Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
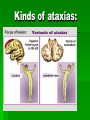
Multiple sclerosis (MS) PROF.SHKROBOT Multiple sclerosis (MS) – is a chronic disease that begins most commonly in young adults and is characterized pathologically by multiple areas of central nervous system (CNS) white matter inflammation, demyelination, and glial scarring (sclerosis) Epidemiology Age of onset is between 20 – 40 years. Usually it is 21 – 25 years, in women – 2 – 3 years earlier. In women the incidence of MS is 1.5 – 2 times higher than in men. Nowadays there are about 2 mln people with MS all over the world . The geographic distribution is uneven. Most of northern USA, southern Canada, northern Europe, southern Australia and New Zealand are areas of high prevalence. Epidemiology In Ukraine the incidence of MS is 15 per 100 000 people. But it is much more higher in western regions (25 per 100 000 people) than in eastern and southern ones (6 – 8 per 100 000 people). Multiple sclerosis (MS) – The main cause of the increased growth of the disease Better diagnosis Unitary diagnostic scales Increasing possibilities of treatment that leads to the growth of percentage of the patients with long lasting course of the disease True growth of MS incidence Etiology The cause of MS is unknown. There are 2 groups of possible reasons of the disease: Genetic susceptibility Environmental factors Infections (the virus can influence on nervous system directly or through the autoimmune mechanisms). Geographical (ground, water properties, the number of light days in a year) Toxic Social conditions Diet (domination of meat in the diet) Other factors (trauma) The typical features of MS pathogenesis Clinical and immune signs are closely connected with each other in MS patients. Usually immune signs are the first ones There is disturbance of activating and suppressing cytokines balance The immunity is changed in the course of the disease There are signs of immune suppression and immune modulation according to the stage of the disease – exacerbation or remission Pathogenesis Different etiologic agents provoke autoimmune mechanisms. The result of this process is myelin destruction. At the beginning of the process auto-allergic processes prevail over the other ones. Then immunodeficiency is developed. Pathogenesis The typical features of MS pathogenesis are: Clinical and immune signs are closely connected with each other in MS patients. Usually immune signs are the first ones There is disturbance of activating and suppressing cytokines balance The immunity is changed in the course of the disease There are signs of immune suppression and immune modulation according to the stage of the disease – exacerbation or remission Pathology There are multiple areas of Central Nervous System white matter inflammation, demyelination and glial scarring (sclerosis). The lesions are multiple in space. They are located in: spinal cord cerebellum Optic n. brain white substance The beginning of the disease Paresthesia. It is the feeling of numbness or tingling in one of the extremity. It can be spread during the next 3 – 4 days and lasts for about 1 – 2 weeks, then gradually disappear Motor disorders - weakness in lower extremities. This symptom is much more common at the age of 25 – 40 years Retrobulbar neuritis is a progressive loss of vision, colour vision disturbances. It lasts for about several weeks The beginning of the disease Oculomotor n. disorders (diplopia and cross eye) Pelvis disorders (retention of urine, micturition) Acute vestibular syndrome Cerebellar disorders – ataxia, disorders of coordination ROMBERG TEST Typical clinical features Motor disorders – 89 – 97% Ataxia – cerebellar, sensitive and vestibular – 62 – 74% Sensory disorders – pains and sensitive ataxia - 72 – 74% Brain stem symptoms – vestibular syndrome, dysarthria, CN’s lesion – 47 – 58% Visual and eye movements disorders – 42 – 52% Autonomic disturbances – pelvic and sexual disorders – 46 – 60% Nonspecific symptoms – cognitive, memory disturbances, loss of attention – 62% Paroxysmal symptoms Motor disorders Hemiparesis, lower paraparesis and monoparesis are common symptoms of MS Upper extremities are injured very seldom The typical signs