Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
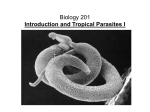
Elephantiasis and Its Treatment 1 Elephantiasis and Its Treatment Elephantiasis, or lymphatic filariasis, is a rare disorder of the lymphatic system caused by parasitic worms that are transmitted by mosquitoes. Elephantiasis leads to a generalized enlargement of the lymphatic vessels, termed lymphoedema. Inflammation of the lymphatic vessels causes the infected area to enlarge, most commonly limbs or parts of the head and torso. While anyone can contract the parasitic worms, elephantiasis is most common in tropical regions. It occurs frequently in Africa when an infected female mosquito injects microfilariae, the parasite, into the blood. The microfilaria reproduces and spreads throughout the bloodstream, where they can live for many years (Weil, Lammie, & Weiss, 1997). This devastating parasite cripples the individual over time and intervenes with their daily life. Elephantiasis is a vivid and accurate term for the condition that produces swelling in the extremities. It is a rare disorder of the lymphatic system caused by parasitic worms such as Wuchereria bancrofti, Brugia malayi, and B. timori (Vhi Healthcare, 2002-2003). These worms are transported to their host by mosquitoes found mostly in tropical and subtropical places. They are particularly dangerous to humans because they obstruct the lymphatic system. The lymph nodes in the lymphatic system help sustain fluid balance in the body and immunity. Any blockage to these vessels causes tissue destruction, or swelling called lymphoedema, which can cause crippling effects over time. Furthermore, different species of mosquitoes transmit different round worms that cause elephantiasis. Research conducted by microbiologists reveals that “Culex, Aedes, and Anopheles mosquitoes are the carriers of W.bancrofti. Anopheles and Mansonia mosquitoes are the carriers of B. malayi, and Anopheles mosquitoes are the carriers of B. Elephantiasis and Its Treatment 2 timori” (Vhi Healthcare, 2000-2003, p. 3). Moreover, when a person is bitten, the larvae in the mosquito travel through the blood stream of the host. These parasites are destined to the lymph nodes of the lymphatic system. Eventually, it blocks the lymph node vessels, causing swelling and disfiguration of the limbs because lymph fluid cannot be drained from the tissues. Elephantiasis continues to spread as the infected individual is bitten by mosquitoes not carrying the parasite. When the mosquito bites an uninfected person, the cycle repeats inside the new host. Individuals with lymphatic filariasis show no symptoms of carrying this rare disease (Weil, Lammie, & Weiss, 1997). Once infected, the parasite can reside unnoticed. Most will miss any sign of infection until the adult worm dies about seven years after infection. The worm hosts in the lymph vessels; once it dies, the lymph system’s function decomposes. This causes fluid to collect in the lymph system, resulting in severe swelling to arms, legs, breasts, and genitals. The function of the corrupted lymph system also causes hardening to the skin, due to the decreased performance of the immune system. Long term effects caused by lymphatic filariasis are permanent damage to lymph system, kidneys and disability. Persons carrying this rare disease are often shunned from their community. This prevents the infected individual from supporting their family (“CDC,” 2003). Lymphatic filariasis creates a global burden. According to the Global Programme to Eliminate Lymphatic Filariasis Annual Report, 120 million people are infected with elephantiasis and more than a billion people are at risk. The disease is an endemic in more than 80 countries and territories. Most of these cases occur in third-world countries because the population is generally poor and lacks access to adequate health care. Elephantiasis and Its Treatment 3 Contaminated regions have steadily increased because of the expansion of slums and poverty, especially in Africa and the Indian subcontinent. About 90% of the lymphatic filariasis infections occur in South East Asia, Western pacific regions of East Africa, Eastern Mediterranean Region and Region of Americas. The remaining 10% of the infections occur in Asia and various Pacific Islands. Lymphatic filariasis is thought to be the second leading cause of permanent and long-term disability (Dreyer, 2002). An individual with elephantiasis will first notice abnormal growths