Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
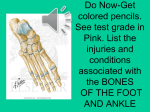
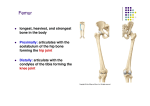
On September 18, 2013, 7 year old female patient X, was scheduled at Columbia Presbyterian Children Hospital for a follow up appointment, due to her undergoing right tibial lengthening 6 years prior. At birth, the patient was diagnosed with fibular hemimelia of her right lower extremity and at one year of age she was treated by surgical limb lengthening. Fibular hemimelia is a partial or total aplasia of the fibula, and is usually associated with other anomalies of the tibia, femur and foot. It represents the most frequent congenital defect of the long bones and is the most common skeletal deformity in the lower limbs. The anomaly is most often unilateral. The causes of Fibular hemimelia are unclear, although maternal viral infections, embryonic trauma, teratogen environmental exposures (drugs, radiation) or vascular dysgenesis (failure of the embryo to form a satisfactory blood supply) are considered possible causes. Hemimelia is usually not an inheritable condition. The majority of children born with this condition have no family history of this condition. The exception is when fibular hemimelia is present and is associated with other birth defects. In these cases, an extensive family history and possible genetic testing is required. The severity of the defect is variable with mild cases presenting simply as a shortening of one leg, whereas more severe cases involve a complete absence of the calf bone and bowing of the tibia. Children with fibular hemimelia have four main problems with their limb: Limb length discrepancy, foot and ankle deformities, knee deformity and deficient cruciate ligaments of the knee. The main symptoms associated with this anomaly are: shortened leg, deficient or absent calf bone, bowed tibia, knee and ankle instability. Treatment of fibular hemimelia varies from a simple shoe lift or bracing, to Syme amputation or gradual limb lengthening. The latter is mostly indicated for less severe cases with a relatively normal foot and ankle and is performed by the Ilizarov technique. The Syme amputation is the method preferred when extreme limb inequality is observed or when gross instability of foot and ankle is present and it is performed between ten months to 2 years of age. After amputation, the application of a highly functional below the knee prosthesis allows the patient to have a remarkable recovery. Lengthening requires numerous operations and sometimes leads to complications, whereas the amputated cases involve a single surgical procedure without notable complications. With both treatment options, the ultimate goal is to enable the child to gain maximum function by achieving adequate lower-extremity alignment, length, and stability. For a better understanding of the disease, a look at the anatomy and physiology of the tibia and fibula is in order. In human anatomy, tibia is the second largest bone, after the femur, and is recognized as the strongest weight bearing bone in the body. Tibia is the larger of the two bones of the lower leg, sitting next to the fibula, on the medial side of the leg, connecting the knee with the ankle bones. Primary ossification forms the long central shaft of the long bones called the diaphysis, while the secondary ossification, which occurs after birth, forms the epiphysis at both ends of the long bones. Near age 21, the epiphyseal plate that develops between the two areas becomes the epiphyseal line and full ossification occurs. The proximal tibia expands in the transverse plane with the medial and lateral condyles and the upper portion of the condyles contains the intercondylar eminence. The lower extremity of the tibia is smaller and on its medial side, the medial malleolus can be seen. The distal part of the tibia and fibula, together with the talus, forms the ankle joint. Fibula is the smaller of the two bones of the lower leg and it is located on the lateral side of the tibia. Its proximal extremity is placed toward the back of the head of the tibia, below the level of the knee, and excluded from the formation of this joint. Its lower extremity ends in the lateral malleolus forming the ankle joint. Fibula and tibia are connected thru the interosseous membrane, forming a syndesmosis joint. Diagnosis of the fibular hemimelia is based on clinical examination and X-rays. On September 18th, 2013, the patient received the following examinations for her regular follow up treatment: 3 projections of the right ankle (AP, oblique, and lateral), 2 projections of the right lower leg (AP and lateral), and 3 joint lower extremity exam. For the ankle examination, the patient was supine with the affected leg extended. The AP examination requires the foot to be dorsiflexed 90 degrees, the central ray is perpendicular to the ankle joint at a point midway between the malleoli. The oblique is obtained by medially rotating the foot approximately 15-20 degrees, adjusting the line between the malleoli to make it parallel to the IR. For the lateral view, the patient must turn toward the affected side, until the leg is laterally along the table, placing the patella perpendicular to the IR, dorsiflex the foot and direct the central ray perpendicular to the ankle joint, entering the medial malleolus. The technique utilized for the ankle exams was 55 Kvp and 4 mAs at an SID of 40 inches. The lower leg projections required the patient to remain in the supine position for the AP view, adjusting the femoral condyles so that they will be parallel to the IR with the foot dorsiflexed. The central ray is perpendicular to the mid shaft of the lower leg. The lateral projection is obtained by turning the patient onto the affected side with the femoral condyles perpendicular to the IR. The technique necessary for the lower extremity views was 55 Kvp at 4 mAs. For the 3 joint lower extremity projection, the patient is standing erect in the AP position, feet shoulder width apart and collimation is open to the level of the iliac crest down to the ankle joints. The technique used for the 3 joint lower extremity view was 60 Kvp and 5 mAs. Proper shielding was utilized during all examinations. No contrast medium is necessary for these projections, as the anatomy of interest is bone. The radiographic findings were the following: a solitary bone of the right lower leg; a single cannulated screw extending from medial malleolus to tibial shaft; talocalcaneal fusion is noted; indication of flatfoot deformity is observed; there is no fracture. The diagnostic erect 3 joint lower extremity clinical information consists of: left femur is approximately 11 mm longer than the right femur; the left tibia arises 2 cm higher than the right, but direct comparison between the tibiae is limited as the distal right tibia epiphysis is absent or dysplastic; prior plate and external fixator have been removed and mild residual irregularity in the bone density is noted; lucencies from wire hardware also seen in the proximal right tibia. All examinations were performed with a Philips DR imaging system, therefore no cassette is necessary. The follow up for this patient consists of regular checkups to review the progress of her right tibial lengthening which will ultimately allow her stability when standing and walking. In conclusion, our case deals with a young girl who at birth presented with the condition of fibular hemimelia, which in this particular incident was a complete absence of her right fibula. Her physician recommended tibial lengthening in order to correct the discrepancy between the right and left lower extremity. Surgery was performed at the age of one year in order to install the external fixator device so as to gradually lengthen the tibia. There will be an indeterminate number of follow up surgeries along with radiographic exams to both monitor and visualize the progress, until the expected outcome is achieved. References: Merrill’s Atlas of Radiographic Positioning S.Viquet, Carrin P.Garnero,P.D.Delmas- The role of collagen in bone strength Peter G. Bullough –Fibular Hemimelia Medicinenet.com Springer.com- Clinical Orthopedics and related research