Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
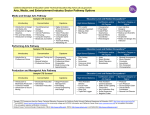
Prostate Cancer Treatment Pathway Version 2015.11 Disclaimer The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Pathway Preamble Target Population Patients with a confirmed prostate cancer diagnosis who have undergone the recommended diagnostic and staging procedures outl ined in the Prostate Cancer Diagnosis Pathway. Pathway Considerations Primary care providers play an important role in the cancer journey and should be informed of relevant tests and consultation s. Ongoing care with a primary care provider is assumed to be part of the pathway. For patients who do not have a primary care provider, Health Care Connect is a government resource that helps patients find a doctor or nurse practitioner. Throughout the pathway, a shared decision-making model should be implemented to enable and encourage patients to play an active role in the management of their care. For more information see Person-Centered Care Guideline and EBS #19-2 Provider-Patient Communication* Hyperlinks are used throughout the pathway to provide information about relevant CCO tools , resources and guidance documents. The term health care provider , used throughout the pathway, includes primary care providers and specialists, nurse practitioners, and emergency physicians For more information on Multidisciplinary Cancer Conferences visit: MCC Tools For more information on wait time prioritization, visit: Surgery, Systemic therapy and Radiation wait time prioritization Clinical trials should be considered for all phases of the pathway. Psychosocial care should be considered an integral and standardized part of cancer care for patients and their families at al l stages of the illness trajectory. For more information visit EBS #19-3 The following should be considered when weighing the treatment options described in this pathway for patients with potentiall y lifelimiting illness: Palliative care may be of benefit at any stage of the cancer journey , and may enhance other types of care – including restorative or rehabilitative care – or may become the total focus of care Ongoing discussions regarding goals of care is central to palliative care, and is an important part of the decision-making process. Goals of care discussions include the type, extent and goal of a treatment or care plan, where care will be provided, which health care providers will provide the care, and the patient s overall approach to care. For more information on the systemic treatment QBP please refer to the Quality-Based Procedures Clinical Handbook for Systemic Treatment * Note. EBS #19-2 is older than 3 years and is currently listed as For Education and Information Purposes . This means that the recommendations will no longer be maintained but may still be useful for academic or other information purposes. Confidential Draft For Review Only Version Version 2015.11 yyyy.mm Page 22 of of 11 11 Pathway Legend Shape Guide Colour Guide Intervention Primary Care Decision or assessment point Supportive and End of Life Care Patient (disease) characteristics Pathology Consultation with specialist Exit pathway Diagnostic Assessment Program (DAP) X Surgery or X Prostate Cancer Treatment Pathway Off-page reference Patient path Radiation Oncology Medical Oncology R Referral Radiology W Wait time indicator time point Multidisciplinary Cancer Conference (MCC) Line Guide Required Possible Pathway Disclaimer This pathway is a resource that provides an overview of the treatment that an individual in the Ontario cancer system may receive. The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medic al advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. While care has been taken in the preparation of the information contained in the pathway, such information is provided on an as-is basis, without any representation, warranty, or condition, whether express, or implied, statutory or otherwise, as to the information s quality, accuracy, currency, completeness, or reliability. CCO and the pathway s content providers (including the physicians who contributed to the information in the pathway) shall have no liability, whether direct, indirect, consequential, contingent, special, or incidental, related to or arising from the information in the pathway or its use thereof, whether based on breach of contract or tort (including negligence), and even if advised of the possibility thereof. Anyone using the information in the pathway does so at his or her own risk, and by using such information, agrees to indemnify CCO and its content providers from any and all liability, loss, damages, costs and expenses (including legal fees and expenses) arising from such person s use of the information in the pathway. This pathway may not reflect all the available scientific research and is not intended as an exhaustive resource. CCO and its content providers assume no responsibility for omissions or incomplete information in this pathway. It is possible that other relevant scientific findings may have been reported since completion of this pathway. This pathway may be superseded by an updated pathway