Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
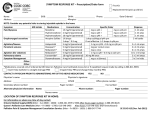
Saint John Regional Hospital CVS ICU Post-Op Order Set Nutrition NPO Activity Bedrest Elevate head of bed 30 degrees when hemodynamically stable Turn and position q2h Vital Signs BP, MAP, P, R, PAS, PAD, PAM, CO, CI, SVR, PVR, CVP q15min until stable then q1h then q4h and PRN Temperature q1h until 36 degrees Celsius, then q4h ETCO2 continuous until extubated Neuro checks q1h until awake then q4h Labs CBC, electrolytes, urea, creatinine, glucose, PT-INR, PTT activated, magnesium, ionized calcium, ABG, MVG immediately post-op and morning post-operative day one Blood gas lytes arterial q1h x 4 then q2h x 4 then q4h and PRN Troponin T 4 hours post-op CBC 6 hours post-op Diagnostic Imaging Chest x-ray immediately post-op Routine chest x-ray every morning while in ICU Electrodiagnostic Testing ECG immediately post-op. ECG with every rhythm or ST change. Routine ECGs every morning while in ICU IV Infusion Surgeon dependent o 0.9% NaCl @ 50mls/hr o D5W & 0.45% NaCl @ 50mls/hr o D5W @ 50mls/hr Analgesics Morphine Sulfate 2.5-5 mg IV q30min PRN while intubated For extubated patients under 80 kg: morphine sulfate 5 to 7.5 mg IM q3h PRN For extubated patients 80 kg or >: morphine sulfate 10 to 12.5 mg IM q3h PRN For patients allergic to morphine or codeine o Fentanyl 50 to 100 mcg IV q1h PRN For one surgeon: ketorolac 30 mg IV when patient placed on PSV if creatinine is within normal limits and chest tube drainage <100mls/hr For minimally invasive approach and some Transapical Aortic Valve Implantation patients o Ketorolac 15 mg IV q6h for 48 hours o Acetaminophen 975 mg PO q6h o Gabapentin 100 mg PO TID Antiemetic Ondansetron 4 mg IV q6h PRN Antipyretic Acetaminophen suppository 650 mg q4h PRN temperature > 38.5 degrees Celsius Antibiotic Cefazolin 1000 mg q8h x 3 doses for three surgeons, x 4 doses for one surgeon. First dose in ICU is given 3 hours after the last dose in the OR. For patients 100kg or > dose increases to 2000mg. If bilateral thoracic arteries are utilized three of the surgeons will extend the number of doses to 9 or 10. If the patient has a true penicillin allergy, vancomycin is utilized. Antiarrhytmic One surgeon will give 2 gm of magnesium sulfate immediately post-operatively Three surgeons give 2 gm of magnesium sulfate routinely the morning of post-op day one Antiheparin Two surgeons give protamine 50 mg x 2 doses post-op One surgeon gives protamine 50 mg x 1 dose post-op One surgeon does not use any additional protamine in the ICU (the cell saver is used for all of his patients) Antihypertensive Agents Nitroprusside infusion (0.25 to 5 mcg/kg/min) o For the first 1 to 2 hours SBP is maintained between 80 – 100 mmHg o After this time if the patient is not bleeding the pressure is allowed to rise. Each surgeon varies in parameters for pressure MAP less than 95 SBP less than 110 SBP less than 120 SBP less than 140 If nitroprusside infusion is at 1 mcg/kg/min nurses are able to utilize labetalol for hypertenision PRN. o Three surgeons will give 10 mg bolus doses q10min PRN o One surgeon will give an infusion of 100 mg over 2 hours q8h PRN o Hold parameters are for a heart rate less than 60 or a cardiac index less than 2.2 Coronary Perfusion/Spasm All patients who underwent bypass grafting surgery will be placed on a nitroglycerin drip at 0.25 mcg/kg/min for coronary perfusion and prevention of vasospasm Volume Resuscitation Three surgeons will use volulyte, with different parameters and volume amounts. o To maintain CVP 5-10 if MAP<65 (maximum of 750 mls) o To maintain CVP 4-12 (maximum of 1000 mls) o To maintain CVP 6-12 (maximum of 1000 mls) One surgeon will use voluven, to maintain a CVP 6-12 to a maximum of 1000 mls. Two surgeons will use crystalloid (0.9 % NaCl, D5W & 0.45% NaCl, or Ringer’s Lactate) if the patient requires more volume If a patient has renal insufficiency or is bleeding 3 of the surgeons will use 5% albumin in place of the volulyte or voluven. One surgeon will use crystalloid instead of volulyte. Insulin Infusion Humulin R drip: titrate to maintain glucose 6-9 mmol/L @ nurse’s discretion. Maximum rate for three surgeons is 15 units/hr. One surgeon has no maximum. ACCUs q1h. If no change in infusion after two serial checks may do ACCUs q2h. For glucose below 4 please give 25 mL of 50% dextrose. Please recheck glucose in 15 minutes. Sedation Propofol infusion 5 to 75 mcg/kg/min as needed for sedation Midazolam 2 mg IV q30min PRN Shivering Meperidine 25 mg q30min PRN. Stop after 2 doses. (Typically only used by one surgeon) Rocuronium 50 mg PRN Thromboembolic Prophylaxis Three surgeons will give an ASA (325 mg) 7 hours post-op in patients who have had bypass grafting. One surgeon will give an ASA (325 mg) 7 hours post-op in all of his patients Chest Tubes Connect to under water seal drainage with suction at 20 cm Strip chest tubes q15min x 2 hours and then q1h (for two surgeons) Strip chest tubes lightly q1h (for two surgeons) Nursing Fluid Balance Connect foley catheter to urometer Intake and output q1h Titrate total fluid intake to 50 mL/hr Suspend all PO medications Test ventricular pacemaker settings on arrival. Pacing wires are to be tested q12h while in ICU. Transfuse with red cell concentrates to maintain HGB greater than 70 (for most patients). In older patients and patients with renal disease they will maintain a HGB greater than 80. Insert an oral gastric tube and connect to low suction. Flush OG with 10 mL of NaCl q4h. Respiratory Ventilation: o PRVC AC at RT’s discretion (for 3 surgeons) o PRVC/SIMV respiratory rate 10; tidal volumes around 10 mls per kg; Peep 5; FiO2 0.6 o When stable awake and extubate at the discretion of RRT