Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
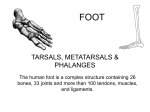
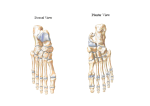
Chapter 18: The Foot Foot Anatomy: Bones Toes – Phalanges – Sesamoid Bones Metatarsals Tarsal Bones – – – – – Calcaneus Talus Navicular Cuboid Cuneiforms Foot Anatomy: Arches Anterior Metatarsal Arch – Shaped by heads of 1st-5th metatarsals Transverse Arch – Primarily cuboid & internal cuneiform Medial Longitudinal Arch – Calcaneus, talus, navicular, 1st cunieform, & 1st metatarsal – Calcaneonavicular Ligament Lateral Longitudinal Arch – Calcaneus, cuboid, & 5th metatarsal Foot Anatomy: Plantar Fascia Fibrous connective tissue Originates at medial tuberosity of calcaneus Inserts at proximal heads of metatarsals Supports foot against downward forces Foot Anatomy: Articulations Interphalangeal Joints Metatarsophalangeal Joints Intermetatarsal Joints Tarsometatarsal Joints Intertarsal Joints Subtalar Joint – Articulation between talus in calcaneous – Inversion, eversion, pronation, & supination Midtarsal Joint – Consists of two joints: Calcaneocuboid and Talonavicular – Directly related to position of subtalar joint Movements Dorsiflexion Plantar Flexion Inversion Eversion Adduction Abduction Supination Pronation Flexion Extension Intrinsic Muscles of Foot Extensor Digitorum Brevis Abductor Hallucis Flexor Digitorum Brevis Abductor Digiti Minimi Quadratus Plantae Lumbricales Flexor Hallucis Brevis Adductor Hallucis Flexor Digit Minimi Brevis Plantar Interossei Dorsal Interossei Muscle & Action Extensor Digitorum brevis (dorsal muscle) – extends the 2nd-5th toes Abductor Hallicus – abducts the great toe Flexor Digitorum Brevis – flexes the 2nd-5th toes Abductor Digiti Minimi – abducts the small toe 8 Muscles & Actions Quadratus Plantae – Aids in flexing the 2nd-5th toes Lumbricles – flexes the 2nd-5th toes Flexor Hallucis Brevis – flexes the great toe Adductor Hallicus – adducts the great toe 9 Muscles & Actions Flexor Digiti Minimi Brevis – flexes the small toe Plantar interossei – adducts the toes toward the 2nd toe Dorsal interossei – Abducts the toes from the 2nd toe; moves the 2nd toe medially and laterally 10 Nerve & Blood Supply Nerve Supply – Tibial Nerve Posterior Leg & Plantar aspects of foot – Common Peroneal Nerve Anterior Leg & Foot Blood Supply – Anterior & Posterior Tibial Arteries Gait Stance Phase – Initial contact to toe-off – Five periods Initial Contact Loading Response Mid Stance Terminal Stance Pre-Swing (Toe Off) Swing Phase – Period of non-weight bearing – Three periods Initial Swing Mid Swing Terminal Swing Prevention of Foot Injuries Selecting Appropriate Footwear Using a Shoe Orthotic Foot Hygiene Foot Assessment History – What? When? How? Previous hx? Observation – Symptoms – Structural Deformities – Shoe Wear Patterns Palpation – Bony Palpations – Soft-Tissue Palpation – Pulses Range of Motion – AROM (athlete performs ROM) – PROM (ATC performs ROM) – RROM (Adds resistance) Special Tests – Tinel’s Sign – Morton’s Tests - Squeeze Test – Fracture Tests (Bump Test) – Neurological Assessment Special Tests Morton’s test (Neuroma) – Put the foot in a supine position – Apply tranverse pressure to the – heads of the metatarsals – + test is a sharp p! in the forefoot 15 Special Tests Tinel’s Sign – Tapping over the posterior tibial nerve – Produces tingling distal to that area – + sign numbness, tingling, and paresthesia (prickling sensation) – Indicates possible tarsal tunnel syndrome 16 Recognition Of Injuries Fractures – – – – Talus Calcaneus Phalanges 5th Metatarsal Jones Fx – 1st or 2nd Metatarsal March Fx – Tarsometatarsal Lisfranc Injury Bursitis – Retrocalcaneal Apophysitis – Calcaneus (Sever’s Disease) Morton’s Neuroma Contusions – Heel – “Bone Bruise” Subluxation/Dislocations – – Cuboid Phalanges Arches – – – – – Pes Planus Pes Cavus Longitudinal Strain Metatarsal Strain Plantar Fascitis Bunions – Hallux Valgus Inflammation – Sesamoiditis Toes – – – – – Sprains Turf Toe Hammer, Mallet, or Claw Overlapping Subungual Hematoma Injuries Fractures of the Talus – Etiology: occurs laterally from a severe IV & DF force or medially from an IV and PF force – Treatment X-ray for accurate diagnosis, immobilization – S&S hx of repeated trauma to the ankle p! on weight bearing, complains of catching and snapping intermittent swelling 18 talar dome is tender on palpation Injuries Fracture of the Calcaneus – Etiology occurs from landing after a jump or fall from a height – S&S immediate swelling and p! can not bear weight – Management RICE immediately X-rays Immobilize 19 Injuries Sever’s Disease – Etiology occurs in young, physically active patients injury at the apophysis (bone protrusion) of the calcaneus where the Achilles tendon attaches – S&S p! occurs at the posterior heel p! occurs during vigorous activity – Management Rest, Ice, stretching the Achilles tendon Anti-inflammatory medications (IBU, Advil) 20 Injuries Tarsal Tunnel Syndrome – Etiology tarsal tunnel is behind the medial malleolus tibialis posterior, flexor hallucis & flexor digitorum pass through this tunnel. Any trauma to this area can compromise these structures – S&S p! and paesthsia along the medial & plantar aspect + Tinel’s sign – Management anti-inflammatory medication, orthotics, surgery 21 Injuries Pes Planus Foot (Flatfoot) – Etiology medial longitudinal arch appears to be flat/fallen repeated pounding – S&S P! or fatigue in the medial longitudinal arch – Management no p!=no treatment P!= orthotic 22 Injuries 2nd Metatarsal Stress Fracture (Morton’s Toe) – Etiology the 1st metatarsal is longer than the 2nd – S&S p! both during & after activity point tenderness – Management no symptoms= no correction medial wedge orthotic 23 Injuries Plantar Fascitis – Etiology can occur in patients with pes cavus or pes planus – S&S p! in the anterior medial heel p! is increased when the patient bears weight in the morning or after sitting for long periods of time p! in dorsiflexion – Management Orthotic Arch taping and stretching the plantar fascia 24 Foot Rehabilitation General Body Conditioning Weight Bearing – Progress from NWB to WB – Correct Gait Joint Mobilization – Anterior/Posterior Glides Flexibility – Triceps Surae & Plantar Fascia Muscular Strength – Exercises? Neuromuscular Control – Proprioception Exercises – Closed Kinetic Chain Foot Orthotics & Taping