are a common cause of metatarsalgia in women. Shoes with a narrow toe box or athletic shoes that lack support and padding also can contribute to metatarsal problems. Stress fractures. Small breaks in the metatarsals or toe bones can be painful and change the way you put weight on your foot. Morton's neuroma. This noncancerous growth of fibrous tissue around a nerve usually occurs between the third and fourth metatarsal heads. It causes symptoms that are similar to metatarsalgia and can also contribute to metatarsal stress. Morton's neuroma frequently results from wearing high heels or too-tight shoes that put pressure on your toes. It can also develop after high-impact activities such as jogging and aerobics. Treatment Removing the callus is not advised because the callus is a response to pressure and is not the primary disease. If symptoms are acute with a short duration, abnormal pronation of the subtalar joint in the ankle can be the primary cause. The doctor may recommend using orthotic devices in these cases. Chronic symptoms respond better to a metatarsal bar that can be added to the running or athletic shoe. Individuals with a high arch who experience pain from metatarsalgia respond well to an orthotic device that provides total contact to the medial longitudinal arch because preventing collapse of the arch reduces the stress on the metatarsal heads. Patients with a Morton toe respond well to a rigid orthotic with an extension underneath the first metatarsal bone. Foot freedom: If you wear tight shoes with thin soles and high heels, give them away. If you have symptoms of a Morton's neuroma, remove the shoes periodically and gently massage the painful area. If you pinch or rub vigorously, you may experience pain as intense as when you hit your "funny bone." Orthotics (or metatarsal pads): As inflammation subsides, an orthotic device often is the only intervention required to maintain normal mechanical function. These devices are necessary to distribute force away from the site of injury. Patients should continue self-mobilization exercises, including long-axis distraction and dorsal/plantar glides as directed by the practitioner. Consult your Orthotist for a footpad that relieves pressure on the metatarsal area. Medications: Your doctor may prescribe nonsteroidal anti-inflammatory medication, this is the most common treatment. Ibuprofen, or diclofenac sodium, prescription astringents, emollients or ointments can help treat bunions or calluses, which sometimes are associated with metatarsalgia. Rarely, injections of a corticosteroid into the tender area may be used. Surgery: An operation seldom is necessary. In severe cases of Morton's neuroma, surgeons remove the nerve associated with painful symptoms. Surgical options for other types of metatarsalgia include reshaping joints and modifying irregularly shaped bones Physical Therapy: The primary focus of treatment is restoration of normal biomechanics and relief of pressure in the symptomatic area. Therapy needs to allow the inflammation to subside or resolve by relieving the repeated excessive pressure. Passive range of motion exercises will progress to active exercises as the inflammation resolves. Therapy to increase range of motion allows improved forward progression of the tibia over the foot with reduced stress on the forefoot. Strengthening the toe flexor muscles may allow for greater weight-bearing capacity on the toes. Recreational Therapy: Alternate forms of conditioning and training during healing should be encouraged. For example, swimming is an excellent exercise for maintaining physical conditioning while the patient is in a restricted weight-bearing phase of healing. Prognosis Prognosis generally is good, with the treatment described in the Treatment section. Resources http://www.webmd.com/a-to-z-guides/metatarsalgia http://www.mayoclinic.com/health/metatarsalgia www.webmd.com/a-to-z-guides/metatarsalgia