Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of beta-blockers wikipedia , lookup
CCR5 receptor antagonist wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Toxicodynamics wikipedia , lookup
Drug discovery wikipedia , lookup
NMDA receptor wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Drug design wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug interaction wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
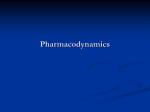
2004-2005 Module 2 #1 Pharmacodynamics Kash Desai 966-2723 HSc A120 [email protected] 2004-2005 Drug Receptors and Pharmacodynamics (how drugs work on the body) The action of a drug on the body, including receptor interactions, doseresponse phenomena, and mechanisms of therapeutic and toxic action. 2004-2005 2 Pharmacodynamics (how drugs work on the body) many drugs inhibit enzymes Enzymes control a number of metabolic processes A very common mode of action of many drugs in the patient (ACE inhibitors) in microbes (sulfas, penicillins) in cancer cells (5-FU, 6-MP) some drugs bind to: proteins (in patient, or microbes) the genome (cyclophosphamide) microtubules (vincristine) 2004-2005 3 Pharmacodynamics most drugs act (bind) on receptors in or on cells form tight bonds with the ligand exacting requirements (size, shape, stereospecificity) can be agonists (salbutamol), or antagonists (propranolol) receptors have signal transduction methods 2004-2005 Drug Receptor • A macromolecular component of a cell with which a drug interacts to produce a response • Usually a protein 2004-2005 Types of Protein Receptors 1. Regulatory – change the activity of cellular enzymes 2. Enzymes – may be inhibited or activated 3. Transport – e.g. Na+ /K+ ATP’ase 4. Structural – these form cell parts 2004-2005 5 dose response curves k1 [D] + [R] [DR] effect k -1 at equilibrium: k1/k-1 = affinity const. [D] x [R] x k1 = [DR] x k-1 k-1/k1 = dissociation const.(kd) so that: [DR] = k1 [D] [R] 2004-2005 k-1 the lower the kd the more potent the drug Drug - Receptor Binding D+R DR Complex Affinity Affinity – measure of propensity of a drug to bind receptor; the attractiveness of drug and receptor – Covalent bonds are stable and essentially irreversible – Electrostatic bonds may be strong or weak, but are usually reversible 2004-2005 Drug Receptor Interaction DR Complex Effect Efficacy (or Intrinsic Activity) – ability of a bound drug to change the receptor in a way that produces an effect; some drugs possess affinity but NOT efficacy 2004-2005 Isolated Muscle Contraction Drug-receptor interaction Arithmetic Scale 100 Percent Maximum Drug + Free Receptor 75 D (100 - DR) k1 k-1 Drug-receptor Complex DR 50 Where: 25 D = drug concentration DR= 0 concentration 0.00 0.25 of drug-receptor complex 0.50 0.75 1.00 Dose (ug/ml) 100 DR = free receptor concentration 2004-2005 Drug-receptor interaction • At equilibrium: [D] x [R] x k1 = [DR] x k-1 so that: [DR] = k1 [D] [R] k-1 k-1/k1 = dissociation constant (kd) 2004-2005 • At equilibrium: [D] x [R] x k1 = [DR] x k-1 so that: [DR] = k1 [D] [R] k-1 What can we learn? k-1/k1 = dissociation constant (kd) • Ke (k1/k-1) is called the affinity constant • DR is the response; D is concentration of drug • when DR = 50 percent (effect is half maximal), D (or EC50) is equal to kd or the reciprocal of the affinity constant • response is a measure of efficacy • drugs that have parallel dose-response curves often have the same mechanism of action 2004-2005 6 dose response curves-2 effect = [DR] = Emax * [D]/([D]+EC50) 2004-2005 % occupancy Concept: spare receptors Arithmetic Dose Scale • Rate of change is rapid at first and becomes progressively smaller as the dose is increased • Eventually, increments in dose produce no further change in effect i.e., maximal effect for that drug is obtained • Difficult to analyze mathematically 2004-2005 Log Dose Scale • transforms hyperbolic curve to a sigmoid (almost a straight line) • compresses dose scale • proportionate doses occur at equal intervals • straightens line • easier to analyze mathematically 2004-2005 Ethyl Alcohol: Arithmetic vs log Sleep scale of dose 30 20 10 0 0.1 0.31 % fall in blood pressure 40 Number Responding % fall in blood pressure 50 30 20 Control L-NAME 10 3 50 40 30 20 10 0 -2 10 Acetylcholine nmol/kg 0 5.28 5.40 -1 0 1 2 0.1 0.3 1 3 10 Acetylcholine nmol/kg 5.52 5.64 5.76 Dose (g/kg) 2004-2005 Control L-NAME 5.88 6.00 Potency Relative position of the dose-effect curve along the dose axis Has little clinical significance for a given therapeutic effect A more potent of two drugs is not clinically superior Low potency is a disadvantage only if the dose is so large that it is awkward to administer 2004-2005 Relative Potency hydromorphone morphine codeine Analgesia aspirin Dose 2004-2005 7 Why are there spare receptors? allow maximal response without total receptor occupancy – increase sensitivity of the system spare receptors can bind (and internalize) extra ligand preventing an exaggerated response if too much ligand is present The receptor theory assumes that all receptors should be occupied to produce a maximal response. In that case at half maximal effect EC50=kd. Sometimes, full effect is seen at a fractional receptor 