on the same topic. © CCO retains all copyright, trademark and all other rights in the pathway, including all text and graphic images. No portion of this pathway may be used or reproduced, other than for personal use, or distributed, transmitted or "mirrored" in any form, or by any means, without the prior written permission of CCO. Prostate Cancer Treatment Pathway Low Risk Version 2015.11 Page 3 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Screen for psychosocial needs, and assessment and management of symptoms. Click here for more information about symptom assessment and management tools Consider the introduction of palliative care, early and across the cancer journey. Click here for more information about palliative care. Watchful Waiting Ongoing assessment for symptoms and monitoring development of metastatic disease. Frequency up to dis cretion of managing physician PSA Test, DRE, Imaging as indicated No From Diagnosis Pathway (Page 5) Low Risk (must include all of the following): T1-T2a, Gleason score 6, PSA 10ng/mL R Assess candidacy for curative treatment (e.g. comorbidities, life expectancy, patient preference) MCC Life expectancy <10 years Yes PSA Test every 3-6 months DRE every year Urologist Patient considers options Patient s treatment decision Patient education regarding treatment options Active Surveillance EBS #17-9 Confirmatory TRUS biopsy Serial biopsy at within 6-12 a minimum months every 3-5 years (minimum 12 thereafter cores) Radical Prostatectomy Open, laparoscopic or robotic-assisted EBS #17-3 W Standard Pelvic Lymph Node Dissection EBS #17-3 . Quality-Based Procedures Clinical Handbook for Cancer Surgery External Beam Radiation Therapy W 1 A Proceed to Page 8 Patient candidate for curative treatment? Consultations to discuss ALL treatment options Radiation Oncologist1 Progression to metastatic prostate cancer If low risk prostate cancer patients are seeking definitive treatment, a radiation oncology consultation should be sought. Or Brachytherapy EBS #3-10 Peer Review Multiparametric MRI if discordance between clinical and pathological findings or suspected disease progression Patient preference Or meets defined progression or reclassification criteria Proceed to Appropriate Active Treatment EBS #17-9 B Proceed to Page 6 Proceed to Prostate Cancer Follow-up Pathway Prostate Cancer Treatment Pathway Intermediate Risk Version 2015.11 Page 4 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Screen for psychosocial needs, and assessment and management of symptoms. Click here for more information about symptom assessment and management tools Consider the introduction of palliative care, early and across the cancer journey. Click here for more information about palliative care. Watchful Waiting Ongoing assessment for symptoms and monitoring development of metastatic disease. Frequency up to dis cretion of managing physician PSA Test, DRE, Imaging as indicated No From Diagnosis Pathway (Page 5) Intermediate Risk Any one of the following: PSA 10-20, Gleason score 7, T2b, and asymptomatic for metastases R Assess candidacy for curative treatment (e.g. comorbidities, life expectancy, patient preference) MCC Radiation Oncologist Radical Prostatectomy Open, laparoscopic or robotic-assisted EBS #17-3 Yes W Standard Pelvic Lymph Node Dissection EBS #17-3 D Proceed to Page 6 Quality-Based Procedures Clinical Handbook for Cancer Surgery Patient considers options Patient s treatment decision Radiation therapy according to Radiation Oncologist opinion3 Brachytherapy EBS #3-10 Patient education regarding treatment options Or W External Beam Radiation Therapy Or Combined Modality Treatment (Brachytherapy and External Beam Radiation Therapy) 2 Active surveillance may C Proceed to Page 8 Patient candidate for curative treatment? Consultations to discuss ALL treatment options2 Urologist Progression to metastatic prostate cancer be considered for a highly selective subset of patients in the intermediate risk group presenting with the following features: Stage T2 Gleason score 7/10 (3+4) with < 10% of total tumor pattern Gleason 4 and patient life expectancy 10-15 years, refer to EBS #17-9 3Neoadjuvant/adjuvant androgen deprivation therapy can be considered for select patients. Peer Review Proceed to Prostate Cancer Follow-up Pathway Prostate Cancer Treatment Pathway High Risk/Locally Advanced Version 2015.11 Page 5 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Screen for psychosocial needs, and assessment and management of symptoms. Click here for more information about symptom assessment and management tools Consider the introduction of palliative care, early and across the cancer journey. Click here for more information about palliative care. Watchful Waiting Ongoing assessment for symptoms and monitoring development of metastatic disease. Frequency up to dis cretion of managing physician PSA Test, DRE, Imaging as indicated No From Diagnosis Pathway (Page 5) High Risk Any one of the following: T2c or higher, Gleason score 8, PSA 20ng/mL, and select patients with nodal involvement R Assess candidacy for curative treatment (e.g. comorbidities, life expectancy, patient preference) MCC