Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hospital-acquired infection wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Neonatal infection wikipedia , lookup
Orthohantavirus wikipedia , lookup
Ebola virus disease wikipedia , lookup
West Nile fever wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Henipavirus wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Antiviral drug wikipedia , lookup
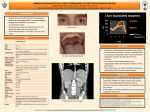
Sexually transmitted infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Leptospirosis wikipedia , lookup
Assessment and Management of Patients With Hepatic Disorders Part 1 1 2 3 Serum Aminotransferase or Transaminase Studies AST (SGOT) ALT (SGPT) GGT, GGTP LDH 10–40 units (4.8–19 U/L) 5–35 units (2.4–17 U/L) 10–48 IU/L 100–200 units (100–225 U/L) The studies are based on release of enzymes from damaged liver cells. These enzymes are elevated in liver cell damage. Elevated in alcohol abuse. 4 Definition Hepatitis is an inflammation of the liver. Viral hepatitis can be acute or chronic. There are five major categories of viral hepatitis (hepatitis F and G have been identified but are uncommon). Hepatitis A virus (HAV) Hepatitis B virus (HBV) Hepatitis C virus (HCV) Hepatitis D virus (HDV) Hepatitis E virus (HEV) 5 There are a lot of carriers and not infected persons People with hepatitis should never donate blood, body organs, or other body tissue. Every healthcare worker should take the series of hepatitis B vaccines. 6 7 8 High Risk Behaviors Failure to follow Universal Precautions Percutaneous exposure (dirty needles, sharp instruments, body piercing, tattooing,……) Unprotected sexual intercourse with a hepatitis-infected person; sex with multiple partners) Unscreened blood transfusions Hemodialysis 9 High Risk Behaviors Ingestion of food prepared by a hepatitisinfected person Using tap water to clean food products and drinking contaminated water) Eating and/or living in crowded environments (correctional facilities, dormitories, universities, long-term care facilities, military base housing) 10 Diagnostic Assessments and Nursing Interventions Albumin: Decreased (normal – 3 to 5 g/dL) Serologic Markers: Identify presence of virus (HAV, HBsAg and Anti HBc IgM, HCV, HDV, HEV). Serum presence of HBsAg for longer than 6 months indicates chronic hepatitis and/or hepatitis carrier status. Hepatitis antibody serum testing: Identify exposure to anti-HAV, HBsAb, anti-HCV, anti-HDV, anti-HEV. Serum presence of HBsAb indicates immunity to HBV either following recovery from hepatitis B or successful vaccination. Stool analysis for hepatitis A antigen 11 Diagnostic Assessments and Nursing Interventions Serum liver enzymes: Elevated ALT: Elevated (normal – 8 to 20 units/L; 3 to 35 IU/L); most definitive for assessment of liver tissue damage. AST: Elevated (normal – 5 to 40 units/L) Alkaline phosphatase (ALP): Elevated (normal – 42 to 128 units/L; 30 to 85 IU/L) Serum bilirubin: Elevated Bilirubin – direct (conjugated): Elevated (normal – 0.1 to 0.3 mg/dL) Bilirubin – indirect (unconjugated): Elevated (normal – 0.2 to 0.8 mg/dL) Bilirubin – total: Elevated (normal – 0.1 to 1.0 mg/dL) either following recovery from hepatitis B or successful vaccination. 12 Diagnostic Assessments and Nursing Interventions Abdominal films to visualize possible hepatomegaly, ascites, spleen enlargement. Liver biopsy: Most definitive. Identifies intensity of infection and degree of tissue damage. Nursing interventions include: pre & post procedural responsibilities) 13 Assessments Influenza symptoms (headache, fatigue, low grade fever, RUQ abdominal pain, N&V). HBV presents with additional symptoms: hepatomegaly, signs of obstruction (light colored stools, dark urine, jaundice, elevated bilirubin and liver enzyme levels). Assess for alterations in physical assessment related to hepatitis: Inspect overall color of skin, eyes, and mucus membranes for presence of jaundice and skin irritations probably due to pruritus. Pain in muscles, joints, and abdomen. Fever, malaise, increased fatigue, and N&V. Change in color of stool (clay colored) or dark urine. Palpate RUQ for swelling and complaints of tenderness. Have the client take deep breath to feel border of liver under ribs and measure/ record abdominal distention. 14 Assessments Pertinent Client History Take an inventory of recent travel, work history, and onset and intensity of symptoms. Identify measures the client has already taken such as pain medicine, fluids, and diet changes. Identify exposure agents. When interviewing the client, use a nonjudgmental manner. Behaviors that may have caused this disease occurred years before the present illness and can be embarrassing to the client to express comfortably. 15 A. HEPATITIS A VIRUS (HAV) HAV accounts for 20% to 25% of cases of clinical hepatitis in the developed world. Hepatitis A, formerly called infectious hepatitis The mode of transmission of this disease is the fecal–oral route, primarily through the ingestion of food or liquids infected by the virus. The virus has been found in the stool of infected patients before the onset of symptoms and during the first few days of illness. 16 Clinical Manifestations Many patients are anicteric (without jaundice) and symptomless. If symptoms appear, they are of a mild, flu-like upper respiratory tract infection, with low-grade fever. Anorexia, an early symptom, is often severe. Later, jaundice and dark urine may become apparent. Indigestion is present in varying degrees, marked by vague epigastric distress, nausea, heartburn, & flatulence. 17 Medical Management Bed rest during the acute stage and a diet that is both acceptable to the patient and nutritious are part of the treatment and nursing care. During the period of anorexia, the patient should receive frequent small feedings, supplemented, if necessary, by IV fluids with glucose. 18 Nursing Management The patient is usually managed at home unless symptoms are severe. Therefore, the nurse assists the patient and family in coping with the temporary disability and fatigue that are common in hepatitis and instructs them to seek additional health care if the symptoms persist or worsen. 