Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
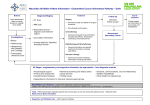
Rapid Access GI MDC for Early Cancer Diagnosis – Sara McCartney Speaker Key IV SM Interviewer Sara McCartney SM Hello. I’m Sara McCartney. I’m a Consultant Gastroenterologist at UCH and I’ve been talking today about introduction of a rapid access GI MDC, which is multidisciplinary clinic, to help with early diagnosis of cancer. IV Can you tell us about this new service? SM Well, one of the problems is that a lot of patients are diagnosed as emergencies and less than 50% of patients come through the two week wait pathway. We’re concerned that cancers are being diagnosed late; we want to diagnose them early so they get better treatment. There’s a coordinated pathway that’s good for patient care and a service that the GPs are happy with, that they can access easily when they’re worried about patients. Sometimes with the two week pathway patients don’t always fit the pathway requirements but an experienced GP may have a lot of knowledge and may feel that these patients are likely to have a cancer and want some early diagnosis. So we have four specific pathways that we’re assessing. This is a pilot project and we aim to look at around 100 patients and then reassess whether we’re doing the right thing. So the first group are patients with painless jaundice. The idea is that they don’t have gallstone disease; they do have a bilirubin of more than 80. The second group will be patients who’ve got a documented weight loss of more than 5% of their body weight and there’s no obvious reason for this. So this isn’t somebody who’s been depressed or had another illness or a thyroid disease. It’s someone that you really can’t explain why they’ve lost the weight. The third group which is probably the most interesting group are patients who’ve had vague abdominal symptoms and these are patients where the GP feels that there is a high likelihood that they might have cancer. They may not fit any of the other pathways. We’re looking for patients who have had symptoms for more than three weeks but less than six months, so not people who have had chronic symptoms for many years and not people who’ve had their symptoms investigated before. Typically this would be someone who doesn’t come to the GP surgery very often and because of that when they do come there’s a high index of suspicion of pathology and in this case particularly a worry about cancer. The fourth group really refers more to... is more important for the A&E practitioners rather than for the general practitioners because these will be people who come 1 through the A&E route and who have attended on more than one occasion in the last month with unexplained abdominal symptoms and for whatever reason they haven’t gone to their GP and they’ve come straight to A&E. IV How do you refer in? SM If you want to refer in to this service, it’s very straightforward. There’ll be a form which will be available at all practices and there’ll also be a patient leaflet. So the form just needs to be filled in and emailed through to a coordinator and we’ll give you the email address for that. The patient is then given a leaflet to tell them that they will be going to a Macmillan Cancer Centre. We think it’s important that they know there is a suspicion that they might have cancer although we do emphasise that that’s not necessarily the diagnosis, but that’s what we need to exclude. So the idea is that this is a very rapid access, so once we have the referral patients will be seen within 24 hours and will have their CT scans if required within 24 hours, blood tests will be done immediately, and if they require any endoscopy or further intervention these will be arranged. The idea is that over a period of seven to ten days all the investigations are completed. If they do have a cancer diagnosis, they’ll go on to an MDT discussion and if they don’t have a cancer diagnosis, appropriate further referral will be discussed with their GP. IV Where can GPs find out more? SM We have an email address for contact. It’s [email protected] and any queries or any forms can be sent there and they’ll be accessed rapidly. 2