of these symptoms are low muscle strength, the presence of pathological reflexes and low abdominal reflexes There are also changes of muscle tonus – spastic hypertonus, hypotonus or dystonus Hypotonus can be the sign of cerebellum and spinal cord posterior columns lesion Disorders of coordination Ataxia: Cerebellar dynamic and static ataxia Vestibular Sensitive Mixed Dysmetry, hypermetry Intention tremor Asynergy Dysmetry Finger-nose test Heel to knee test Kinds of ataxias: Kinds of ataxias: Multiple sclerosis (MS) PATOLOGICAL REFLEXES PATOLOGICAL REFLEXES Sensory disorders Subjective sensory disturbances are early signs of MS Then conductive sensory disorders are joined to them Muscle – joint sense usually suffers at the fifth year of the disease and later The loss of vibration sense points on posterior columns lesion Brain stem disturbances There is vestibular symptom with: dizziness nystagmus vestibular ataxia; Sometimes trigeminal pains are observed Visual and eye movements disorders The typical features of MS are: retrobulbar neuritis subatrophy of optic nerve disc decoloration of disc’s temporal part Eye movement disorders mean that there are syndromes of ophthalmoplegia Autonomic (pelvic) disorders Syndrome of m. Detrussor hyperreflexion. That means urine bladder inability to accumulate urine. The main symptoms are: micturition increased frequency of urination incontinence of urine retention of urine. Incomplete urine bladder emptiness. Dyssynergy of m. Detrussor and Sphincter. Nonspecific symptoms General weakness Cognitive disorders Memory Attention disturbances Behavioral disorders Depression, euphoria and fatigue syndrome Paroxysmal symptoms Tonic muscles spasm (painful and short lasting) Dysarthria and ataxia attacks Lermitt symtom – it is a short lasting feeling of electrical current along the spinal cord Paroxysmal trigeminal pains Atypical pains in extremities Paroxysmal itching Paroxysmal choreoatetosis Paroxysmal nystagmus Paroxysmal facial hemispasm Epileptic attacks (focal and general) Pains are very often observed at MS. They can be paroxysmal or chronic ones Uthoff’s symptoms – it is the worsening of patients state after the hot bathroom or hot meal Clinical forms Cerebral : cortical (epileptic attacks, psychiatric disorders) Visual brain stem cerebellar. Spinal: Cervical Thoracic lumbar – sacral pseudotabes. Cerebrospinal The course of the disease Acute Subacute Chronic: – remittent, - remittent – progressive - progressive – remittent - progressive The periods of the disease: Exacerbation Remission (complete, incomplete). Stable period MS degree: I – patient has difficulty to walk only after physical training II – patient has difficulty to walk and weakness on 2-3 km III – patient has spastic-paretic gait, difficulty to walk and weakness on 200-300 m. IV – patient can’t to walk without help V – patient can’t to walk or has blindness Клінічні прояви РС MS diagnosis Immune examinations of blood and CSF. Usually there are increased Ig G, M, A contents. Insignificant increasing of protein content and moderate pleocytosis in CSF Lymphocytosis, eosynophilia – in exacerbation stage; leukopenia, lymphopenia – in the period of remission. Increased thrombocytes aggregation and fibrinogen content. Increased Ig content in serum and decreased T – lymphocytes quantity. MRI To put veridical MS we have to reveal in patient at least 2 focuses of lesion and 2 exacerbations, or 2 exacerbations of 1 clinical focus and 1 paraclinical supposed focus. According to the accepted criteria there should be at least 3 focuses in MRI (2 of them should be located paraventricularly, 1 – subtentorialy (that means in brain stem or cerebellum). The diameter of focuses should be at least 6 mm, or there should be 4 focuses, 1 of them periventricularly. mri ЗМІНИ НА МРТ Method of evoked potentials This is a method that reveals bioelectrical brain activity in response to the stimulation. This method is not a specific one for MS diagnosis. Treatment Pathogenetical treatment Corticosteroids and ACTH Cytostatics and immune modulators, non specific immune suppressors Cytokines, interferones Antigen – specific immune therapy Corticosteroids and ACTH Prednisone is used orally 1 – 1.5 mg/kg/day twice a