Radical Prostatectomy Open, laparoscopic or robotic-assisted EBS #17-3 Yes Consultations to discuss ALL treatment options Radiation Oncologist E Proceed to Page 8 Patient candidate for curative treatment? W Urologist Progression to metastatic prostate cancer F Proceed to Page 6 Standard Pelvic Lymph Node Dissection EBS #17-3 Quality-Based Procedures Clinical Handbook for Cancer Surgery Patient considers options Patient s treatment decision Patient education regarding treatment options W Neoadjuvant Optimize Androgen bone Deprivation health Therapy External Beam Radiation Therapy Peer Review Adjuvant Androgen Deprivation Therapy Optimize bone health Proceed to Prostate Cancer Follow-up Pathway Prostate Cancer Treatment Pathway Low/Intermediate/High Risk continued Version 2015.11 Page 6 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Screen for psychosocial needs, and assessment and management of symptoms. Click here for more information about symptom assessment and management tools Consider the introduction of palliative care, early and across the cancer journey. Click here for more information about palliative care. G Proceed to Page 8 Positive B D F H No From Pages 3, 4, 5 (Radical Prostatectomy) Pathology PSA Test Lymph node status Yes, if one or more of the following: surgical margins positive, postprostatectomy PSA is rising and is > 0.1ng/mL R4 Radiation Oncologist Negative No, if pT2, negative margins and PSA 0.1ng/mL 4 Early referral recommended, refer to EBS #3-17 Rising PSA Patient candidate for adjuvant treatment? Yes Further treatment required? Observation Proceed to Page 7 Patient considers options Patient s treatment decision W Adjuvant External Beam Radiation Therapy Within 6-18 weeks following prostatectomy EBS #3-17 & Peer Review Proceed to Prostate Cancer Follow-up Pathway Proceed to Prostate Cancer Follow-up Pathway Prostate Cancer Treatment Pathway Primary/Local Recurrence Version 2015.11 Page 7 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Screen for psychosocial needs, and assessment and management of symptoms. Click here for more information about symptom assessment and management tools Consider the introduction of palliative care, early and across the cancer journey. Click here for more information about palliative care. Yes H From Page 6 or Prostate Cancer Follow-up Pathway Imaging Tests Bone Scan and X-Ray of suspicious areas CT Abdomen/ Pelvis Yes, if local recurrence suspected and no previous adjuvant therapies Biopsy 5 6 MCC6 No, if metastatic or patient received adjuvant radiation treatment following radical prostatectomy Urologist W MRI is appropriate when used for targeted biopsy Salvage radical prostatectomy following radiation therapy should be performed and offered at centres of known expertise PSA Test I Proceed to Page 8 Metastatic disease? No, if negative lymph nodes and PSA 0.1ng/mL Proceed to Prostate Cancer Follow-up Pathway J No Patient post radical prostatectomy without adjuvant radiation therapy with detectable rising PSA Pathology Patient candidate for Salvage Radical Prostatectomy? MCC Radiation Oncologist R W Proceed to Page 8 Progression Observation Yes Patient eligible for local salvage therapies with curative intent Pelvic MRI5 EBS #26-4 Salvage therapy based on prior treatment Patient post external beam radiation, brachytherapy, or combined modality treatment with detectable rising PSA or positive biopsy R Individualized Local Salvage (Surgery) Quality-Based Procedures Clinical Handbook for Cancer Surgery Yes, if lymph nodes positive and/ or post-prostatectomy PSA is rising AND is > 0.1ng/mL Neoadjuvant Optimize Androgen bone Deprivation health Therapy Salvage External Beam Radiation Therapy Peer Review Salvage Radiation Therapy? (Joint decision by Urologist and Radiation Oncologist) Proceed to Prostate Cancer Follow-up Pathway K No Observation Progression Proceed to Page 8 Prostate Cancer Treatment Pathway Metastatic/Secondary Recurrence - Hormone Naïve Version 2015.11 Page 8 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Screen for psychosocial needs, and assessment and management of symptoms. Click here for more information about symptom assessment and management tools Consider the introduction of palliative care, early and across the cancer journey. Click here for more information about palliative care. **The appearance of specific drugs on this pathway does not imply that the drugs are publicly funded. A C E G I J K From Treatment Pathway Pages 3, 4, 5, 6 or 7 Imaging Tests If not performed already Secondary Recurrence Following primary treatment with or without adjuvant or salvage therapy Urologist R Radiation Oncologist Bone Scan and X-Ray of suspicious areas CT Abdomen/ Pelvis Pelvic MRI From Diagnosis Pathway (Page 5) Negative Bone Scan and CT PSA rising and testosterone at castrate levels Follow-up / Surveillance Scheduling can vary. Managed by the treating physician. PSA Test, Imaging - As needed Consider ADT when PSA >5ng/ mL and/or PSA doubling time <3 months Intermittent Androgen Deprivation Therapy Or Orchiectomy EBS #3-1 PSA rising and testosterone at castrate levels PSA Test, Testosterone Levels Frequency determined