Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
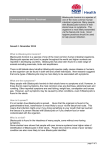
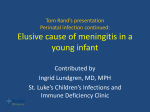
Blastocystis Hominis Delamon Rego February 2010 QuickTime™ and a decompressor are needed to see this picture. http://www.dpd.cdc.gov/DPDX/images/ParasiteImages/AF/Blastocystis/Bhominis_cyst_wtmt_io2.jpg Introduction: Blastocystis Hominis is a protozoan intestinal parasite belonging to the Blastocystis genus of Stramenopiles – a vast array of organisms including brown algae, water molds, and diatoms. It has a widespread geographic distribution and is found in countries of all income levels across the world. It's status as a true pathogen is controversial - while it has been found in patients with gastrointestinal symptoms it is not proven to be the cause, and many carriers are asymptomatic. Research on Blastocystis Hominis is limited, with large gaps remaining in our understanding of its life cycle, transmission mechanisms, incubation period, epidemiology, and treatment options. Agent (Classification and Taxonomy): Like most aspects of Blastocystis Hominis, the parasite’s taxonomy and classification is rather unclear. For many years opinion on the matter varied widely, placing the parasite alternatively as a yeast, fungus, or cyst stage of another organism.i Only recently was it classified as a protozoa after an analysis of small-subunit rRNA sequences placed it firmly as a member of the Stramenopiles.ii Different sources currently provide slightly different phylogenetic trees for Blastocystis Hominis. The National Center for Biotechnology Information (NCBI) lists the following, rather simple, version in their technology browser:iii Eukaryota Stramenopiles Genus: Blastocystis Species: Blastocystis Hominis A more complex tree (though older) tree is provided by Zierdt et al.., wherein the following breakdown is proposediv: Kingdom: Protista Subkingdom: Protozoa Phylum: Sarcomastigophora Subphylum: Sarcodina Superclass: Rhizopoda Class: Lobosea Subclass: Gymnamoeba Order: Amoebida Suborder: Blastocystina Genus: Blastocystis Species: Hominis Synonyms: The disease caused by Blastocystis Hominis, though its actual legitimacy is controversial, is referred to simply as Blastocystosis. There are no other widely used synonyms that refer to the parasite. History of Discovery: The genus Blastocystis was created by A. Alexieff in 1911. It was originally described as a yeast before being placed among the protozoans following a series of physiological and morphological comparisons carried out in the 1960s. Since then, studies have continued to try and reach accurate conclusions about many aspects of B. hominis.v Clinical Presentation in Humans: In so much as it exists, the clinical presentation of B. hominis is known as Blastocystocis. Again, there is controversy over whether or not Blastocystis Hominis is actually pathogenic or just part of the gut flora. Blastocystis has been found in people who report no symptoms, and it is estimating that most cases may be asymptomatic. Whether this is due to Blastocystis’ lack of pathogenicity or personal immunity of the host is unknown. A third possibility is that Blastocystis Hominis is split in several demes, some of which are infectious and some of which are not. Since most of the research on Blastocystis infection has been based on case reports, no conclusive evidence has emerged to answer these questions.vi Where symptoms have been attributed to the parasite, they have included diarrhea, nausea, abdominal cramps, bloating, excessive gas, and anal itching.vii The timescale of infection with the parasite can range from weeks to years.viii Transmission: The precise transmission mechanisms of Blastocystis Hominis remain murky. Fecal-oral transmission is the most accepted pathway, and recent studies have shown that transmission involves only the cyst form of the parasite.ix The extent to which humanhuman, human-animal, and animal-human transmission occurs is still unknown. Genomic studies provide evidence for all three routes, though experimental studies have yet to provide conclusive proof for the existence of either.x Reservoir: Conclusively stating that Blastocysistis Hominis has an animal reservoir depends upon unraveling the true nature of its transmission. If, as Noël et al. deem likely based upon their own molecular work and a review of the