Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
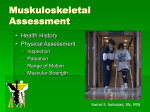
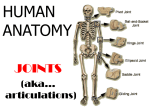
RHEUMATOID ARTHRITIS AND REHABILITATION Prof. Dr. Ülkü Akarırmak Rheumatic Diseases • Rheumatoid arthritis RA • Ankylosing spondylitis AS spondyloarthropathies • Osteoarthritis OA What is Rheumatoid Arthritis? RA is a chronic, systemic, inflammatory condition which: • • • • • Affects 1-2% of the adult population More common among women than men (2-3x) Highest incidence between ages 40 and 60 Causes pain, disability and loss of function Unwnown pathogenesis RA Background RA is a chronic autoimmune disorder Results from the interplay between an individual's genetic background and unknown environmental triggers Human leukocyte antigens (HLAs) account for ~30% of the heritable risk. Most of the genetic components are largely unknown RA – Etiology / Risk Factors • Genetics HLA – DR4 Sex Infection • Proteus, Mikoplazma EBV, Parvo, HTLV–1 Smoking Age Pathology • Synovial hyperplazia • Inflammatory cells • Increased joint fluid • Pannus • Invasive synovium • Erosion in bone and cartilage RA – Clinic • Morning stiffness • Arthritis – Sinovytis / Effusion Swelling • Structural changes • Loss of cartilage bone erosion periarticular lesions Joint Involvement in RA • Peripheral synovial joints • Hands and feet • Symmetrical • Especially hands • Wrist • MCP • PIP (+) • DIP (-) RA Deformities MTP Subluxation / Toe Deformities Atlantoaxiell Subluxation RA – X-Ray - Erosions 2010 ACR/EULAR Classification Criteria for RA JOINT DISTRIBUTION (0-5) 1 large joint 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) ≥6 = definite RA What if the score is <6? Patient might fulfill the criteria… Negative RF AND negative ACPA 0 Low positive RF OR low positive ACPA 2 High positive RF OR high positive ACPA 3 Prospectively over time (cumulatively) SYMPTOM DURATION (0-1) <6 weeks 0 ≥6 weeks 1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR 0 Abnormal CRP OR abnormal ESR 1 Retrospectively if data on all four domains have been adequately recorded in the past The Consequences of RA • Decline in functional status • Work disability • Co-morbidity • Increased mortality Rationale for Early Intervention • Some patients have early progressive disease • Joint damage begins within 6 months 1 year of onset • Disease modification thought to correlate with control of inflammation RA – Treatment • Early agressive treatment! • DMARD = “disease modifying anti–rheumatic drugs” • Combination therapy • Biologics – TNF- inhibitors, IL–1 antagonists, Anti–CD20, CTLA4 – Ig • NSAIDs • Glucocorticoid + Osteoporosis prevention + Pain medication RHEUMATOID ARTHRITIS MEDICATIONS • Medications are the cornerstone of treatment for active RA • The goals are to control inflammation, achieve remission, prevent further damage of the joints and loss of function • The type and intensity of RA treatment depends upon individual factors and potential drug side effects – follow-up DMARDs • DMARDs reduce inflammation of RA, reduce or prevent joint damage, preserve joint structure and function, and enable a person to continue ADL • DMARDs include methotraxate, hydroxychloroquine, sulfasalazine and leflunomide • Improvement in symptoms may require 4 – 6 weeks of treatment with methotraxate, 1 – 2 months with sulfasalazine. Even longer durations of treatment may be needed Biologic Agents • Biologics, are DMARDs • Biologics target molecules on cells of the immune system, joints, and the products that are secreted in the joint • There are several types of biologics • Biologics that bind TNF (anti-TNF agents or TNF inhibitors) include etanercept, adalimumab, infliximab, ertolizumab, tosilizumab and golimumab Biologic Agents • Biologics tend to work rapidly, within 2 and 4 to 6 weeks • Biologics may be used alone or in combination with other DMARDs (methotraxate), NSAIDs, and/or glucocorticoids or other biologics • All biologic agents must be injected (SC, IV) and patients have to be followed closely NSAIDs • NSAIDs are used to relieve pain and reduce minor inflammation. However, NSAIDs do not reduce the long-term damaging effects of RA on the joints • NSAIDs have significant side effects; GIS bleeding, fluid retention, increased risk of heart disease • The risks need to weighed carefully against the benefit Therapeutic Goals • Control of pain • Suppression of inflammation, CRP and the absence of swollen joints • Control of joint damage • Maintenance of normal ADL • Maximization of QOL Optimal Management Strategies • Early diagnosis • Early use of effective second-line agents, including, when required, the use of agents that act at different levels • Rest when joints are actively inflamed • Physiotherapy when inflammation is suppressed (multidisciplinary approach) Multidisciplinary Approach • Appropriate medical treatment • Bed rest during active disease • Splinting of actively inflamed joints • Pain control • Bone-sparing agents (for osteoporosis) The Rehab Team • • • • • • • • • Physiatrist Physiotherapist Occupational therapist Social worker Orthopedist Internalist Podiatrist Ophtalmolog Psychiatrist etc. Flare-up Periods • Resting • Splints • Positioning • Bed rest Deformities in RA Joint Deformity Position of Splinting Head and neck .Flexion, rotation . Full extension, cervical spine, chin forward Wrist Palmar flexion 30 degreees dorsiflexion Thumb Finger Hips . Knee Flexion Extension, apposition . Flexion, ulnar deviation Extension, no lateral deviation . Flexion,adduction, Extension, in line with body; external rotation . foot pointing upward Flexion Extension Splinting • Relieve pain • Relieve muscle spasm • Prevent deformity Involvement of the Lower Exremity Nonpharmacologic Therapy • Education program • Physiotherapy • Occupational therapy • Support from social workers Physical Therapy and Rehab • • • • • Effective in maintaining the ROM Strengthening of muscles Prevent contractures Prevent deformities Maintain ADL Physical and Occupational Therapy • • • • Preserve joint structure and function in RA The application of heat or cold can relieve pain or stiffness Ultrasound may reduce inflammation in tenosynovitis Passive and active exercises can improve and maintain ROM Rest and rest splinting can reduce joint pain and improve joint function Physical Therapy • Finger splinting and other assistive devices can prevent deformities and improve hand function • Podiatrist can make foot orthotics (devices for correct position of foot) and supportive footwear • Occupational therapists for active participation in work and recreational activity Physiotherapy Methods I - Exercises II- Cold treatment: During stages of acute inflammation III- Heating modalities: During subacute and chronic stages of the disease IV- TENS: Pain control V- Hydrotherapy Exercises I. Acute stage Aim: Preservation of ROM ROM and isometric exercises Subacute stage III. Chronic stage II. Cold TENS US Exercises II. Subacute stage III. Chronic stage Aim: Increasing strength and endurance Strengthening and endurance ROM exercises Stretching ROM Exercises/ Hydrotherapy Occupational Therapy • Education of patients in the use of ADL • Prevention of joint contractures and deformities Devices for ADL Management of Ankylosing Spondylitis • Rehabilitation • Exercises • Hydrotherapy Exercises in the Management of AS Posture ROM exercises Flexibility exercises & stretching Hip – Knee - Spine Respitatory Strengthening: Extensor / Core muscles Education • • • • • • • • Life style modification Exercises on a regular basis Posture awareness Swimming Spa Quit smoking Patient schools Secondary osteoporosis evaluation Q&A • Comments?