by treating physician Metastatic Any of the following: Nodal Involvement7 Evidence of Metastasis Follow-up / Surveillance Scheduling may vary. Managed by the treating physician Low volume Or Orchiectomy EBS #3-1 Select patients with nodal involvement can be managed with the high risk/locally advanced pathway High volume defined as visceral metastases and/or 4 or more bone metastases (at least 1 beyond pelvis and vertabral column) 9 Limited course of docetaxel to androgen-depriv ation therapy in the setting of newly diagnosed metastatic androgen-sensitive prostate cancer, refer to EBS #3-15 10 Secondary Hormone Manipulation may include: antiandrogen, antiandrogen withdrawal, antiandrogen switch, luteinizing hormone releasing hormone (LHRH) switch, ketoconazole, or steroids For more information about early palliative care for advanced cancer refer to Zimmermann et al., (2014) Early palliative care for patients with advanced cancer: a cluster-randomized controlled trial. Lancet, 383(9930), 1721-30 Continue Androgen Deprivation Therapy EBS #3-1 Androgen Deprivation Therapy (ADT) EBS #3-1 Disease burden? Optimize bone health High volume of metastatic disease at presentation8 Continue Androgen Deprivation Therapy Intermittent or continuous depending on prior therapy EBS #3-1 PSA Test, Testosterone Levels, Imaging As needed M Progression 7 8 Radiation Oncologist R Medical Oncologist Response Evaluation PSA stable PSA stable Positive Bone Scan and/or CT EBS #3-1 PSA Test, Testosterone Levels Frequency determined by treating physician Response evaluation Optimize bone health Metastatic prostate cancer? Secondary Hormone Manipulation10 L Proceed to Page 9 Palliative Radiation Therapy Chemotherapy9 EBS #3-15 Page 8 for Secondary Hormone Manipulation or page 9 for Castrate Resistant Prostate Cancer (CRPC) depending on prior treatments and/or current presentation Prostate Cancer Treatment Pathway Metastatic/Secondary Recurrence - Castrate Resistant Version 2015.11 Page 9 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. Screen for psychosocial needs, and assessment and management of symptoms. Click here for more information about symptom assessment and management tools Consider the introduction of palliative care, early and across the cancer journey. Click here for more information about palliative care. **The appearance of specific drugs on this pathway does not imply that the drugs are publicly funded. L M From Treatment Pathway Page 8 CastrateResistant Prostate Cancer (CRPC) Rising PSA levels with testosterone at castrate level Imaging or Restaging Unless recently perfomed and no new or worsening symptoms Bone Scan and XRay of suspicious areas Continue Androgen Deprivation Therapy (with or without androgen receptor axis targeted therapy) Negative Bone Scans and CT and asymptomatic Optimize bone health PSA Test, Testosterone Levels Appropriate therapy includes one or more of the following depending on prior therapies: Androgen Deprivation Therapy indefinitely regardless of additional therapies EBS #3-15 Sequence of specialties and care is individualized Pelvic MRI And A systemic therapy with demonstrated survival benefit and quality-of-life benefits: Medical Oncologist Positive Bone Scans and/or CT Chemotherapy11,12 Urologist R Radiation Oncologist Primary Care Provider Supportive and End of Life Care Teams EBS #3-15 W Radioisotope Therapy for Bone Metastases EBS #3-15 Androgen Receptor Axis Targeted Therapy13 EBS #3-15 And Other therapies to consider: Palliative Radiation Therapy Optimize Bone Health 11 Docetaxel/prednisone PSA doubling time <8 months, symptoms suggestive of progression, and 6 months since last staging Appropriate therapies include: Metastatic CRPC? CT Abdomen/Pelvis CT Chest Follow-up / Surveillance Scheduling can vary. Managed by the treating physician. should be offered 12 Cabazitaxel and prednis one may be offered to men who experience progression with docetaxel 13 Therapies with demonstrated survival and quality-of-life benefit s are abiraterone acetate/prednisone; enzalutamide 14 Bone-Targeted Therapy may include zoledronic acid or denosumab For more information about early palliative care for advanced cancer refer to Zimmermann et al., (2014) Early palliative care for patients with advanced cancer: a cluster-randomized controlled trial. Lancet, 383(9930), 1721-30 Bone-Targeted Therapy14 Palliative Radiation Therapy Radioisotope Therapy for Bone Metastases EBS #3-15 Follow-up/ Surveillance Scheduling can vary. Managed by the treating physician. PSA Test, Testosterone Levels, Imaging As needed Androgen Receptor Axis Targeted Therapy13 EBS #3-15 Progression Chemotherapy11,12 EBS #3-15 Continuous Androgen Deprivation Therapy EBS #3-15 Psychosocial Oncology and supportive care Referral to appropriate specialist if additional support is required End of Life Care Planning Progression Proceed to End of Life Care Pathway (Page 10) Prostate Cancer Treatment Pathway End of Life Care Version 2015.11 Page 10 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. End of Life Care (refer to Collaborative Care Plan) Pathway Map Target Population: Individuals with cancer approaching end of