Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
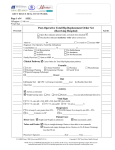
ADDRESSOGRAPH GREY BRUCE HEALTH NETWORK Page 1 of 2 SITE: __________________ Allergies: □ NKA or: __________________________ Weight (kg) _____________ Height (cm) ______________ Radical Prostatectomy Post-Operative Order Set ______ Admission Diagnosis: Post-Operative Radical Prostatectomy IN PACU: ______ CBC with diff, Electrolytes, Creatinine Diet On Admission: ______ Sips to Clear Fluids OR Energy controlled Clear Fluids When passing flatus: ______ Regular Diet OR ______ Activity as tolerated Energy controlled Diet Activity Out of bed day of surgery Ambulate TID Post-Op Day 1 Vital Signs ______ VS + O2 sats Q4H x 24 hours, QID x 24 hours then BID when stable ______ Notify Authorized Provider: for temp greater than 38.5° C systolic blood pressure less than 90 mmHg or greater than 160 mmHg diastolic blood pressure greater than 100 mmHg pulse less than 50 bpm or greater than 120 bpm True Urine output less than 120 mL in 4 hours O2 sats less than 92% Patient Care Tubes/Drains ______ Urinary catheter to straight drainage. Manual irrigation PRN ______ Catheter traction overnight. Discontinue catheter traction Post-Op Day 1 ______ NS bladder irrigation at a rate of 125 mL/h Or at a rate to maintain catheter patency Adjust rate to keep urine clear or light pink ______ Intake and Output Q4H x 24 hours, then QSHIFT and PRN ______ Snyder drain to suction. Empty and record volume QSHIFT and PRN Incision/Wound Care ______ Change Dressing 24 hours Post-Op, then PRN POC ______ POC Capillary Glucose: BID before meals or TID before meals or ______ If POC ordered – Authorized Provider to reassess after 72 hours TID AC and QHS Laboratory ______ CBC with diff, Electrolytes, Creatinine Day 1 Post-Op Day 1 and Day 2 Post-Op Authorized Provider’s Signature ______________________ Date ______________ Time __________ Page 1/2 GBHN/Radical Prostatectomy Post op/MD/06-15/v6 Copyright © 2007-2015 Grey Bruce Health Network NOTE: this is a CONTROLLED document as are all files on this server. Any documents appearing in paper form are not controlled and should ALWAYS be checked against the server file versions (electronic version) prior to use. ADDRESSOGRAPH GREY BRUCE HEALTH NETWORK Page 2 of 2 SITE: __________________ Allergies: □ NKA or: __________________________ Weight (kg) _____________ Height (cm) ______________ Radical Prostatectomy Post-Operative Order Set IV Solutions ______ IV Fluid: ______ ______ Ringers Lactate 125 mL/h 2/3 1/3 NS With 20 mEq KCl per L of IV fluid With 40 mEq KCl per L of IV fluid Rate ___________________ mL/h ______ Saline lock IV when drinking well Medications ______ Belladonna and Opium suppository Rectally Q6H PRN (Not to be discontinued when Spinal/Epidural Analgesia Post-Operative Order Set is used) ______ bisaCODYL suppositories 10 mg Daily Rectally, starting Post-Op Day 1, until flatus ______ Docusate Sodium 100 mg PO BID ______ Hyoscine Butylbromide 20 mg IV or Subcutaneous Q4H PRN ______ Home medications as per Medication Reconciliation History sheet when signed by Authorized Provider Antibiotic Prophylaxis ______ ______ ______ ______ ______ Cephalexin 500 mg PO BID Nitrofurantoin SR 100 mg PO Daily Diabetes Management Hypoglycemia Clinical Protocol greater than or equal to 18 years Subcutaneous Insulin Order Set Nicotine Replacement Therapy Nicotine Replacement Therapy (NRT) Order Set VTE Prophylaxis Management ______ Patient has been assessed for VTE Prophylaxis Management: Bleeding Risk ______ VTE Prophylaxis Order Set if indicated to be signed by Authorized Provider LOS less than 48 hours Admission/Discharge/Transfer ______ Plan for Post-Op Day 1 – 3 discharge ______ Follow up in 2 weeks for catheter removal after cystogram Consults ______ CCAC for catheter care, wound care and supplies ______ Physiotherapy Other ______ Order Set Orderable – (Automatic order for statistical reports) Authorized Provider’s Signature ______________________ Date ______________ Time __________ Page 2/2 GBHN/Radical Prostatectomy Post op/MD/06-15/v6 Copyright © 2007-2015 Grey Bruce Health Network NOTE: this is a CONTROLLED document as are all files on this server. Any documents appearing in paper form are not controlled and should ALWAYS be checked against the server file versions (electronic version) prior to use.