Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Drug discovery wikipedia , lookup
Methylphenidate wikipedia , lookup
Neuropharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
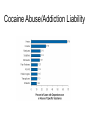
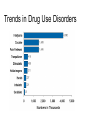
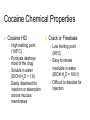
Cocaine, Stimulants, and MDMA ASAM’s 2008 Review Course in Addiction Medicine ACCME required disclosure of relevant commercial relationships: Dr. Drexler has nothing to disclose. Objectives The participant will be able to understand: How chemical structure of stimulants influences pharmacology Basic neurobiology of stimulant dependence How to recognize and manage acute stimulant intoxication and withdrawal Overview Background Stimulant- structure and pharmacology Neurobiology of stimulant addiction Management of acute intoxication and withdrawal Relapse Prevention Background Stimulants have been used by humans for thousands of years to increase energy. Plant-derived stimulants have been refined and new drugs developed to increase potency and duration. As potency increases negative effects become apparent. History of Stimulant Use 3000 B.C. – Ma-Huang 0 A.D. – Coca leaf chewing and coca tea 1860 – Cocaine isolated 1887 – Amphetamine synthesized 1914 – Harrison Narcotic Act MDMA 1919 – Methamphetamine 1930s – Benzedrine inhaler 1959 – Benzedrine banned 1980s – Crack Epidemiology Cocaine 2nd most widely used illicit drug in U.S. Most frequent illicit drug in ED visits In 2004 (NHSDA and DAWN) 11.2% lifetime use; 1.5% past year; 0.8% past month 2.7% lifetime prevalence of dependence 19% of drug-related ER visits 39% of drug-related deaths Cocaine Abuse/Addiction Liability Epidemiology Synthetic Stimulants Non-prescription use peaked at 1.3% in 1985 In 2004 (NHSDA) 6.6% lifetime non-prescription use 1.7% lifetime prevalence of dependence Methamphetamine Most commonly used synthetic stimulant In 2004, 59% of users had a use disorder Up from 27.5 % in 2002. Methamphetamine Lab Seizures Trends in Illicit Drug Use Trends in Methamphetamine Use Trends in Drug Use Disorders Club Drugs Epidemiology DAWN, July 2001 Overview Background Stimulant- structure and pharmacology Neurobiology of stimulant addiction Management of acute intoxication and withdrawal Structure and Pharmacology All stimulant drugs share a common basic phenylalkylamine structure. Additions to the phenyl group tend to increase hallucinogenic properties. Additions of a methyl group to the nitrogen atom tend to increase the stimulant properties. N OH OH Stimulant Drugs Plant-derived Caffeine Cocaine Ephedra Khat Synthetic Amphetamine Methamphetamine Methylphenidate Mazindol Phenylpropanolamine Ephedrine Pseudoephedrine Phenylephrine MDA / MDMA* Clinical Uses of Stimulants Drug Trade name Street name CSA Indications Amphetamine Adderal Dexedrine Amp, Dex Bennies II ADHD, Wt control Narcolepsy Coke, Crack Flake, Snow II Local anesthetic IV Wt control Cocaine Mazindol Sanorex Methamphetamine Adipex Desoxyn Ice, crystal II Meth, Speed ADHD Wt control Methylphenidate Ritalin Rits, Vit R ADHD Narcolepsy II Cocaine Chemical Properties Cocaine HCl High melting point (195°C) Pyrolysis destroys most of the drug Soluble in water (EtOH:H2O = 1:8) Easily dissolved for injection or absorption across mucous membranes Crack or Freebase Low melting point (98°C) Easy to smoke Insoluble in water (EtOH:H2O = 100:1) Difficult to dissolve for injection Stimulant Chemical Properties Most variations on phenylethylamine Phenylisopropylamine stimulants have stereoisomers D-isomers - 3 – 5 times more CNS activity D-methamphetamine – potent stimulant L-methamphetamine- OTC decongestant N OH OH MDMA Properties 3,4- Methylenedioxymethamphetamine Stimulant, hallucinogenic, empathogenic Taken orally as a pill 50 mg to 250 mg “Stacking” with other drugs (LSD, DM, ephedra) Non-linear kinetics Saturation of high-affinity enzymes Large increase in response to small dose increase Clinical Uses of Stimulants Prescription cocaine Local anesthetic Prescription stimulants ADHD Narcolepsy Weight loss Bronchdilation Depression, pain* Parenteral phenylephrine OTC stimulants Spinal anesthesia Antihypotensive