life, and their families. While this section of the pathway map is focused on the care delivered at the end of life, the palliative care approach begins much earlier on in the illness trajectory. Refer to Screen, Assess & Plan within the Psychosocial & Palliative Care Pathway Map Triggers that suggest patients are nearing the last few months and weeks life ECOG/PatientECOG/PRFS = 4 OR PPS 30 Declining performance status/functional ability Gold Standards Framework indicators of high mortality risk Revisit Advance Care Planning Ensure the patient has determined who will be their Substitute Decision Maker (SDM) Ensure the patient has communicated to the SDM his/her wishes, values and beliefs to help guide that SDM in future decision making Discuss and document goals of care with patient and family Assess and address patient and family s information needs and understanding of the disease, address gaps between reality and expectation, foster realistic hope and provide opportunity to explore prognosis and life expectancy, and preparedness for death Introduce patient and family to resources in community (e.g., day hospice programs) Screen, Assess, Plan, Manage and Follow-Up + End of Life Care planning and implementation Collaboration and consultation between specialist-level care teams and primary care teams Develop a plan of treatment and obtain consent Determine who the person wants to include in the decision making process (e.g., substitute decision maker if the person is incapable) Develop a plan of treatment related to disease management that takes into account the person s values and mutually determined goals of care Obtain consent from the capable person or the substitute decision maker if the person is incapable for an end-of-life plan of treatment that includes: - Setting for care - Resuscitation status - Having, withholding and or withdrawing treatments (e.g. lab tests, medications, etc.) Screen for specific end of life psychosocial issues Specific examples of psychological needs include: anticipatory grief, past trauma or losses, preparing children (young children, adolescents, young adults), guardianship of children, death anxiety Consider referral to available resources and/or specialized services Identify patients who could benefit from specialized palliative care services (consultation or transfer) Discuss referral with patients and family Proactively develop and implement a plan for expected death Explore place-of-death preferences and assess whether this is realistic Explore the potential settings of dying and the resources required (e.g., home, residential hospice, palliative care unit, long term care or nursing home) Anticipate/Plan for pain & symptom management medications and consider a Symptom Response Kit (SRK) for unexpected pain & symptom management Preparation and support for family to manage Discuss emergency plans with patient and family (who to call if emergency in the home or long-term-care or retirement home) Home care planning Connect with CCAC early (not just for last 2-4 weeks) Ensure resources and elements in place Consider a Symptom Response Kit (SRK) with access to pain, dyspnea and delirium medication Identify family members at risk for abnormal/complicated grieving and connect them proactively with bereavement resources Eastern Cooperative Oncology Group Performance Status (ECOG); Palliative Performance Scale (PPS); Patient Reported Functional Status (PRFS) For more information on the Gold Standards Framework, visit http://www.goldstandardsframework.org.uk/ Prostate Cancer Treatment Pathway End of Life Care cont. Version 2015.11 Page 11 of 11 The pathway is intended to be used for informational purposes only. The pathway is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all pathways are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the pathway. In the situation where the reader is not a healthcare provider, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the pathway. The information in the pathway does not create a physician-patient relationship between Cancer Care Ontario (CCO) and the reader. At the time of death: Pronouncement of death Completion of death certificate Allow family members to spend time with loved one upon death, in such a way that respects individual rituals, cultural diversity and meaning of life and death Implement the pre-determined plan for expected death Patient Death Arrange time with the family for a follow-up call or visit Provide age-specific bereavement services and resources Inform family of grief and bereavement resources/services Initiate grief care for family members at risk for complicated grief Encourage the bereaved to make an appointment with an appropriate health care provider as required Bereavement Support and Follow-Up Offer psychoeducation and/or counseling to the bereaved Screen for complicated and abnormal grief (family members, including children) Consider referral of bereaved family member(s) and children to appropriate local resources, spiritual advisor, grief counselor, hospice and other volunteer programs depending on severity of grief Provide opportunities for debriefing of care team, including volunteers