Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
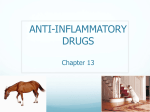
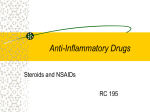
Rheumatoid Arthritis: A Chronic Inflammation By Catherine A. Olubummo, RN, MS, MSN, FNP Nursing made Incredibly Easy! November/December 2009 2.3 ANCC contact hours Online: www.nursingcenter.com © 2009 by Lippincott Williams & Wilkins. All world rights reserved. Definition An autoimmune disorder characterized by chronic symmetric inflammation of the synovial joints Often affects the wrist and finger joints closest to the hand, usually progressing from peripheral to more proximal joints A systemic disease with multiple extra-articular features, the most common of which are fever, weight loss, fatigue, anemia, lymph node enlargement, and Raynaud’s phenomenon When a chronic fluctuating course of the disease is experienced, it may result in joint destruction, deformity, disability, and premature death Prevalence RA is seen in all racial and ethnic groups Two to three times more likely to occur in women than men (70% of those diagnosed with RA are women) Although RA may affect any age group, peak onset of the disease is between ages 30 and 55 Patients with RA are said to be three times more likely to have been hospitalized for an acute heart attack; a recent study found that arthritis affects 57% of adults with heart disease Three Stages of RA Phagocytosis produces enzymes within the joint, which break down collagen, causing edema, proliferation of the synovial membrane, and pannus (inflammatory exudate) formation Pannus causes the synovium to thicken Cartilage is destroyed and bone erodes, leading to loss of articular surfaces and joint motion Pathophysiology Causes The etiology of RA remains unknown; however, most investigators believe that genetics, environment, and hormonal and reproductive factors are relevant Researchers have shown that people with the HLA genetic marker have a fivefold greater probability of developing RA Other more recently identified genes with a connection to RA include STAT4, TRAF1 and C5, and PTPN22 Other causes may include infectious agents such as bacteria and viruses and the body’s response to stressful events Signs and Symptoms Patients usually experience bilateral and symmetrical small joint involvement in the proximal interphalangeal and metacarpophalangeal joints Initial symptoms include: • tender, warm, swollen joints • morning stiffness, lasting more than 1 hour • weakness • malaise • fatigue • persistent low-grade fever • anorexia and weight loss Signs and Symptoms Chronic inflammation may lead to destruction of cartilage, bone, and ligaments, causing deformity of the joints Spontaneous remission is rare, although women with RA often experience remission when pregnant RA typically progresses to a chronic state associated with significant morbidity and functional disability The Effects of RA on Certain Joints Diagnostics There’s no single test for the disease Symptoms may differ in severity and can mimic those of other types of arthritis and joint conditions The presence of extra-articular features, such as weight loss, fever, anemia, serositis (inflammation of the serous tissues), carpal tunnel syndrome, and rheumatoid vasculitis, favors the diagnosis of RA Diagnosis will rely on a thorough medical history and physical exam, X-rays to show joint spacing and erosion, and lab tests Diagnostics Possible lab tests include: • complete blood cell count with differential • erythrocyte sedimentation rate and C-reactive protein • rheumatoid factor (present in 70% to 80% of patients with RA) • blood urea nitrogen and creatinine levels • hepatic panel (alanine aminotransferase, aspartate aminotransferase, and albumin) • synovial fluid analysis • hemolytic complement • antinuclear antibody titers The American Rheumatism Association Classification of RA Treatment Goals Overall treatment goals for RA are to control signs and symptoms, restore physical function, and prevent development of joint damage and disability If damage already exists, the goal is to halt the progression of the disease With advanced, unremitting disease, subsidiary goals are to relieve pain, improve joint motion, limit functional losses, incur a minimum of adverse reactions, and improve the patient’s sense of well-being and ability to function Nonpharmacologic Management Instruction in joint protection, conservation of energy, joint range of motion (ROM), and strengthening exercises is important Regular participation in exercise conditioning programs can greatly improve joint mobility, muscle strength, aerobic fitness, function, and psychological well-being, without increasing fatigue or joint symptoms Pharmacologic Management Primary goals of pharmacologic therapy for RA are relief of pain, reduction of inflammation, preservation of functional status, prevention of complications such as joint damage, and remission of the pathogenic process Pharmacologic therapy often consists of a combination of nonsteroidal anti-inflammatory drugs (NSAIDs), disease-modifying antirheumatic drugs (DMARDs), and glucocorticoids Biologic response modifiers, such as anti-tumor necrosis factor (TNF) alpha therapy and interleukin-1 receptor antagonist (IL-1RA) therapy, are also options NSAIDs Initial medical treatment of RA usually involves the use of NSAIDs such as aspirin or a selective cyclo-oxygenase-2 inhibitor (also known as a COX-2 inhibitor), to reduce joint inflammation and pain Patients taking anticoagulants or corticosteroids must avoid the use of NSAIDs due to an increased risk of bleeding Alternatively, simple analgesics may be considered in place of NSAIDs and DMARDs DMARDs All patients with RA are candidates for DMARD therapy The initiation of DMARD therapy shouldn’t be delayed beyond 3 months for any patient with an established diagnosis who, despite adequate treatment with NSAIDs, has ongoing joint pain; significant morning stiffness, fatigue, and active synovitis; persistent elevation of erythrocyte sedimentation rate and C-reactive protein levels; or radiographic joint damage For any untreated patient with persistent synovitis and joint damage, DMARD treatment should be started promptly to prevent or slow further damage DMARDs Common adverse reactions may include nausea, headaches, diarrhea, alopecia, leucopenia, and thrombocytopenia Patients receiving DMARD therapy must have routine kidney and liver function tests and urinalysis Patients must also be told to restrict alcohol intake Continuous monitoring of the number of swollen joints, duration of morning stiffness, and overall function will determine the drug’s efficacy Glucocorticoids Short-term, low-dose oral glucocorticoids are highly effective in relieving symptoms in active RA; patients will require close monitoring for adverse reactions Articular injections of a glucocorticoid are often used for persistent, erosive RA in single large joints Anti-TNF Alpha Therapy Administered by infusion, anti-TNF alpha drugs alter the natural progression of RA by inhibiting structural joint damage, such as bone erosion and joint space narrowing Monitor the patient’s pulse and BP every 30 minutes for early detection of potential infusion reactions and prompt intervention Patients with hypersensitivity to murine proteins or those who have moderate to severe heart failure shouldn’t receive anti-TNF alpha therapy Caution should be exercised in immunosuppressed patients and those with current infections; serious infections have occurred in patients treated with anti-TNF agents IL-IRA Therapy Anakinra subcutane has recently been approved by the FDA for treatment of RA It’s indicated to reduce signs and symptoms and slow the progression of structural damage for moderately to severely active RA in patients age 18 or older who haven’t received adequate relief with one or more DMARDs It can be used alone or in combination with DMARDs; this drug shouldn’t be used in combination with TNF antagonists because it increases the risk of infection IL-IRA Therapy Routine complete blood cell and platelet counts are recommended because neutropenia and thrombocytopenia have occurred in a small number of patients Headache, GI upset, and injection site reactions have been reported Live viruses shouldn’t be administered concurrently Patients with acute and chronic infections shouldn’t receive this drug Surgical Treatment Surgical treatments should be considered in patients who have untreatable pain, loss of ROM, or limitation in function due to joint damage Surgical procedures include tendon reconstruction, carpal tunnel release, synovectomy, resection of metatarsal heads, total joint arthroplasty, and joint fusion Patient Teaching Teach your patient about: • lifestyle modification, such as increased bed rest during flare-ups • use of adaptive aids to facilitate activities of daily living (such as raised toilet seats, special eating utensils, zipper pullers, and long-handled shoe horns) • prioritizing and planning activities to accommodate fatigue • use of splints for painful and swollen wrists and hands • the benefit of warm showers in the morning and frequent position changes to alleviate stiffness Patient Teaching Teach your patient about medication use, restrictions, and adverse reactions to report Warn her not to stop certain medications without notifying her healthcare provider Instructions should be given about dietary restrictions or recommendations as they relate to prescribed medications Advise her to discuss the use of any complementary or alternative therapies with her healthcare provider Patient Teaching During periods of remission, encourage your patient to exercise regularly Education concerning a regular aerobic and muscle strengthening exercise program is essential to help reduce stiffness, avoid joint contractures, and prevent osteoporosis The goal of exercise is to maintain ROM, strength, endurance, and mobility; improve general health; and promote well-being Patient Teaching Referral to a rheumatologist for diagnosis and treatment of RA is strongly recommended Referral to an orthopedic surgeon specialized in joint replacement should be considered for endstage joint disease Physical and occupational therapists should be consulted for exercise programs and adaptive devices Referral to a clinical psychologist or social worker may be beneficial Self-management programs, educational information, and exercise programs are available to patients at http://www.arthritis.org