Terminate SVT Decongestion Bronchodilation None for MDMA Methamphetamine Brand name: Desoxyn ADHD: 20 – 25 mg / day Obesity: 15 mg / day Binge: 125 mg – 1000 mg/dose Toxic doses*: 4- 6 mg/kg q2h (>3 gm/day) 37% loss of dopamine *Segal et al: 2003; Neuropsychopharmacology Pharmacokinetics Smoking and IV Reaches brain in 6 – 8 seconds Onset of action and peak occur in minutes Rapid decline in effect Rapid onset of withdrawal symptoms and craving Intranasal and oral Slower absorption and peak effect (30 – 45 minutes) Longer peak effect and gradual decline Peak intensity less than smoking or IV Alkalinization enhances absorption Pharmacokinetics Smoked Oral Metabolism and Elimination Cocaine Hydrolysis of ester bonds Amphetamines To metabolites Ecgonine methylester Benzoylecgonine Cytochrome P450 Eliminated in urine Benzoylecgonine detectable for ~3 days Acidifying s excretion Deamination- inactive Oxidation- active Parahydroxylationactive Eliminated in urine Increased by lower pH Drug Interactions Other stimulants- sympathetic activity Cardiac arrhythmia Hypertension Seizure Death MAOIs- inhibit metabolism of stimulants Tricyclics- may block presynaptic uptake Cocaine + EtOH = cocaethylene cardiac toxicity due to longer half-life Stimulant Effects Range of effects vary depending on Structure Dose Route of administration Duration and intensity of use Typical initial doses for desired effects: 5 to 20 mg of oral amphetamine, methylphenidate 100 to 200 mg of oral cocaine 15 to 20 mg of smoked cocaine 50 to 250 mg of MDMA Acute Stimulant Effects CNS Euphoria (low dose) energy, alertness sociability appetite Dysphoria (high dose) Anxiety, panic attacks Irritability, agitation Suspciousness Psychosis Movement disorders Seizures Cardiovascular HR, BP, vascular resistance, temperature Acute myocardial infarction (AMI), ischemia, arrhythmia Stroke Pulmonary Shortness of breath Bronchospasm Pulmonary edema Acute Stimulant Effects (cont) Musculoskeletal Rhabdomyolysis Acute renal failure secondary to myoglobinuria Ketoacidosis in diabetics Activation of HPA Increased arousal Prolonged erections Head and neck Endocrine Sexual function Renal Chronic rhinitis, nasal septal perforation Xerostomia Bruxism Fetal effects Most Category C Mechanisms of Action All stimulants enhance monoamine activity Inhibition of presynaptic monoamine transporters Dopamine – reward, psychosis Norephinephrine – physiological arousal Sertonin – mood elevation, psychosis OTC stimulants bind to and activate norepinephrine receptors Mesocorticolimbic Pathway Anterior cingulate Prefrontal cortex Nucleus accumbens Ventral tegmental area Dopamine (DA) Stimulants acutely enhance dopamine activity Cocaine, methylphenidate- transporter blockers Amphetamines- false substrates Stimulants chronically deplete dopamine DA activity key in mediating addictive potential Fluctuations in mesolimbic DA parallel cocaine selfadministration Stimulant potency correlates with potency for binding at DA transporter Cocaine Microdialysis in Awake Squirrel Monkeys Norepinephrine (NE) Stimulants acutely block NE transporter plasma NE and epinephine NE release correlates with subjective and physiological stimulant effects Ephedrine related compounds stimulate alpha-adrenergic NE receptors Serotonin (5-HT) All stimulants acutely enhance 5-HT activity by blocking serotonin transporter MDMA s 5-HT by blocking transporters Cocaine acutely s firing in mesolimbic serotonergic neurons, but s firing in dorsal raphe nucleus Serotonin appears to play a permissive, but not obligatory role in reward Other Neurotransmitters Endogenous opioid activity Mesolimbic glutamate Cocaine s Amphetamine s Acetylcholine No direct stimulant effect Cocaine indirectly s Cocaine s Sodium channel blockade (cocaine only) Overview Background Stimulant- structure and pharmacology Neurobiology of stimulant addiction Management of acute intoxication and withdrawal DSM-IV Substance Dependence >/= 3 of the following over a 12-month period: Tolerance Characteristic withdrawal Larger amounts than intended Persistent efforts to cut down or control use A great deal of time spent getting the substance, taking it, or recovering Important