literature, animal-to-human transmission is possible, then animals such as pigs and dogs could in fact be acting as a large reservoir capable of human infection.xi Epidemiological studies finding that infection is more common in people living in proximity to farm animals or petsxii further supports this notion. However, until a conclusive study is published regarding the precise life cycle of B. hominis, the presence of a reservoir will continue to be unconfirmed. Vector: None Incubation Period: An accurate analysis of the incubation period of Blastocystis Hominis is pending while the details of its transmission mechanisms and life cycle remain murky. Morphology: Culture studies of Blastocystis Hominis have identified several main forms of the organism as well as a recently confirmed cyst stage.xiii -Vacuolar and granular forms: These consist of a spherical cell containing a large single vacuole. Granular cells contain many small granules in the cytoplasm or the central vacuole. The cells range between an average of 4 and 15 micrometers in diameter. Multiple nuclei (up to 4) can be present. These are the most common forms of B. hominis. -Multivacuolar and avacuolar forms: These contain many smaller vacuoles or no vacuoles within a smaller cell of between 5 and 8 micrometers in diameter. 1 nucleus tends to be present, with a maximum of two. -Ameboid form: This is a very rare form with irregularly shaped cells from 2.6 to 7.8 micrometers in diameter. Pseudopodia are often attached. A large central vacuole may or may not be present. -Cyst form: A hard, resistive form between 3 and 10 micrometers in diameter. A thick wall encapsulates the structure which includes many vacuoles and 1 or 2 nuclei. QuickTime™ and a decompressor are needed to see this picture. http://upload.wikimedia.org/wikipedia/commons/b/b9/Four_common_forms_of_Blastocy stis_hominis_Valzn.jpg Images of several forms of Blastocystis hominis. Life Cycle: QuickTime™ and a decompressor are needed to see this picture. http://www.dpd.cdc.gov/dpdx/HTML/Blastocystis.htm A CDC diagram of B. hominis’ life cycle. The lifecycle of B. hominis is, of course, not fully understood. The CDC approximation indicates the following, however. It is proposed that within the gut, vacuolar stages reproduce by mitosis, occasionally forming multi-vacuolar or ameboid forms. The ameboid form replicates further through mitosis, eventually undergoing schizogony before exiting the host as a thick-walled cyst. This cyst may then infect others via the fecal-oral pathway. The multi-vacuolar form, meanwhile, may undergo schizogony to become a thin-walled cyst that eventually ruptures to unleash new vacuolar cells.xiv Diagnostic Tests: Blastocystis Hominis is diagnosed using microscopy on a stool sample. The CDC recommends that samples be concentrated and at least three separate samples should be taken before a negative result is confirmed. The two most common methods for preparing slides are a wet mount and a trichrome stain. In the wet mount Blastocystis Hominis is stained with iodine and appears as a large vacuole in the middle of many small nuclei, though it may be difficult to see. In the trichrome stain, the parasite is stained with trichrome giving the large central body a gray or green appearance and the cytoplasm elements a dark red color.xv Management and Therapy: Even though the pathogenicity of Blastocystis Hominis remains controversial, antiprotozoan drugs have been used to treat individuals in whom the parasite is found. The most widely used treatment option is the chemotherapeutic drug Metronidazole which, while effective in some individuals, shows signs of resistance by B. hominis or limited effectiveness in others. At least one group of researchers has also used the drug combination Trimethoprim/Sulfamethoxazole (TMP/SMX) with similar effects. xvi More recently, Nitazoxanide has been with much more positive effects, with 86% of those treated with the drug effectively cured.xvii Epidemiology: Blastocystis Hominis has not been as reliably tracked as diseases such as malaria. Case reports indicate that while nearly worldwide in distribution, it is more common in less developed nations and may prefer tropical and sub-tropical climates. In addition, researchers have found that the ratio of urban-to-rural infection rates is 3:1. Proximity to pets and farm animals also appears