that may superficially appear as a typical insect bite. Most patients will first seek advice from their family physician concerning the abnormal growth. However, if the patient’s condition progresses before seeking help, the site of infection can enlarge and produce a grid or brick like pattern on the skin. The skin is often accompanied by foul smelling bacteria and fungi and becomes extremely engorged. These conditions are clear indicators to the physician that treatment for lymphoedema must begin before permanent damage occurs to lymphatic vessels, muscle, and nervous tissue. However, the family physician will need further tests to determine that microscopic parasites are responsible for the patient’s lymphoedema. Commonly, a nurse will take blood samples and a lab technician will separate the lymph using a centrifuge. The presence of filarial worms is easily detected with a microscopic analysis and elephantiasis is confirmed with relative certainty. (Erikson, Kobayashi, & Vogel, 2003). Resolving elephantiasis first begins with eliminating the parasitic worms. If the worms are in the larva stage, the physician will prescribe Ivermectin. Ivermectin is not approved by the Food and Drug Administration, but is available in the United States Elephantiasis and Its Treatment 4 under agreement with the Center for Disease Control. Adult worms are eliminated with the FDA approved drug Hetrazan (Farley, 1997). With the parasites removed from the lymph system, the family physician will focus on restoring function to affected limbs. Antibiotics are used to treat bacterial and fungal infections. Skin lesions are treated with topical keratolytic and oral retinoids, but the patient may have to use these drugs indefinitely in order to maintain the positive results (Erikson, Kobayashi, & Vogel, 2003). Urologists and cosmetic surgeons work together to correct possible swelling in the genitals. The generalized swelling of limbs from elephantiasis is reversed with restrictive stockings that compress previously fluidfilled tissue. If affected limbs cannot be improved with standard compression stockings, the physician may recommend pneumatic stockings that maintain an even greater pressure over the affected limb. However, the most severely affected patients may have their extremities amputated if treatments fail to reduce swelling. Physical therapy is coupled with medication to restore the patient’s mobility. Ironically, the areas of the world that are most plagued by elephantiasis do not have access to these resources. As technology advances, it should be the goal of scientists worldwide to conduct more laboratory tests and improve treatment of elephantiasis. Like other diseases, treatment is most effective when coupled with early detection. However, this disease is difficult to detect during its early stages. Therefore, to prevent this disease from spreading even further, it is imperative that more research is performed regarding its prevention, treatment, and rehabilitation. Someone with elephantiasis has to live everyday with feelings of shame and embarrassment about their physical condition. Elephantiasis and Its Treatment 5 Continued advances in elephantiasis will diminish this problem that plagues third world countries. Elephantiasis and Its Treatment 6 An individual with elephantiasis. The large masses on the legs are caused by lymph fluid buildup in the limbs. Brugia malayi, one of worms that cause elephantiasis. Elephantiasis and Its Treatment 7 Work Cited Center for Disease Control. (2003). Division of Parasitic Diseases – Lymphatic filariasis. Retrieved March 10, 2004 from http://www.cdc.gov/ncidod/dpd/parasites/lymphaticfilariasis/factsht_lymphatic_fi lar.htm Dreyer, H. (2002). Basic Lymphoedema Management: Treatment and Prevent of Problems Associated with Lymphatic Filariasis. Hollis NH. Hollis Publishing Company. Erickson, Q., Kobayashi, T., & Vogel, P. (2003). Diagnosis of skin diseases. American Family Physician, 76, 583-585. Farley, D. (1997). Treating tropical diseases. FDA Consumer, 31, 26-31. Vhi Healthcare. (2003). Elephantitis: Causes, Symptoms and Definition. Retrieved March 18, 2004 from http://www.raintree-health.co.uk/cgibin/getpage.pl?/data/elephantitis.html Weil, G., Lammie, P., & Weiss, N. (1997). The ICT Filariasis Test. A Rapid-format Antigen Test for Diagnosis of Bancroftiam Filariasis, 13, 401-404. World Health Organization. (2002). Global Programme to Eliminate Lymphatic Filariasis Annual Report. Geneva: Author.