19 B. HEPATITIS B VIRUS (HBV) Transmitted primarily through blood (percutaneous and permucosal routes). HBV has been found in blood, saliva, semen, and vaginal secretions and can be transmitted through mucous membranes and breaks in the skin. HBV is also transferred from carrier mothers to their babies, especially in areas with a high incidence (ie, Southeast Asia). The infection is usually not via the umbilical vein, but from the mother at the time of birth and during close contact afterward. HBV has a long incubation period. It replicates in the liver and remains in the serum for relatively long periods, allowing transmission of the virus. 20 B. HEPATITIS B VIRUS (HBV) transmitted primarily through blood (percutaneous and permucosal routes). HBV has been found in blood, saliva, semen, and vaginal secretions and can be transmitted through mucous membranes and breaks in the skin. HBV is also transferred from carrier mothers to their babies, especially in areas with a high incidence (ie, Southeast Asia). The infection is usually not via the umbilical vein, but from the mother at the time of birth and during close contact afterward. Those at risk for developing hepatitis B include surgeons, clinical laboratory workers, dentists, nurses, and respiratory therapists. Staff and patients in hemodialysis and oncology units and sexually active homosexual 21 Clinical Manifestations Clinically, the disease closely resembles hepatitis A, but the incubation period is much longer (1 to 6 months). Signs and symptoms of hepatitis B may be insidious and variable. Fever and respiratory symptoms are rare; some patients have arthralgias and rashes. Prevention The goals of prevention are to interrupt the chain of transmission, to protect people at high risk with active immunization through the use of hepatitis B vaccine, and to use passive immunization for unprotected people exposed to HBV 22 A. PREVENTING TRANSMISSION Continued screening of blood donors for the presence of hepatitis B antigens The use of disposable syringes, needles, and lancets and the introduction of needleless IV Good personal hygiene is fundamental to infection control. In the clinical laboratory, work areas should be disinfected daily. Gloves are worn when handling all blood and body fluids as well as HBAg positive specimens. Eating and smoking are prohibited in the laboratory and in other areas exposed to secretions, blood products. 23 B. Active Immunization: Hepatitis B Vaccine Active immunization is recommended for individuals at high risk for hepatitis B (eg, health care personnel and hemodialysis patients). In addition, individuals with hepatitis C and other chronic liver diseases should receive the vaccine. Administered IM (in the deltoid muscle in adults) in three doses, the second and third doses 1 & 6 months after the first dose. The third dose is very important in producing prolonged immunity. Antibody response may be measured by anti-HBs levels 1 to 3 months after completing the basic course of vaccine Universal vaccination of all infants. 24 C. PASSIVE IMMUNITY: HEPATITIS B IMMUNE GLOBULIN Hepatitis B immune globulin (HBIG) provides passive immunity to hepatitis B and is indicated for people exposed to HBV who have never had hepatitis B and have never received hepatitis B vaccine. Specific indications for postexposure vaccine with HBIG include: (1) inadvertent exposure to HBAg-positive blood through percutaneous (needlestick) or transmucosal (splashes in contact with mucous membrane) routes, (2) sexual contact with people positive for HBAg, and (3) perinatal exposure (babies born to HBV-infected mothers should receive HBIG within 12 hours of delivery). 25 NANDA Nursing Diagnoses Fatigue Nausea 26 Nursing Interventions Implement contact isolation precautions (universal precautions). Limit client activity (bedrest) in order to promote hepatic healing. Provide dietary education: high-carbohydrate, high-calorie, lowto moderate-fat, and low- to moderate-protein diet and small, frequent meals to promote nutrition and healing. Medications are used sparingly for hepatic rest and regeneration of tissue. Administer interferon (for HBV and HCV). Monitor clients receiving interferon for side effects of flu-like symptoms, alopecia, and bone marrow suppression. Monitor CBC and administer antiemetics as needed during interferon therapy. 27 Nursing Interventions Educate the client and family regarding measures to prevent transmission of disease with others at home Provide comfort measures. Encourage hepatitis prevention activities: Community health educational interventions on transmission and exposure. Hepatitis B vaccination prophylaxis for all healthcare workers. Proper use of Universal Precautions. Use of a needleless system when delivering 28 medications Nursing Interventions Frequent handwashing If traveling in underdeveloped countries, drink bottled water, and limit sharing of bed linens and eating utensils. Report hepatitis outbreaks to health authorities. Instruct clients to avoid alcohol and all OTC Consider administration of immunoglobin (Ig) to clients exposed to hepatitis A or hepatitis B. 29 Complications and Nursing Implications Chronic hepatitis – results from hepatitis B, C, or D. Increases the client’s risk for liver cancer. Fulminating hepatitis (fatal); due to the inability of the liver cells to regenerate with increased progression of the necrotic process. This disease results in hepatic encephalopathy and death. Cirrhosis of the liver – continued episodes of chronic hepatitis result in scarring and permanent injury to the liver and also is a risk factor for liver cancer. 30 Complications and Nursing Im Liver cancer – chief report is abdominal discomfort. Diagnosis is made by US, CT, elevated liver enzymes, and liver biopsy for confirmation of cancer. Liver failure – chronic hepatitis, liver abscesses, and fatty liver infiltration all result in changes within the healthy liver and cause irreversible damage 31