to be linked with increased infection rates.xviii A study in Salamanca, Spain showed prevalence rates to be 2-3 times higher in day care centers and 4-6 times higher in primary schools than in the general population.xix Public Health and Prevention Strategies/Vaccines: Due to the uncertain infective nature and transmission pathways of the parasite, there are no widespread public health or prevention strategies directly aimed at Blastocystis Hominis. The CDC does list the following, however, as potentially useful preventative and control measures:xx -Handwash with soap and water before handling food and after using the toilet. If employed in a child-care center, also wash after each diaper change even if gloves were used. -Avoid potentially infected water and food -Wash and peel all raw fruits and vegetables -avoid untreated water in countries with less established water-safety standards It does not appear as if there are any vaccines for Blastocystis Hominis on the horizon. Useful Web Resources: http://www.cdc.gov/ncidod/dpd/parasites/blastocystishominis/factsht_blastocystis_homin is.htm -The CDC’s official fact sheet on Blastocystis Hominis, including great information for the beginner. http://cmr.asm.org/cgi/reprint/9/4/563 A great paper that touches upon many aspects of B. hominis from morphology to taxonomy and more. References: Stenzel, D. J.; Boreham, P.F.L. (1996). Blastocystis hominis Revisited. Clinical Microbiology Reviews 1996. Vol. 9 No. 4 p. 563-584. ii Silberman, J.D. et al. (1996). Human parasite finds taxonomic home. Nature, London 380, 398. iii http://www.ncbi.nlm.nih.gov/Taxonomy/Browser/wwwtax.cgi iv Zierdt, Charles et al. (1988). Biochemical and Ultrastructural Study of Blastocystis hominis. Journal of Clinical Microbiology. Vol. 26(5) May 1988, p. 965-970. v Ibid. vi Hotez, Peter. (2000). The other intestinal protozoa: Enteric infections caused by blastocystis hominis, entamoeba coli, and dientamoeba fragilis. Seminars in Pediatric Infectious Diseases 2000. Vol. 11 No. 3. i Centers for Disease Control and Prevention (http://www.cdc.gov/ncidod/dpd/parasites/blastocystishominis/factsht_blastocystis_homi nis.htm) viii Doyle, Patrick et al. (1990). Epidemiology and Pathogenicity of Blastocystis hominis. Journal of Clinical Microbiology. Jan. 1990. P. 116-121. ix H. Yoshikawa et al. (2004). Fecal-oral transmission of the cyst form of Blastocystis hominis in rats. Parasitol. Res. 2004 Dec; 94(6):391-6. Epub 21004 Oct 9. x H. Yoshikawa, N. Abe, M. Iwasawa et al., Genomic analysis of Blastocystis hominis strains isolated from two long-term health care facilities. J. Clin. Microbiol. 38 (2000), pp. 1324–1330. xi Noël, Christophe et al. (2003). Phylogenetic analysis of Blastocystis isolates from different hosts based on the comparison of small-subunit rRNA gene sequences. Molecular & Biochemical Parasitology 126 (2003). p. 119-123. xii P.W. Doyle, M.M. Helgason, R.G. Mathias and E.M. Proctor , Epidemiology and pathogenicity of Blastocystis hominis. J. Clin. Microbiol. 28 (1990), pp. 116–121. xiii Stenzel, D. J.; Boreham, P.F.L. (1996). Blastocystis hominis Revisited. Clinical Microbiology Reviews 1996. Vol. 9 No. 4 p. 563-584. xiv Centers for Disease Control and Prevention (http://www.dpd.cdc.gov/dpdx/HTML/Blastocystis.htm) xv Centers for Disease Control and Prevention (http://www.dpd.cdc.gov/DPDX/HTML/PDF_Files/Blasto_benchaid.pdf) xvi Moghaddam, D; Azami, M.; Ghadirian, E. (2005). Blastocystis hominis and the evaluation of efficacy of metronidazole and trimethoprim/sulfamethoxazole. Parasitol. Res. (2005) 96: 273-275. xvii Rossignol, JF et al. (2005). Clin Gastroenterol Hepatol. 2005 Oct;3(10):987-91. xviii P.W. Doyle, M.M. Helgason, R.G. Mathias and E.M. Proctor , Epidemiology and pathogenicity of Blastocystis hominis. J. Clin. Microbiol. 28 (1990), pp. 116–121. xix Martít-Sánchez, A.M. et al. (1992). Epidemiology and Clinical Significance of Blastocystis Hominis in different population groups in Salamanca (Spain). Eur. J. Epidemiol. Vol. 8, No. 4. (1992) p. 553-559 xx Centers for Disease Control and Prevention (http://www.cdc.gov/ncidod/dpd/parasites/blastocystishominis/factsht_blastocystis_homi nis.htm) vii Images: Life Cycle: http://www.dpd.cdc.gov/dpdx/HTML/Blastocystis.htm Morphology: http://upload.wikimedia.org/wikipedia/commons/b/b9/Four_common_forms_of_Blastocy stis_hominis_Valzn.jpg