2004-2005 occupation 10 Agonists and antagonists agonist has affinity plus intrinsic activity antagonist has affinity but no intrinsic activity partial agonist has affinity and less intrinsic activity competitive antagonists can be overcome 2004-2005 Agonist Drugs • drugs that interact with and activate receptors; they possess both affinity and efficacy • two types – Full – an agonist with maximal efficacy – Partial – an agonist with less then maximal efficacy 2004-2005 Agonist Dose Response Curves Full agonist Partial agonist Response Dose 2004-2005 Antagonist Drug • Antagonists interact with the receptor but do NOT change the receptor • they have affinity but NO efficacy • two types – Competitive – Noncompetitive 2004-2005 Competitive Antagonist • competes with agonist for receptor • surmountable with increasing agonist concentration • displaces agonist dose response curve to the right (dextral shift) • reduces the apparent affinity of the agonist i.e., increases 1/Ke 2004-2005 Noncompetitive Antagonist • drug binds to receptor and stays bound • irreversible – does not let go of receptor • produces slight dextral shift in the agonist DR curve in the low concentration range • this looks like competitive antagonist • but, as more and more receptors are bound (and essentially destroyed), the agonist drug becomes incapable of eliciting a maximal effect 2004-2005 11 Desensitization agonists tend to desensitize receptors homologous (decreased receptor number) heterologous (decreased signal transduction) antagonists tend to up regulate receptors 2004-2005 8 dose response curves-3 quantal dose response curves (used in populations, response is yes/no) Therapeutic index =Toxic Dose50/Effective Dose50 2004-2005 (TD50/ED50) DR Curve: Whole Animal • Graded – response measured on a continuous scale • Quantal – response is an either/or event – relates dose and frequency of response in a population of individuals – often derived from frequency distribution of doses required to produce a specified effect 2004-2005 Effectiveness, toxicity, lethality • ED50 - Median Effective Dose 50; the dose at which 50 percent of the population or sample manifests a given effect; used with quantal dr curves • TD50 - Median Toxic Dose 50 - dose at which 50 percent of the population manifests a given toxic effect • LD50 - Median Toxic Dose 50 - dose which kills 50 percent of the subjects 2004-2005 Quantification of drug safety Therapeutic Index = 2004-2005 TD50 or LD50 ED50 Drug A 100 sleep death Percent 50 Responding 0 ED50 LD50 dose 2004-2005 Drug B 100 Percent Responding sleep death 50 0 ED50 dose 2004-2005 LD50 9 The therapeutic index The higher the TI the better the drug. TI’s vary from: 1.0 (some cancer drugs) to: >1000 (penicillin) Drugs acting on the same receptor or enzyme system often have the same TI: (eg 50 mg of hydrochlorothiazide about the same as 2.5 mg of indapamide) 2004-2005 4 Signal transduction 1. enzyme linked (multiple actions) 2. ion channel linked (speedy) 3. G protein linked (amplifier) 4. nuclear (gene) linked (long lasting) 2004-2005 1. 2004-2005 G protein-linked receptors Structure: •Single polypeptide chain threaded back and forth resulting in 7 transmembrane å helices •There’s a G protein attached to the cytoplasmic side of the membrane (functions as a switch). 2004-2005 2. Tyrosine-kinase receptors Structure: •Receptors exist as individual polypeptides •Each has an extracellular signal-binding site •An intracellular tail with a number of tyrosines and a single å helix spanning the membrane 2004-2005 2004-2005 3. Ion channel receptors Structure: •Protein pores in the plasma membrane 2004-2005 Intracellular receptors Not all signal receptors are located on the plasma membrane. Some are proteins located in the cytoplasm or nucleus of target cells. • The signal molecule must be able to pass through plasma membrane. Examples: ~Nitric oxide (NO) ~Steroid (e.g., estradiol, progesterone, testosterone) and thyroid hormones of animals). 2004-2005 B. Second Messengers •Small, nonprotein, water-soluble molecules or ions •Readily spread throughout the cell by diffusion •Two most widely used second messengers are: 1. Cycle AMP 2004-2005 2. Calcium ions Ca2+ 2. Calcium Ions (Ca2+) and Inositol Trisphosphate •Calcium more widely used than cAMP •used in neurotransmitters, growth factors, some hormones •Increases in Ca2+ causes many possible responses: •Muscle cell contraction •Secretion of certain substance •Cell division 2004-2005 Two benefits of a signal-transduction pathway A. 1. Signal amplification 2. Signal specificity Signal amplification •Proteins persist in active form long enough to process numerous molecules of substrate •Each catalytic step activates more products then in the proceeding steps 2004-2005 2004-2005 12 Summary most drugs act through receptors there are 4 common signal transduction methods the interaction between drug and receptor can be described mathematically and graphically agonists have both affinity (kd) and intrinsic activity () antagonists have affinity only antagonists can be competitive (change kd) or non-competitive (change ) when mixed with agonists agonists desensitize receptors. antagonists sensitize receptors. 2004-2005