day during 10 – 14 days. Then during the next 2 months we decrease the dose gradually. One of the most popular schema for Methylprednisolone usage is 500 – 1000 mg per day i/v in 500 ml of physiological solution during 3 – 5 days. Then Prednisone is used in dose 0.5 – 1 mg/kg during 3 – 7 days with gradually decreasing of dose during the next 2 – 3 weeks. This way of usage has much more expressed and quick effectiveness and insignificant outside effects Dexamethasone is used i/v or i/m according to the schema – 8 mg per day during 7 days, 4 mg – 4 days, 2 mg – 3 days. It is used at retrobulbar neuritis The peculiarities of Corticosteroids usage: Long lasting and frequent usage is undesirable Usually H-2 blockers are used together with Corticosteroids ACTH has immune suppressive activity, inhibits cellular and humoral immunity. It is used in dose 40 – 100 U i/m during 10 – 14 days. Plasmapheresis is used in case of exacerbation. Cytostatics and immune modulators, non specific immune suppressors Asatioprine, Cyclophosfamidum, Cyclosporinum A. But all of these medicines have a lot of outside effects. The representatives of immune modulators are - T – activinum, Timalinum, Myelopid, Levamisolum. They are prescribed at progressive forms of MS. T – activinum is used in dose 100 mcg s/c every evening during 5 days, then 1 – 3 injections every 10 days. Timalinum is used in dose 10 mg i/m twice a day during 5 days, then every 10 days 2 injections are used. Interferones There are 3 types of Interferonum – α, β, γ. α - Interferonum has neither toxic nor treating activity. γ - Interferonum activates immune system and that’s why it provokes exacerbations. β - Interferonum inhibits production of γ – interferonum, increases activity of T – suppressors, has antiproliferative, antiviral and immune modulating properties. Rebif – is a modern human β – interferonum produced by “Serono” production. It is used in dose 6 – 12 mln s/c 3 times per week. It is one of the most effective modern medicines in MS patients, but unfortunately it is very expensive Antigen – specific immune therapy One of the representatives of these medications is Copaxone, made in Israel. Cost of treatment is about 7 000 $. It is used in dose 20 mg per day s/c during 6 – 24 months. It has selective immune modulating action. Basic therapy Vitamins B group Desensibilizative medicines Amino acids Nootrops ATP, Cocarboxylasa Biostimulants Entero and hemosorption Antiplatelet Antioxydants Angioprotectors Inhibitors of proteolytic enzymes Regeneration stimulants Symptomatic treatment Pelvis disorders Proserinum, Halantaminum decrease m. Detrussor hyperreflexion. α - Adrenoblockers decrease dysynergy of Sphincter and Detrussor. Spasticity Baclofen 5 mg 3 times per day Sirdalude 4 mg 3 times per day Tremor β - Adrenoblockers are used at postural tremor Clonasepam, Carbamasepam are used at intention Symptomatic treatment Hyperkinetic form Adrenoblockers Antidepressants Asthenia Psychostimulants Dopaminergic medicines Paroxysmal signs Carbamasepinum, Filepsin Acute multiple encephalomyelitis (AMEM) It is an infectious – allergic disease that is characterized by acute multiple lesion of the brain and spinal cord Clinical forms Encephalomyelopoliradiculoneuritis – it is the most common form of the disease, which is characterized by the lesion of all parts of nervous system. Polioencephalomyelitis – it is characterized by the lesion of CN’s nuclei and spinal cord gray substance. Opticoencephalomyelitis and opticomyelitis – are characterized by optic nerve neuritis and symptoms of lesion of brain and spinal cord. Disseminated myelitis – the spinal cord is damaged on different levels. Acute multiple encephalomyelitis (AMEM) Treatment Corticoids: Prednisolone and Methylprednisolone in dose 10 – 15 mg per kg i/v by drops per day. Later we can use it in pills 1.5 – 2 mg/kg every other day. Together with this medicine we prescribe anabolics , K, Ca, vitamin C. In acute stage we prescribe desensibilizating and dehydrating medicines. In case of severe bulbar disorders we include resuscitation measures. Plasmapheresis and vitamin B are also used. In residual period we prescribe massage, dibasol, KJ, biostomulants, Lidasa, Seduxen, sanatorium treatment.