activities given up or reduced Continued use despite psychological or physical problem caused by or exacerbated by use Neurobiology of Dependence Sensitization of incentive salience Drug Conditioned cues Impairment of inhibition of urges to use Chronic effects of drug Signal transduction Gene transcription Mesocorticolimbic Pathway Anterior cingulate Prefrontal cortex Nucleus accumbens Ventral tegmental area Amygdala – Limbic Connections Nucleus accumbens Amygdala Prefrontal - Limbic Inhibition Orbitofrontal cortex Nucleus accumbens Cocaine craving-related neural activations: Men drug use - neutral Left Right insula -34 mm +34 mm anterior cingulate amygdala -19 mm +19 mm -9 mm +9 mm subcallosal cortex nucleus accumbens area Overview Background Stimulant- structure and pharmacology Neurobiology of stimulant addiction Management of acute intoxication and withdrawal Initial Evaluation of Stimulant Intoxication Drug history Physical examination Laboratory examination Manage basic life support functions T> 102°F – Cooling blanket T> 106°F – Cool saline hydration, ice water lavage Remove drug from GI tract Activated charcoal or gastric lavage If within one hour of ingestion Management of Severe Agitation Benzodiazepines- first line Protect against CNS and cardiovascular toxicity Lorazepam 2 – 4 mg PO or IV q 15 min until sedate Repeat every 1 – 3 hours Antipsychotics- second line May prevent heat dissipation, lower seizure threshold, prolong QTc, increase dyskinesias Haloperidol 2 to 10 mg PO, IM or IV q 6 – 24 hours Avoid physical restraints Cardiovascular Effects of Stimulants Myocardial ischemia is common. Vasoconstriction Increased myocardial workload Increased platelet aggregation Differential - AMI, aortic dissection, pneumothorax, endocarditis, or pneumonia Arrhythmias Due to ischemia, catecholamines, or sodium channel blockade Management of Chest Pain Observe for 12 – 24 hours ECG Cardiac enzymes: Low sensitivity (36%) Low predictive value (18%) Serial CPK- MB or troponin ~ 15% of patients with stimulant-induced chest pain will have AMI. Management of Arrhythmias Treat underlying conditions AMI Electrolyte and acid-base abnormalities Hypoxia Many will resolve without treatment Avoid Class I antiarrhythic drugs Follow ACLS guidelines Management of Seizures Benzodiazepines Lorazepam 2 to 10 mg IV over 2 minutes Diazepam 5 to 10 mg IV over 2 minutes Repeat as needed Monitor respirations, intubation available Management of Rhabdomyolysis Diagnosis requires high suspicion Muscle swelling and myalgia often absent Plasma CK > 5 times normal Urinalysis positive for heme without RBCs IV hydration – urine output 2 ml/kg/hour Urine pH > 5.6 – sodium bicarbonate Management of Hypertension Benzodiazepines first line Lower myocardial oxygen demand Lower seizure risk* If severe hypertension persists Alpha-adrenergic blocker Phentolamine 2 to 20 mg IV over 10 min No beta-adrenergic blockers Unopposed alpha stimulation s vasoconstriction DSM-IV Cocaine Withdrawal A. Cessation of (or reduction in) cocaine use that has been heavy and prolonged. B. Dysphoric mood and two (or more) : Fatigue Vivid, unpleasant dreams Insomnia or hypersomnia Increased appetite Psychomotor retardation or agitation Management of Withdrawal Most symptoms resolve within 2 weeks without treatment Hospitalization for suicidality or psychosis Pharmacologic treatment not necessary Relapse Prevention Psychosocial treatment Cognitive behavioral therapy (CBT) Contingency management (MIEDAR) 12-step facilitation- ? Motivation Enhancement Therapy- ? MATRIX model Treat comorbidities Pharmacotherapy No FDA approved medications Antidepressants Dopaminergic agents Disulfiram Anticonvulsants (GVG, topiramate) Disulfiram Patients Have Less Cocaine Use Carroll et al, 2004 Modafinil Decreases Cocaine Use Dackis 2005 Summary Stimulants are common causes of drug-related morbidity and mortality. Chemical structure of stimulants relates to the pharmacologic properties. Neurobiology of stimulant addiction is related to blockade of monoamine transporters. Management of acute intoxication and withdrawal is symptom driven. Relapse prevention is based on comprehensive biopsychosocial treatment.